

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although the incidence of thyroid cancer has increased worldwide, the mortality has not changed markedly, due to the disease’s indolent features.1234 Even though thyroid cancer patients have a good prognosis, they have to be monitored for a longer time, and the medical expenditure related to cancer surveillance could be similar to—or even more than—other chronic medical conditions, such as diabetes or hypertension.5 A previous study showed that thyroid cancer patients generally have larger financial burdens and higher rates of bankruptcy than other cancer survivors.5 The out-of-pocket costs of initial thyroid cancer diagnosis and treatment range from USD 1,425 to USD 17,000; that is comparable to the costs of cancers with higher mortality, such as cervical, gastric, and esophageal cancer.5
Papillary thyroid cancer smaller than 1 cm is called papillary thyroid microcarcinoma (PTMC). It has been incidentally detected more frequently with other imaging tools; generally, it is not aggressive and progresses slowly.678 In this regard, active surveillance (AS) has been proposed as an alternative management plan to early surgery (ES). However, only a few studies have investigated the cost and effectiveness of AS versus ES, considering disease status and treatment strategy.9 One study, with a study population limited to older adults aged > 65 years, showed that disease stage was an important driver of treatment costs; additional cost of USD 8,902 for regional disease and USD 20,103 for distant metastases were added for five years after diagnosis.10 However, AS was not regarded as a treatment option in the study, with only ES considered for the management of PTMC. In one recent study from Korea, despite the initial costs of AS being lower than ES, in the long-term follow-up, ES was more economical than AS.11 However, this study did not consider the effectiveness or utility score of each treatment strategy. In addition, the study employed a prospective cohort study approach; therefore, it does not fully reflect real-world practice.
Cost-effectiveness analyses could be affected by the country’s healthcare economics system. As most previous studies were conducted in other countries, rather than the Republic of Korea, it is difficult to apply these results directly to present clinical practices in Korea. Therefore, based on the current status mentioned above, we built the cost-effectiveness analysis model based on a real-world practice scenario with the Korean medical cost system and from a Korean cohort considering utility score.
METHODS
Base case scenario and cost-effectiveness analysis model construction
The reference case scenario is that of a healthy 40-year-old patient with a biopsy-proven, unifocal PTMC. This study created a Markov state-transition decision analysis model to analyze the cost-effectiveness of AS of PTMC (Supplementary Fig. 1).1213 Six health states were assumed: continued AS, post-hemithyroidectomy (HT) surveillance without complication, post-HT surveillance with complication, post-total thyroidectomy surveillance without complication, post-total thyroidectomy surveillance with complication, and death. We only considered long-term complications, such as hypocalcemia induced by post-procedural hypoparathyroidism or hypothyroidism by mostly thyroidectomy, assuming that short term complications would barely affect the result of a cost-effectiveness analysis in the long-term follow-up model.
The model cycled annually. Because we assumed the 40-year-old patient as the base case, considering the peak-incidence age of thyroid cancer in Korea,314 the termination of follow-up year ranged from 1 year to 50 years. Age-based probability for mortality was calculated, based on both disease-specific mortality in a Korean cohort population15 and age-dependent all-cause mortality obtained from the “life table” produced by the Korean National Statistical Office.16
Cost and quality-adjusted life years (QALYs) were tracked and were discounted at a rate of 3% or 4.5%, according to a previous study and the current Health Insurance Review and Assessment Service (HIRA) guidelines.1117 Willingness-to-pay (WTP) was set at USD 100,000 or 30,000, based on a previous study and current HIRA guidelines.1718 TreeAge Pro software (TreeAge, Williamstown, MA, USA) was used to construct and analyze the model.
Input data
The input data used in the model are summarized in Table 1.192021222324 The direct medical costs were only considered for cost estimation. The direct costs include physician visiting fee, blood test fee, procedure costs for ultrasonography, biopsy, surgery or radioactive iodine (RAI) therapy, and costs of drugs, including levothyroxine or calcium/vitamin D. We did not consider the indirect costs, such as transportation costs or productivity loss. The costs were based on the 2020 HIRA publication.19
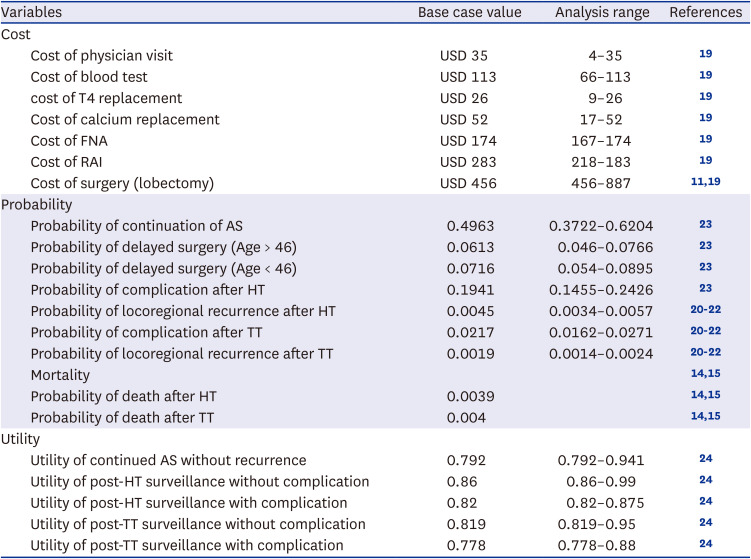
Table 1
Model input data
| Variables | Base case value | Analysis range | References | |
|---|---|---|---|---|
| Cost | ||||
| Cost of physician visit | USD 35 | 4–35 | 19 | |
| Cost of blood test | USD 113 | 66–113 | 19 | |
| cost of T4 replacement | USD 26 | 9–26 | 19 | |
| Cost of calcium replacement | USD 52 | 17–52 | 19 | |
| Cost of FNA | USD 174 | 167–174 | 19 | |
| Cost of RAI | USD 283 | 218–183 | 19 | |
| Cost of surgery (lobectomy) | USD 456 | 456–887 | 1119 | |
| Probability | ||||
| Probability of continuation of AS | 0.4963 | 0.3722–0.6204 | 23 | |
| Probability of delayed surgery (Age > 46) | 0.0613 | 0.046–0.0766 | 23 | |
| Probability of delayed surgery (Age < 46) | 0.0716 | 0.054–0.0895 | 23 | |
| Probability of complication after HT | 0.1941 | 0.1455–0.2426 | 23 | |
| Probability of locoregional recurrence after HT | 0.0045 | 0.0034–0.0057 | 202122 | |
| Probability of complication after TT | 0.0217 | 0.0162–0.0271 | 202122 | |
| Probability of locoregional recurrence after TT | 0.0019 | 0.0014–0.0024 | 202122 | |
| Mortality | 1415 | |||
| Probability of death after HT | 0.0039 | 1415 | ||
| Probability of death after TT | 0.004 | 1415 | ||
| Utility | ||||
| Utility of continued AS without recurrence | 0.792 | 0.792–0.941 | 24 | |
| Utility of post-HT surveillance without complication | 0.86 | 0.86–0.99 | 24 | |
| Utility of post-HT surveillance with complication | 0.82 | 0.82–0.875 | 24 | |
| Utility of post-TT surveillance without complication | 0.819 | 0.819–0.95 | 24 | |
| Utility of post-TT surveillance with complication | 0.778 | 0.778–0.88 | 24 | |
FNA = fine needle aspiration, RAI = radioactive iodine, AS = active surveillance, HT = hemithyroidectomy, TT = total thyroidectomy.
![]()
The schedule of ultrasonography follow-ups was based on a scenario from a previous study.11 All costs were estimated in Korean Republic Won (KRW) and converted into USD by applying the exchange rate of 1 USD to 1,300 KRW (August 01, 2022), before being inserted into the model. To reflect real life scenarios, the costs used ranged widely, according to the kinds of hospitals—such as primary hospital or tertiary hospital—provided in the HIRA data. Base costs were estimated according to the costs of a tertiary hospital.
Transition probabilities were calculated based on previous literature, especially studies with Korean populations.20212223 These transition probabilities were calculated, as suggested in the previous literature.25 For the sensitivity analysis, the values ranged from 75% to 125%.
The possibility of delayed surgery was different in previous literature: patients with younger than 46 years of age were more likely to be treated with delayed surgery. We reflected this probability change according to the age to the analysis.
The utility score is a measure of the overall quality of life and patient preferences related to a specific health condition or treatment. The utility scores range from 0 to 1, with 1 indicating perfect health and 0 indicating death. The utility score could be calculated in many ways.9 EuroQol-5 Dimension (EQ-5D) is one example of the representative methods used to access utility scores. EQ-5D is a standardized instrument that measures health-related quality of life based on five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.26 Due to the lack of research on the utility score of PTMC in a Korean population, we have used the utility score from studies involving various ethnics.24 Because there was no absolute utility score fit to our health status assumption, the minimum and maximum scores for each health status were used for sensitivity analysis.
RESULTS
Base-case analysis
For the base scenario with discount rates of 3% and 4.5%, the cumulative costs and effectiveness were both higher in ES than in AS. In each case, incremental cost-effectiveness ratio (ICER) was USD 5,380.86 and USD 5,930.14, both lower than the set WTP. The net monetary benefit (NMB) was higher for ES than for AS in both cases (USD 1,931,859 vs. USD 2,091,526 in the base case with 3% rate, and USD 1,521,828 vs. USD 1,646,345 in case with 4.5% discount rate; Table 2).

Table 2
ICER in base case (discount rate 3%) and scenario, with discount rate 4.5%
ICER = incremental cost effectiveness ratio, QALY = quality-adjusted life year, NMB = net monetary benefit, AS = active surveillance, ES = early surgery.
![]()
During all stages of the model analysis, cumulative cost for ES was always higher than that of AS; however, the ICER decreased according to the stage of the model analysis. In the first stage, the ICER was USD 12,057, while in the last stage, it was USD 4,237. Furthermore, the difference in NMB between AS and ES increased across the stages; at the first stage, the difference was USD 5,980 while in the last stage, it was USD 159,667 (Fig. 1).
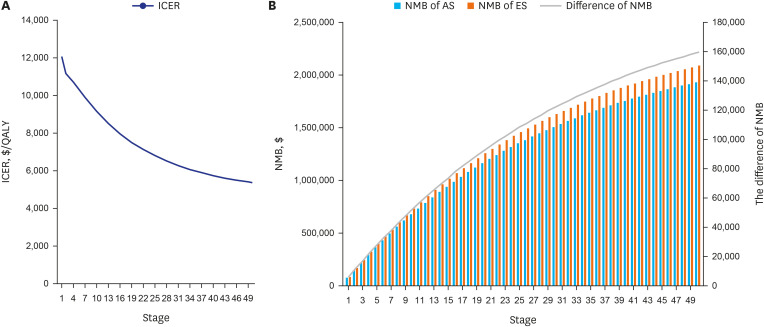
Fig. 1
The ICER and the NMB according to each stage. (A) The ICER decreased according to the stages. (B) The blue bar represents the NMB of AS and the orange bar represents the NMB of ES. The difference in NMB is increasing with each stage, and is represented as a gray curve.
ICER = incremental cost effectiveness ratio, NMB = net monetary benefit, QALY = quality-adjusted life year, AS = active surveillance, ES = early surgery.
![]()
Sensitivity analysis
The tornado diagram illustrates that the start age, utility score of AS or post-HT surveillance, mortality after HT, and cost of surgery had the strongest effects on the analysis (Table 3).
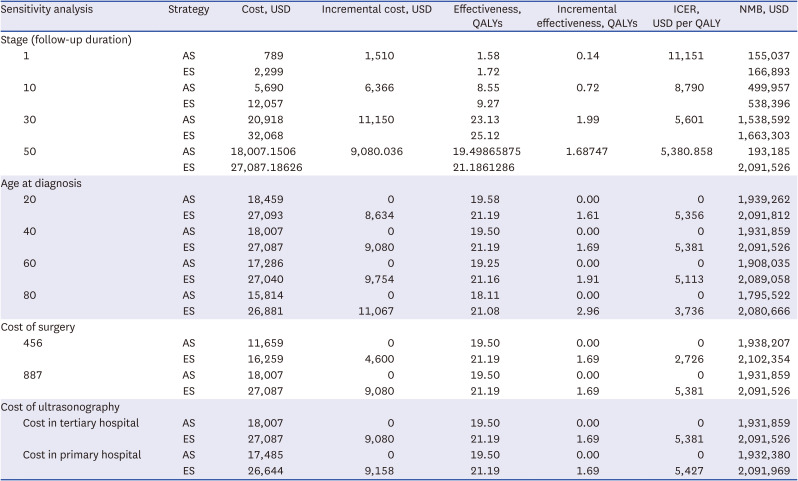
Table 3
Results of sensitivity analysis
![]()
When the analysis starting age was changed from 10 to 100 years old, the ICER decreased as the age increased (USD 5,356/QALY at 15 years old and USD 2,736/QALY at 100 years old). At any age, the ICER was always under the set WTP (Fig. 2A).
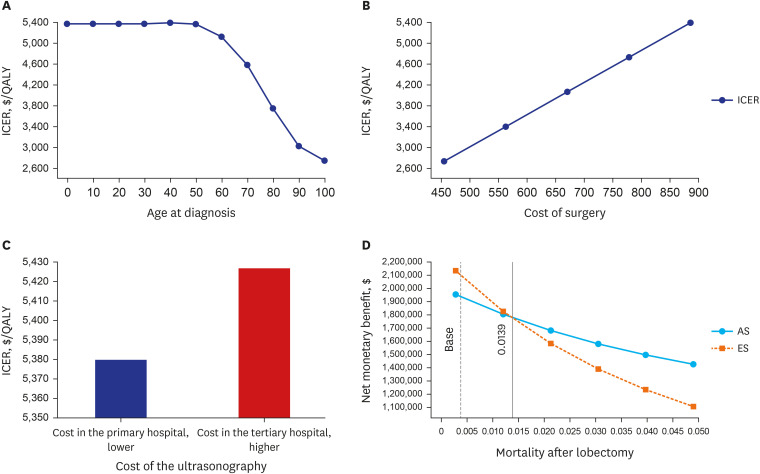
Fig. 2
The results of the one-way sensitivity analysis. (A) The ICER according to age at diagnosis; the ICER decreases with age. (B) The ICER according to surgery costs; the higher surgery costs, the higher the ICER. (C) The ICER according to cost of ultrasonography; the higher the ultrasonography cost, the higher the ICER. (D) The NMB according to mortality after lobectomy. At base case (0.0039), the NMB of ES is higher than NMB of AS. At 0.0139, however, the two lines cross. If the mortality is higher than 0.0139, the NMB of AS is higher than the NMB of ES.
ICER = incremental cost effectiveness ratio, NMB = net monetary benefit, ES = early surgery, AS = active surveillance, QALY = quality adjusted life year.
![]()
As the cost of surgery increased, the ICER increased. However, the ICER remained lower than the set WTP for all surgeries (with cost of surgery USD 456, ICER was USD 2,725/QALY and with cost of surgery USD 887, ICER was USD 5,380/QALY; Fig. 2B).
We also compared the costs of an ultrasound in a primary and a tertiary hospital. Despite the cost being higher in a tertiary hospital, the ICERs were below the WTP for both (USD 5,381/QALY for primary hospitals and USD 5,427/QALY for tertiary hospitals; Fig. 2C). At the base scenario, with a 0.0039 transition possibility of death after lobectomy, the NMB of ES is higher than that of AS. At the possibility of 0.0139 (about 3.5 times possibility in the base scenario), the NMB was reversed (Fig. 2D).
With the cost-effectiveness acceptability curve, the iterations were reversed when WTP was approximately USD 5,000 (Fig. 3A). At the base scenario, with WTP set at USD 100,000, ES was always cost-effective. Therefore, we performed a two-way sensitivity analysis, reducing the WTP.
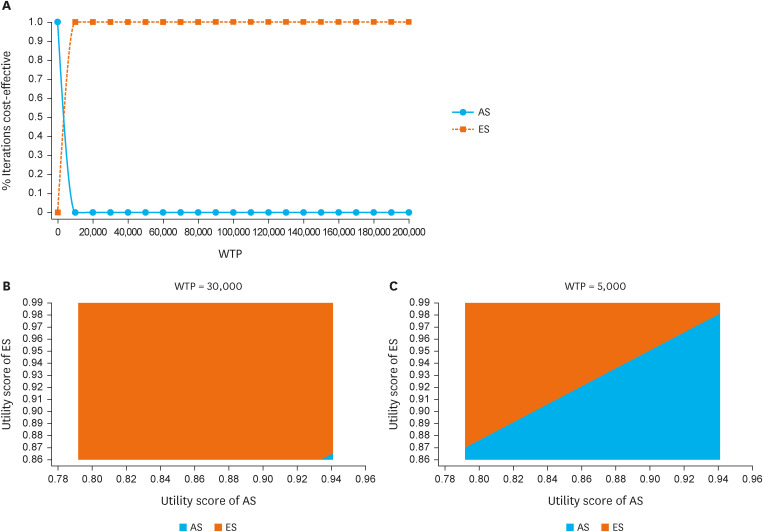
Fig. 3
The cost-effectiveness acceptability curve and the results of the two-way sensitivity analysis. (A) With the cost-effectiveness acceptability curve, the iterations were reversed when WTP is about USD 5,000. (B) The higher the utility score of ES (≥ about 0.865) and the lower the utility of AS (< about 0.934), the higher the cost-effectiveness of ES, with WTP set at USD 30,000. (C) With lower WTP (USD 5,000), AS was slightly more cost-effective, but the ES was still the most cost-effective.
WTP = willingness-to-pay, ES = early surgery, AS = active surveillance.
![]()
The two-way sensitivity analysis showed that the higher the utility score of ES (≥ 0.865) and the lower the utility of AS (< 0.934), the higher the cost-effectiveness of ES, with WTP set at USD 30,000 (Fig. 3B). Therefore, ES was mostly cost-effective. With a lower WTP (USD 5,000), AS was slightly more cost-effective; however, overall, ES was still the most cost-effective (Fig. 3C).
Although the utility score of the AS is lower than that of ES with complication in base scenario (0.792 vs. 0.82), we did two-way sensitivity analysis continuously changing the utility score of AS (from 0.792 to 0.941) as well as that of ES (from 0.82 to 0.875). Therefore, it includes cases where the utility score of AS is greater than the utility score of ES. In most cases the ES was cost effective.
DISCUSSION
The results of this study showed that ES was the most cost-effective in the Korean medical environment. As the number of stages in our model increased, the monetary value obtained through ES was higher than that obtained through AS. The analysis starting age, utility scores, and cost of surgery were the variables that most affected the results. As the analysis starting age increased, the ICER decreased and as the cost of surgery increased, the ICER increased; moreover, the higher the utility score of ES and the lower the utility of AS, the higher the cost-effectiveness of ES.
In an existing study from Hong-Kong, the ICER of AS, compared with ES, was USD 473, meaning that AS was more cost-effective.27 In a study from the United States, the ICER of ES, compared with AS, was USD 4,437, indicating that ES is more cost-effective.28 Another study from the United States concluded that a strategy with the guideline including AS is more cost-effective.29 In our study, ES was shown to be most cost-effective; this difference in results seems to be due to differences in each country’s economic system.
In particular, there is a difference in terms of cost.9 In the United States, surgery costs range from USD 8,000 to USD 12,000, an ultrasound costs about USD 100, and a fine needle aspiration costs about USD 500.2829 However, in Korea and Japan, the costs are relatively low. In previous Japanese studies, surgery costs were between USD 2,800 and USD 3,200, with an ultrasound costing USD 32 and a fine needle aspiration costing USD 55.30 In this study, the cost of surgery was set at USD 887, the cost of a fine needle aspiration was USD 174, and the cost of ultrasound was set at about USD 70; these values are similar to those in another study from Korea.11 Because of the relatively inexpensive ultrasound cost, the total cost for AS was approximately a quarter of the cost of surgery, according to a study conducted in Japan.30 In our study, the cost of an ultrasound is cheap, while the cost of surgery is relatively cheaper; therefore, ES is considered to be cost-effective.
While reflecting on these costs, patients’ follow-up period should also be considered. In an Australian study, the cost of ES was initially shown to be higher than that of AS; however, after 16 years of follow-up, the costs of AS and ES reversed.31 In another study that analyzed only cost, based on a recent prospective study in Korea, the follow-up period was changed to about 15 years.11 In our study, however, the cost of ES is consistently higher than that of AS. This may be related to the low mortality rate of thyroid cancer. Indeed, drastically altering mortality after surgery reverses the values obtained by both interventions. The younger the diagnosis, the higher the efficacy obtained with ES; however, this also translates to a higher cost of lifelong use.
Venkatesh et al.’s study28 shows similar results to ours. The lower the diagnosis age, the higher the overall cost, but the higher the efficacy. This may also be related to the low mortality of thyroid cancer; patients spend a long time living with the diagnosis as a chronic disease.9 However, if thyroid cancer follow-up is simply stopped without taking the mortality into account, it results in a longer follow-up and higher value obtained from ES, compared to the value obtained from AS. In other words, if the disease is diagnosed at a young age and the follow-up is planned for a long time, ES can be more cost-effective. Recently, one study had a similar conclusion with the United States’ medical economic system; ES was cost-effective when the diagnosis age was 40 while the AS was cost-effective when the diagnosis age was 69.32
Indirect costs were not included in our study, as indirect costs are difficult to measure, and therefore, they may introduce uncertainties.33 Instead, they were replaced by changing several costs—including ultrasound cost and surgery cost—in the sensitivity analysis. As the cost of surgery increased, the cost of obtaining one QALY increased, although all costs remained below the WTP, meaning that they were still cost-effective. Ultrasound costs in tertiary hospitals were higher than that in primary hospitals, but ICER remained below the WTP.
Our results also showed that the higher the ES utility score and the lower the AS utility score, the higher the cost-effectiveness of ES. These results were obtained when the WTP was set at USD 30,000 or USD 5,000, which is much lower than the WTP suggested by other studies (USD 100,000 or USD 50,000).1834 When the WTP is set at USD 100,000, ES is always cost-effective. Although the healthcare economic systems differ, a study from the United States also concluded that the cost-effectiveness of ES is dependent on utility changes.28
Our study has limitations in applying the utility score to our cost-effectiveness analysis model. Although the utility score used in this study was obtained from a systematic review on the utility scores of patients with papillary thyroid carcinoma, it might be difficult to completely apply to PTMC among Korean patients, because the race and research settings of each study are different. Also, as mentioned in the methods section, the utility score we used does not exactly fit our health status assumption. In particular, most of the previous studies focused on surgical results, which could overestimate cancer diagnosis and underestimate post-treatment complications. So, the condition before surgery tends to appear relatively negative; the utility scores for AS were based on the assumption that patients were living with the knowledge that they had a cancer diagnosis and were under surveillance, which may have contributed to the lower scores due to burdens of emotional anxiety.2835 On the other hand, the utility scores for post-HT with complications may have been influenced by the fact that these patients had undergone a definite treatment and may have been relieved of the burden of cancer surveillance.2636
To verify the reliability of lower utility score in AS than ES in our study, the sensitivity analysis was performed. In particular, in the 2-way sensitivity analysis, we analyzed the our cost-effectiveness model while continuously changing the utility scores of AS and ES including cases where the utility score of AS is greater than the utility score of ES. At this time, the utility score of AS and ES per se was important but in the end the WTP had a greater impact on the progress. Despite of it, the result that ES is more cost-effective than ES, did not change. Researches on this issue is currently ongoing in a large cohort and the results can be expected in the near future.
The current study is significant in that it was the first to build a model for the cost-effectiveness analysis of PTMC and analyze it in the context of the Korean medical system. Currently, there is one well-designed prospective study (Korean Multicenter Prospective Cohort Study of Active Surveillance or Surgery) that targets ES versus AS in PTMC; this study is still underway in Korea and it can help check medical results and re-evaluate cost-effectiveness analysis.37
In summary, in the current Korean medical system, ES is more cost-effective than AS, especially if the diagnosis is performed at a young age and followed-up for a long time.
 XML Download
XML Download