

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Maternal blood glucose transfers to the fetus with a passive process utilizing facilitative glucose transporters and it is one of the important sources for fetal growth. Therefore, a concentration gradient between fetal and maternal circulation is needed to have good nutrient support for the fetus. However excessive maternal glucose is known to cause maternofetal complications including pregnancy loss, macrosomia, preeclampsia, shoulder dystocia, and cesarean section12 and future metabolic impact in the offspring.34 Despite numerous studies, the threshold for high blood sugar that defines women at increased risk of adverse outcomes is still controversial in screening and diagnostic tests.5 Nevertheless, blood sugar above the threshold needs to be detected and controlled to reduce perinatal complications.
Preconception counseling is one of the essential steps in preparing for a healthy pregnancy and its role has been proven to be effective to decrease adverse pregnancy outcomes. One of the feasible steps for preconception counseling is to measure fasting glucose in the blood. There have been several studies evaluating antenatal fasting glucose levels and their impact on pregnancy outcomes.4567 All demonstrated the utility of fasting glucose for the prediction of gestational diabetes, preterm birth, or large for gestational age (LGA). Although there is still debate on which levels of glucose need to be controlled, glucose control even in mild hyperglycemia during pregnancies, proved to improve outcomes.89
Little is known about the impact of fasting glucose within the normal range before pregnancy on pregnancy outcomes. It is therefore of value to provide data regarding prepregnancy fasting glucose within normal range. In this study, we used large population cohort and examined prepregnancy fasting glucose within normal range and its influence on adverse pregnancy outcomes in a subsequent pregnancy.
METHODS
Health care delivery system in Korea
Most of the Korean population has followed the national health insurance policies and medical problems have been covered by the Korea National Health Insurance (KNHI) except non-insured medical problems such as cosmetics. Therefore, KNHI contains approximately 50 million Koreans and all information about the disease and treatment can be retrieved from this centralized database. Under this system, all subscribers are required to participate in the biannual national health screening examination (NHSE), free of charge.
As part of the KNHI health-care system, a national health-screening program for infants and children, 4–80 months of aged human go through health exam which consists of information on gender, preterm birth, and birth weight.
Study population
We identified all women who had deliveries between January 1, 2007, and December 31, 2010. Of these, only those who had NHSE within 6 months prior to pregnancy and who attended a national health-screening program for infants and children after delivery were included. Women with a diagnosis of pregestational diabetes, fasting glucose ≥ 126 mg/dL, multiple pregnancies, and preterm birth and whose data were missing were excluded.
Assessment of obstetric outcomes
Following seven groups stratified by prepregnancy fasting glucose levels (< 75, 75–79, 80–84, 85–89, 90–94, 95–100, and > 100 mg/dL) were used. The primary outcome was overall obstetric complications The International Classification of Diseases, tenth revision (ICD-10) was used to identify pregnancy induced hypertension (HTN) and gestational diabetes from the KNHI Claims Database. Preterm birth was defined as gestational age < 37 weeks, low birth weight (LBW) was defined as birth weight < 2,500 g, and macrosomia was defined as birth weight > 4,000 g.
NHSE health examination included the body mass index (BMI) (kg/m2) and blood pressure (BP). BP was measured using a standard mercury sphygmomanometer. All blood samples were obtained after a minimum fast of 8 hours. The levels of fasting glucose, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) were measured with a Hitachi 747 Autoanalyzer (Hitachi Instruments Inc., Tokyo, Japan), using enzymatic methods.
Statistical analysis
Data are presented as mean ± standard deviation for continuous variables, and percentage for categorical variables. Clinical and biochemical characteristics were compared between groups using the ANOVA for differences in continuous variables, and the χ2 test for categorical variables. Multivariate logistic regression analysis was used to estimate the adjusted odds ratio (OR) and 95% confidence interval (CI) for the development of pregnancy induced HTN, gestational diabetes, macrosomia, and LBW. All tests were two-sided, and a P value < 0.05 was considered statistically significant. Statistical analyses were performed using SAS for Windows, version 9.4 (SAS Inc., Cary, NC, USA).
RESULTS
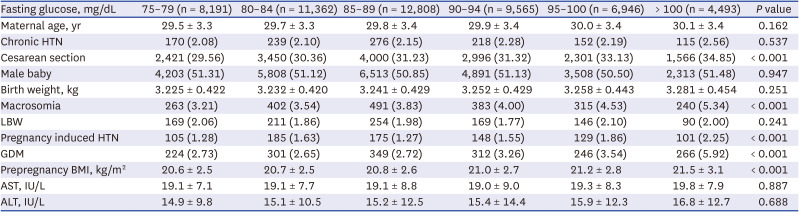
A total of 57,619 women who delivered in South Korea from January 1, 2007 and December 31, 2010, were eligible for analysis. The number of women with fasting glucose < 75 mg/dL was 6,254 (20.4%) and > 100 and < 126 mg/dL was 4,493 (7.5%) (Table 1). Among seven groups stratified by fasting glucose 5 mg/dL, there were no differences in maternal age, birthweight, and prepregnancy AST and ALT. The number of prepregnancy HTN, male sex, and LBW demonstrated no significant differences. The rate of cesarean section, macrosomia, pregnancy induced HTN, and gestational diabetes significantly increased as prepregnancy fasting glucose levels increased. Prepregnancy BMI was positively associated with higher prepregnancy fasting glucose (Table 1).
Table 1
Prepregnancy and pregnancy characteristics of the study population according to prepregnancy fasting glucose levels
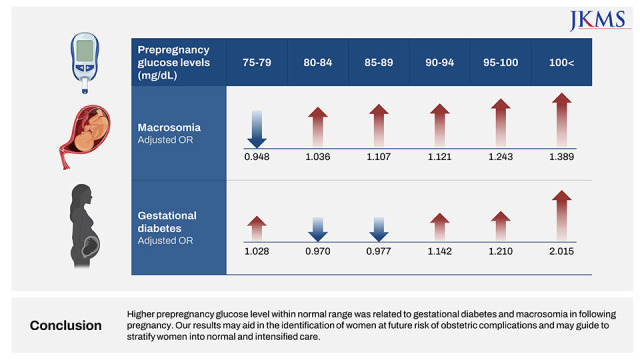
The adjusted ORs are shown in Table 2. Compared with women with prepregnancy fasting glucose less than 75 mg/dL, women with prepregnancy fasting glucose 90–94, 95–100, and > 100 had a higher risk of macrosomia (ORs [95% CI]; 1.121 [0.944–1.332], 1.243 [1.039–1.487], 1.389 [1.147–1.682]) and gestational diabetes (ORs [95% CI]; 1.142 [0.942–1.385], 1.210 [0.989–1.480], 2.015 [1.649–2.462]). Compared with women with prepregnancy fasting glucose less than 75 mg/dL, women with prepregnancy fasting glucose ≥ 100 mg/dL and < 126 mg/dL had a higher risk of pregnancy induced HTN (ORs [95% CI]; 1.240 [0.933–1.648]).
Table 2
Risk of pregnancy outcomes according to prepregnancy fasting glucose level

DISCUSSION
This is the first population based study that elucidated different levels of prepregnancy fasting glucose within normal range and its influence on perinatal outcomes in a subsequent pregnancy. We found that above 90 mg/dL of prepregnancy fasting glucose within the normal range was associated with the risk of macrosomia and gestational diabetes even after adjustment for maternal age and BMI.
There have been three studies on prepregnancy glucose levels on perinatal outcomes however these studies mainly focused on the impact of impaired fasting glucose (IFG) which is between > 100 and < 126 mg/dL compared to normal glucose levels ≤ 100 mg/dL. One study addressed prepregnancy impaired fasting glucose and its relationship to abnormal oral glucose tolerance test results and gestational diabetes.10 A prospective study examined the relationship between prepregnancy maternal factors and obstetric outcomes that fasting blood sugar of more than 6.1 mmol/L (108.9 mg/dL) was associated with increased preterm birth after adjustment.11 Another recent study on prepregnancy IFG was a retrospective cohort study what revealed IFG increased the risk of preterm birth, LGA and severe LGA.12
In our study, prepregnancy fasting glucose between 90 mg/dL and 100 mg/dL is associated with the risk of macrosomia and gestational diabetes even after adjustment of maternal age and BMI. The risk is linearly increased as the glucose level increased. In line with our work, a previous risk prediction model for severe gestational diabetes mellitus (GDM) in Korea population observed that the risk of GDM with prepregnancy fasting glucose 90 to 99 mg/dL was 1.8 times higher than < 90 mg/dL.13
Some factors are likely to be implicated in increased risk of macrosomia and gestational diabetes even in normal fasting glucose levels. Maternal glucose levels are linearly related to birthweight.14 Our result raises the possibility that threshold for impaired fasting glucose level to predict macrosomia may need to be changed. There is still debate on uniform worldwide optimal cut-off point for impaired fasting glucose. Further prospective studies on the cutpoint of impaired fasting glucose or hyperglycemia are needed.
The plausible biological theory related to clinical implications of the findings reported herein may be explained by preconception injury followed by exposure to maternal glucose. Prior to conception, it is believed that exposure has already been made before the implantation through defects in the mitochondria of oocyte which meets with sperm and becomes an embryo. An embryo with impaired metabolism eventually affects abnormal fetal growth.15 Slight alteration in endocrine function may influence a women’s facing diabetogenic challenges of pregnancy, and thereby increase macrosomia and gestational diabetes. Physiologic event of pregnancy is elevated glucose tolerance in order to transfer enough glucose to fetus for appropriate fetal growth. As the glucose levels increases in mother’s blood and it readily cross placenta without mother’s insulin, fetus respond to this phenomenon by secretion of insulin from fetal pancreas. This hyperinsulinemia plus hyperglycemia lead to an increase in the fat and protein stores, resulting macrosomia. In addition to an embryo with impaired metabolism, this phenomenon predispose to higher macrosomia or gestational diabetes risk even in normal glycemic control.
With the aging of pregnant women and the increase in high-risk pregnancies in recent years, pre-pregnancy management is drawing attention as it is important. Previous metanalysis revealed that lifestyle interventions was associated with lower incidence of LGA babies and neonatal adiposity.16 Another metaanalysis further concluded that lifestyle interventions before 2nd trimester could prevent gestational diabetes.17 The present study found the relationship between the prepregnancy fasting glucose within normal range and the risk of gestational diabetes and macrosomia. Fasting glucose check before pregnancy would help to identify who would benefit from lifestyle modification and this early intervention will lead to improve maternal and neonatal health by decreasing gestational diabetes and macrosomia.18 Although prospective studies should be conducted to define cutoff of fasting glucose level before pregnancy for gestational diabetes and macrosomia, it is thought that prepregnancy management including controlling blood sugar may be more effective in preventing gestational diabetes and macrosomia than in early pregnancy.
The major strength of this study is large population cohort and the first study to examine the relationship between prepregnancy fasting glucose levels within normal range and obstetric outcomes. However there are several pitfalls. First our results might not be generalizable because Asian population was only assessed. Second, the diagnosis of gestational diabetes, pregnancy induced HTN and chronic HTN are based on ICD-10 codes from insurance claims data. The diagnosis was not validated in each individual patient data and there is a limitation that it may not be an accurate diagnosis. Third, influential factors for gestational diabetes and macrosomia such as socioeconomic and nutritional status, excessive maternal weight gain, healthcare compliance and access to medical facilities could not be assessed with this insurance claims data. Last, different screening and diagnostic method on gestational diabetes might be used in different hospitals (e.g. NDDG vs. Carpenter Coustan, one step (75 g oral glucose tolerance test [OGTT]) vs. two steps (50–100 g OGTT). In addition, the insurance claims data does not contain the results of HbA1c, a marker for glycemic control.
For the first time, we have uncovered a potential link between normal fasting glucose levels prior to pregnancy and the development of gestational diabetes, as well as macrosomia. The risk of developing gestational diabetes and macrosomia increases as blood glucose levels rise. As the pregnant women continue to age, the number of high-risk pregnancies, including those involving gestational diabetes, is expected to rise. To combat these adverse outcomes, it is essential to perform a thorough risk assessment before pregnancy and take preventive measures. This proactive approach will ultimately help reduce the occurrence of complications related to gestational diabetes and macrosomia. It is crucial for healthcare providers to educate women who are planning to become pregnant about the significance of managing their blood sugar levels, particularly those with IFG levels prior to pregnancy.
 XML Download
XML Download