

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Osteoporosis and bone fracture are linked to inflammatory bowel disease (IBD);1234 several possible mechanisms can explain these. Corticosteroids, a mainstay treatment of active IBD, may affect bone loss and demineralization.5 A recent Swedish nationwide cohort study revealed that cumulative corticosteroid dosages in individuals with > 4,500 mg prednisolone equivalents increased hip and fracture risk in patients with IBD.6 Vitamin D, an important factor in calcium metabolism and healthy bone development, is commonly deficient in patients with IBD.7 Important bone metabolism and mineralization components may become unbalanced because of chronic inflammation.89
The aging of the population with IBD may increase the risk of concomitant conditions such as fractures.10 The mechanisms of fractures vary according to different age groups. In addition to skeletal variables, lifestyle and risk-taking behavior may influence fracture risk because children and adolescents are prone to fracture their bones while playing, participating in sports, or in accidents.1112 In adults and older women, bone aging, such as frailty, changes in soft tissue composition, and reduced bone strength, may be more closely related to fractures.13 Previous data from Olmsted County, Minnesota, showed that younger individuals (aged 18–49 years) had a higher percentage of fracture of hands and feet and fewer fractures at conventional osteoporotic fracture sites, including the vertebra and hip, than older inhabitants (age ≥ 50 years).12 These differences may be observed in populations with IBD, where aging might contribute to the risk of fractures.
Recently, several epidemiologic studies reported that IBD increases the risk of fractures.614 However, most of these studies have primarily focused on corticosteroid use as a risk factor for fractures, and there is a lack of information regarding the fracture risks and associated factors related to comorbidities and lifestyle habits in IBD patients who are particularly vulnerable to age-related osteoporotic changes. Therefore, the objective of our study is to examine the fracture risk and factors associated with comorbidities and lifestyle in IBD patients who are susceptible to age-related osteoporotic changes. We investigate the fracture risks in middle-aged and older Korean patients with IBD and analyzes the impact of comorbidities and lifestyle habits on the risk of developing fractures using population-based data.
METHODS
Data source
In Korea, the National Health Insurance Service-National Health Information Database (NHIS-NHID) covers all claims data, including the International Classification of Disease (ICD) codes and rare intractable disease (RID) enrollment programs; researchers have access to information on treatment prescriptions and specifics of nationwide medical examinations of the entire population.1516
This retrospective population-based cohort study used the NHIS-NHID. Approximately 97% of the enrolled Korean population, who are subjected to semi-required medical examinations every two years, are represented in the database. The NHIS database contains information on a person’s demographics, hospitalization, outpatient medical usage, drug use, medical interventions, and diagnoses denoted by the ICD, Tenth Revision (ICD-10) codes. Also, the national medical examinations included the data of lifestyle behavior questionnaire such as alcohol consumption, smoking, and exercise. The NHIS has established a program for enrolling patients with RIDs to improve medical reimbursement by lessening the economic strain of treating RIDs such as IBD. Trained physicians must determine if the disorders match the diagnostic standards for each RID to enroll individuals with RIDs in this program. A specific diagnostic code (V code), in addition to the ICD-10 code, is assigned upon registration in the RID program. Only patients with IBD who meet stringent comprehensive diagnostic requirements, such as imaging, histological, clinical, and endoscopic findings, are given the V code.
Study population
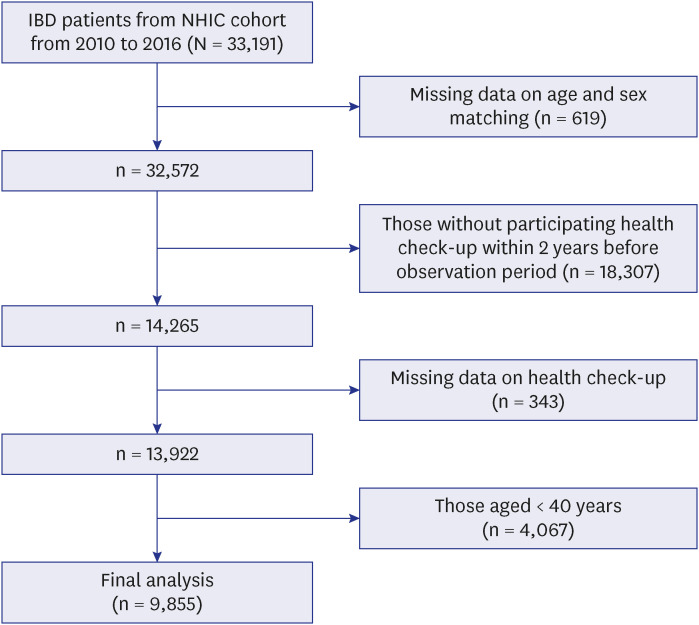
A total of 33,191 patients with IBD were included in this study. These patients were newly registered in the NHIS database with both ICD-10 and V codes from January 2010 to December 2016. To ensure the accuracy of the incidence rates (IRs), a washout period from 2002 to 2009 was implemented. During the process of identifying newly diagnosed IBD cases in 2010, patients who had been previously diagnosed with IBD between 2002 and 2009 were excluded from the analysis. ICD-10 K50 and V130 codes were used to identify patients with Crohn’s disease (CD), whereas the K51 and V131 codes were used to identify patients with ulcerative colitis (UC). Additionally, data were obtained from 14,265 patients with IBD who underwent an NHIS medical examination biannually between 2008 and 2014 and whose medical records were reviewed. Of these patients, 343 were eliminated because of missing values, such as laboratory test results. Finally, 9,855 individuals aged > 40 years were included in the study (Fig. 1). As a control group, 40,193 individuals without IBD were randomly selected and matched by age and sex at a 1:4 ratio. Participants in the study were monitored until fracture occurrence, censoring (such as death), or the final follow-up date (December 31, 2017), whichever occurred first. The mean follow-up period was 3.02 years with a standard deviation of 1.97 years. The median follow-up period was 2.77 years, with an interquartile range of 1.32–4.62 years.
Outcome: fractures
ICD-10 codes for fractures were as follows: vertebral (S22.0, S22.1, S32.0, M48.4, and M48.5), hip (S72.0 and S72.1), and other fractures, including the upper arm (S42.0, S42.2, and S42.3), forearm (S52.5 and S52.6), and lower leg (S82.3, S82.5, and S82.6).141718 Vertebral or other fractures were considered to have occurred when there were two or more outpatient visits during 12 months with the appropriate diagnosis codes. Hip fracture was defined as one hospitalization with an appropriate diagnostic code. ‘Other fractures’ was classified when individuals experienced at least one of the upper arm, forearm, or lower leg fractures.19
Covariates
A standardized self-reported questionnaire and information obtained from the medical examination were used to collect covariates for multivariate analysis. Demographic data including age, sex, place of residence, income level, cigarette smoking (never, former, and current), alcohol consumption (none, mild, and heavy), regular exercise (no, yes), body mass index (BMI), glomerular filtration rate (GFR), previous fracture history within five years in both the IBD and non-IBD groups were collected. We also collected information on comorbidities, including hypertension (defined as ICD-10 codes (I10–13, I15) with antihypertensive agents), diabetes mellitus (DM; defined as ICD-10 codes (E11–14) with antihyperglycemic agents), and dyslipidemia (defined as ICD-10 code (E78) with antihyperlipidemic agents), as described previously.2021 Individuals whose alcohol consumption was < 30 g per day were defined as mild drinkers, and individuals whose alcohol consumption was > 30 g per day were defined as heavy drinkers.22 Regular exercise was based on the frequency and intensity of activity per week. Obesity was defined as a BMI cutoff of 25 kg/m2.23 Chronic kidney disease (CKD) was defined based on the GFR, as estimated by the Modification of Diet in Renal Disease equation. The following GFR categories were recognized: ≥ 60, 30–60, and < 30 mL/min/1.73 m2.
Statistical analysis
Baseline participant characteristics were calculated using numbers and percentages for categorical variables and means and standard deviations for continuous variables. The χ2 test for categorical variables and the t-test for continuous variables were used to compare the characteristics of the groups. The IR was calculated based on the prevalence of the outcome per 1,000 person-years (PY) from the total fracture events and PY in each group.
Using Cox proportional hazards regression models, hazard ratios (HRs) and 95% confidence intervals (CIs) were computed relative to the reference to evaluate fracture risk in patients with IBD, and the association between fracture risk and comorbidities or lifestyle variables.
Subgroup analyses stratified by age, sex (male and female), obesity (< 25 and ≥ 25 kg/m2), cigarette smoking (current smoker or non-smoker), current alcohol consumption (none or heavy), regular exercise (no or yes), and comorbidities (diabetes, hypertension, and dyslipidemia) were conducted. Unadjusted HRs were assessed using Model 1 to evaluate the association between fracture risk and comorbidities or lifestyle habits. Adjusted HRs (aHRs) were calculated as Model 2 (adjusted for age and sex), Model 3 (adjusted for Model 2 + DM, hypertension, dyslipidemia, place of residence, income level, and previous fracture within five years), and Model 4 (adjusted for Model 3 + current smoking, alcohol consumption, regular exercise, BMI, and CKD). The Kaplan-Meier analysis and log-rank test were used to examine the cumulative incidence of fractures in the IBD and non-IBD groups. Statistical significance was set at P < 0.05. All statistical analyses were performed using the SAS software (version 9.3; SAS Institute, Cary, NC, USA). Two-sided P values< 0.05 were considered to indicate statistical significance for all analyses.
RESULTS
Baseline characteristics of the study population
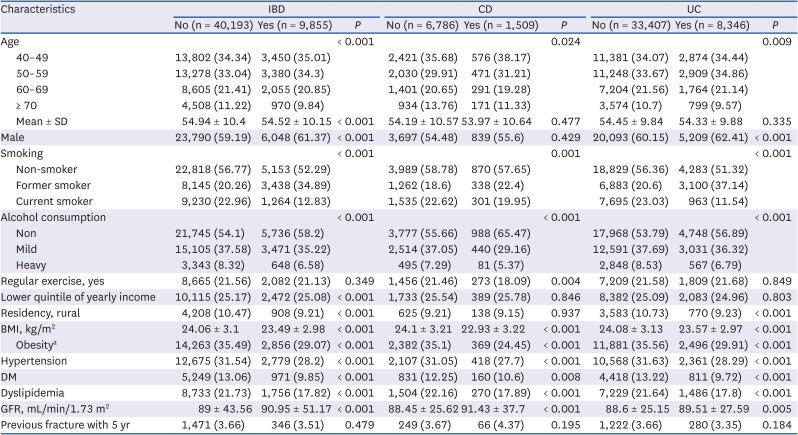
The baseline characteristics of the study participants are summarized in Table 1. The mean age was 54.5 years, and 61.4% were male in the IBD group. The IBD cohort had a lower mean age and a higher proportion of males than the non-IBD controls (P < 0.001, respectively). Compared with the non-IBD group, the IBD cohort had a reduced percentage of rural residents (P < 0.001) and individuals with income levels below 25% (P < 0.001). When compared with controls, the IBD cohort had a significantly decreased prevalence of DM (P < 0.001), hypertension (P < 0.001), and dyslipidemia (P < 0.001). There was no difference in the previous fracture rate within five years between the two groups.
Table 1
Baseline characteristics of the study participants
Risk of fractures in patients with IBD
Despite adjustment for age, sex, place of residence, income level, history of the previous fracture within five years, comorbidities like DM, hypertension, and dyslipidemia, and lifestyle habits such as smoking, alcohol consumption, and regular exercise, the HR indicated that the risk of total fracture was significantly higher in the IBD group than that in the non-IBD group. Similar trends were observed in the UC and CD cohorts (Table 2). Additionally, the cumulative incidence of fractures in the IBD group was significantly higher than in the non-IBD group (P = 0.008, Fig. 2A).
Table 2
Risk of fracture in patients with IBD
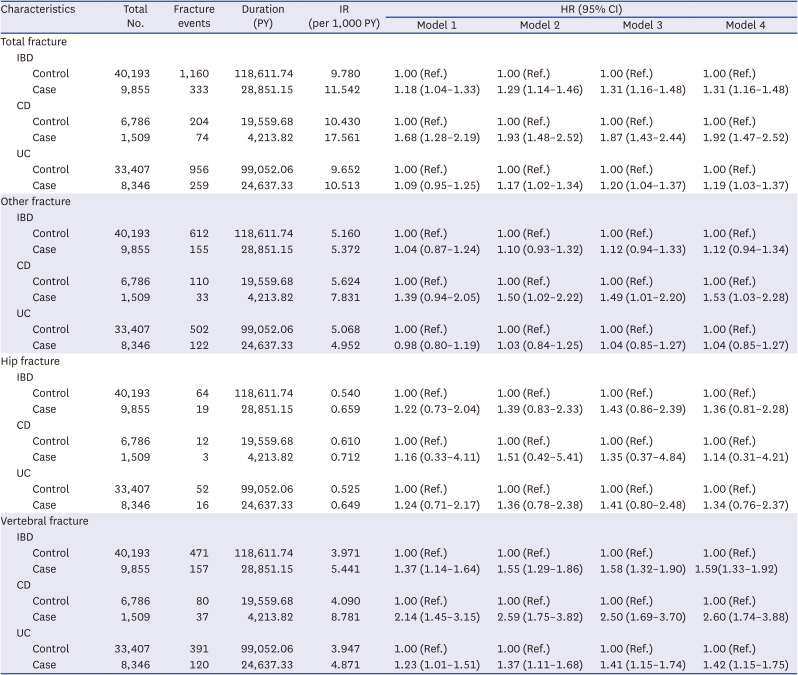
Model 1: unadjusted analysis. Model 2: adjusted for age and sex. Model 3: adjusted for Model 2 + place of residence, income level, diabetes mellitus, hypertension, dyslipidemia and previous fracture within 5 years. Model 4: adjusted for Model 3 + body mass index, chronic kidney disease, current smoking, alcohol consumption and regular exercise.
CD = Crohn’s disease, CI = confidence interval, HR = hazard ratio, IBD = inflammatory bowel disease, IR = incidence rate, PY = person-years, Ref. = reference, UC = ulcerative colitis.
Fig. 2
Kaplan-Meier plots show the cumulative incidence of fractures in patients with IBD, CD and UC. (A) Total fractures. (B) Vertebral fractures. (C) Hip fractures. (D) Other fractures.
IBD = inflammatory bowel disease, CD = Crohn’s disease, UC = ulcerative colitis.
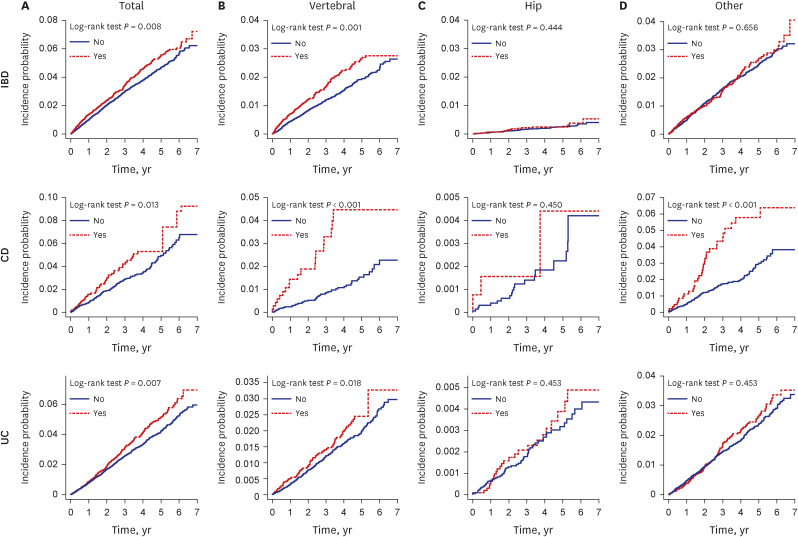
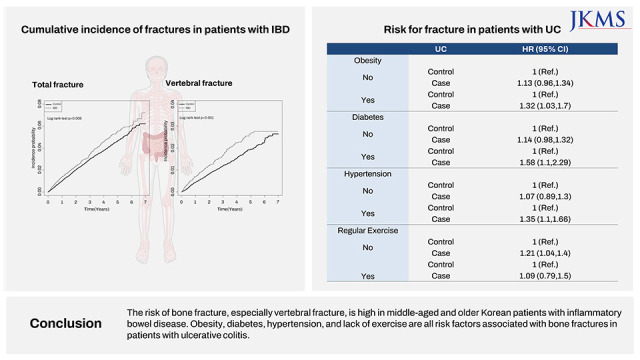
According to the type of fractures, the risk of vertebral fractures was significantly higher in patients with IBD, CD, and UC (aHR, 1.59, 95% CI, 1.33–1.92; aHR, 2.6, 95% CI, 1.74–3.88 and aHR, 1.42, 95% CI, 1.15–1.75 in Model 4, respectively). The risk of other fractures among CD patients, but not UC patients, was higher than that in the control group (aHR, 1.53, 95% CI, 1.03–2.28). IBD, CD, and UC were not associated with an increased risk of hip fracture (Table 2). The cumulative incidence of hip and other fractures in the IBD group was not significantly different from that in the control group (P = 0.656 and 0.444, respectively) (Fig. 2B and C). However, the cumulative incidence of vertebral fractures in IBD was significantly higher than in the non-IBD group (P = 0.001) (Fig. 2D).
Subgroup analysis
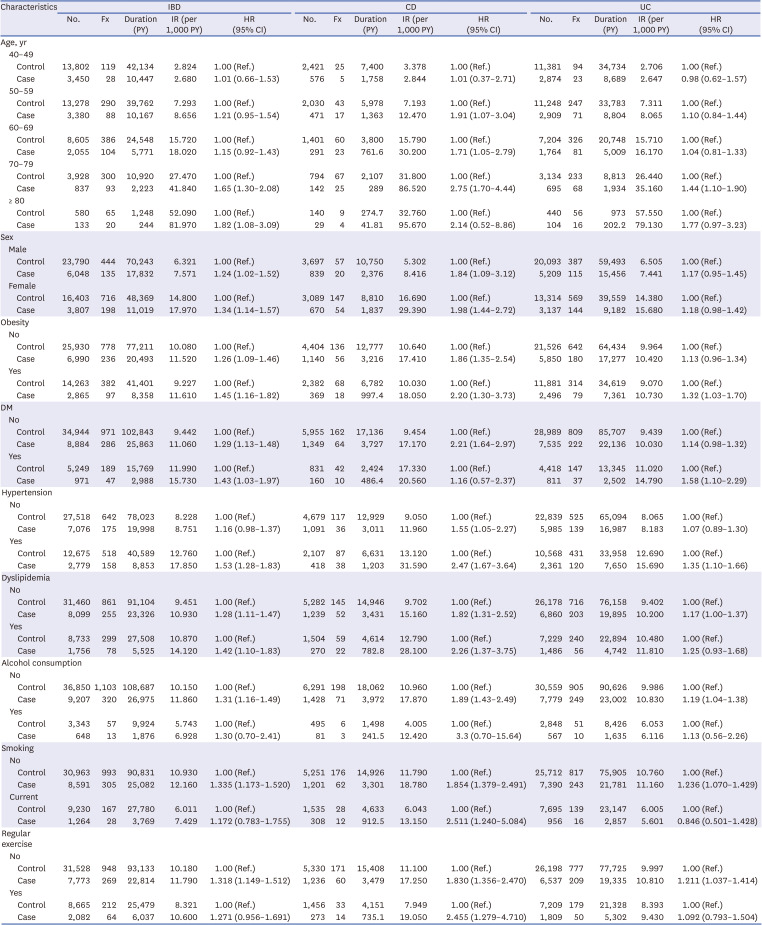
We examined the differences in the risk of fracture among patients with IBD, CD, and UC after adjusting for age, sex, place of residence, income level, history of prior fracture within five years, comorbidities like DM, hypertension, dyslipidemia, lifestyle habits such as smoking, alcohol consumption, and regular exercise (Table 3). The impact of IBD on the occurrence of fractures was significant in patients aged between 70 and 80 years (HR, 1.65) and above 80 years (HR, 1.82) and with comorbidities such as obesity (HR, 1.45), diabetes (HR, 1.43), hypertension (HR, 1.53), and dyslipidemia (HR, 1.42). Besides, the impact of UC on the development of fractures was more prominent in patients aged 70–80 years (HR, 1.44), with comorbidities such as obesity (HR, 1.32), diabetes (HR, 1.58), hypertension (HR, 1.35), and no regular exercise (HR, 1.21). In contrast, fracture risk tended to increase regardless of age, sex, comorbidities, and lifestyle habits in patients with CD.
Table 3
Subgroup analysis of risk for fracture in patients with inflammatory bowel disease
DISCUSSION
We found that the total and vertebral fracture risks in middle-aged and older Korean patients with IBD were significantly higher than in non-IBD individuals. To the best of our knowledge, this is the first nationwide cohort study to reveal the effects of comorbidities, lifestyle habits, and fracture risks in middle-aged and older populations with IBD. Interestingly, the fracture risk in CD increased regardless of age, sex, comorbidities, and lifestyle habits. At the same time, obesity, diabetes, hypertension, and no regular exercise were associated with increased fracture risk in UC.
Recently, several related studies have been published. A Swedish nationwide study revealed that hip and any fracture risks in an adult IBD group were higher than those in a non-IBD group (HR, 1.4 and 1.18, respectively) and were significantly associated with corticosteroid use.6 Similarly, a Korean nationwide study reported that vertebral and hip fracture risks in an IBD group were higher than in a non-IBD group (HR, 1.24), regardless of corticosteroid use.14 The results of both studies were similar to those of our study in terms of increasing fracture risks in IBD. Still, the studies included all IBD patients regardless of age, did not consider lifestyle habit and focused on corticosteroid use as a risk factor. Unlike previous studies, we included only middle-aged and older patients who could undergo osteoporotic changes and consider lifestyle behavior and comorbidities.
Our studies showed that vertebral fracture risk significantly increased in patients with IBD, UC, and CD. Long-term steroid use and bone composition may be associated with this. The ratio of cortical to the trabecular bone in the vertebrae is 25:75. In the femoral head, this proportion was 50:50.24 Riggs et al.25 reported that trabecular volumetric bone mineral density begins to decrease before middle age and proceeds linearly in both sexes, most prominently at the spine. In contrast, cortical volumetric bone mineral density decreases slightly with aging at the femoral neck. Corticosteroid use is a well-known risk factor for osteoporosis and bone fracture. Patients with IBD are often treated long-term with steroids. Glucocorticoid exposure was reported to be associated with a 60% increased risk of hip fracture and a 160% increased risk of vertebral fracture.26
Our study showed an increased risk of vertebral fractures rather than hip fractures, which differs from other studies, and this may be due to differences in the study population. Our study targeted patients aged 40 and above, while previous studies included all patients regardless of age. The risk of vertebral fractures in individuals over the age of 40 is generally related to osteoporosis, which is a condition that causes a decrease in bone density. A decrease in bone density can weaken the bones and increase the likelihood of vertebral fractures.27 On the other hand, the risk of hip fractures is not strongly related to osteoporosis. Instead, the risk of hip fractures is primarily associated with changes in the soft tissues that occur with age. Soft tissues play a role in supporting and stabilizing the joint, so changes in soft tissues can weaken the stability of the hip joint and increase the risk of hip fractures.2728
Vertebral fractures can cause back pain, worsening spinal deformity, limited mobility, and diminished pulmonary function, severely limiting independence and occasionally requiring hospitalization.293031 Therefore, we must interpret our results regarding the increased risk of vertebral fractures in IBD with caution.
Interestingly, bone fractures in patients with UC are associated with obesity, diabetes, hypertension, and lack of exercise; but further research is needed to uncover the related mechanisms. Previous studies have revealed that obesity, diabetes, hypertension, and exercise are associated with osteoporosis and fractures. The impact of several adipokines and cytokines released by adipose tissue, including leptin, resistin, adiponectin, interleukin 6, and tumor necrosis factor-alpha, on bone could be the cause of osteoporosis in obesity.3233 Systemic inflammation, advanced glycation end-product accumulation, and reactive oxygen species generation are all significantly altered in type 2 diabetes. These systemic alterations may have a negative impact on the bone remodeling cycle.34 Important links exist between changes in calcium metabolism and hypertension, including increased calcium loss, compensatory parathyroid gland activation, and increased calcium transit from bones. Deterioration of calcium homeostasis in long-term hypertension may lead to age-related osteoporosis and fracture.35 The risk of osteoporotic fracture being decreased by exercise is becoming more widely accepted since it can increase muscle strength and postural stability.36 There is still no clear evidence in patients with UC that there might be synergistic mechanisms for these factors to cause bone fracture. However, these findings are relevant because our study used large-scale population data. Therefore, in middle-aged and older patients with UC, we could cautiously assume that managing obesity, diabetes, hypertension, and exercise might help prevent fractures.
The major strengths of our study are as follows: 1) this is the first study to analyze the effects of comorbidities, lifestyle habits, and risk of fracture in the middle-aged and older population with IBD using a nationwide, population-based cohort; 2) we could use the data and information from in-depth surveys and laboratory results in the national checkup program; therefore, we performed the analysis using a large number of variables. However, our study also had some limitations, as follows: 1) our study did not consider drug use such as corticosteroid, immunomodulators and biologics. In our study, we found a higher risk of fractures in CD compared to UC. This may be potentially associated with the usage of steroids. It is well-known traditionally that steroid usage is more frequent in CD than in UC.37 However, due to limitations in our data, we were unable to analyze the impact of steroid usage; 2) because we used claims data, the definition of fracture could have caused bias; 3) we could not determine the cause of bone fracture; 4) the follow-up period in our study was relatively short; 5) there is a possibility that hip fractures may have been underestimated in this study. Because, vertebral fractures are often asymptomatic and may not be clinically diagnosed without imaging, while hip fractures usually present with more symptoms and are more likely to be clinically diagnosed; and 6) there are significant differences in age and gender between patients with IBD and the control group, despite age and gender matching. During the selection process of the final study participants, it was observed that the age and gender ratios were not maintained despite efforts to match for age and gender. Therefore, in our study, we included age and gender as covariates in the analysis to account for these potential confounding factors.
In conclusion, the risk of bone fracture, especially vertebral fracture, is increasing in middle-aged and older Korean patients with IBD. Obesity, diabetes, hypertension, and lack of exercise have increased the risk of bone fracture in UC but not in CD. These findings may be helpful for clinicians to educate patients with IBD on bone health and raise awareness of bone fractures in patients with UC who have specific risk factors.
 XML Download
XML Download