

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute myocardial infarction (AMI) remains a major cause of morbidity and mortality in the Asia-Pacific region,1) with mortality often exceeding that of developed western countries.2) The Asia-Pacific region is heterogenous, with a large diversity of ethnicities, cultures, income levels, systems of care and healthcare spending in its constituent countries.
Accordingly, mortality rates from AMI differ, with the gap arguably starkest between high-income and middle/low-income countries. Whilst mortality rates from ischemic heart disease and cardiovascular disease in general have declined over the past 3 decades in the subset of high-income Asia-Pacific countries,3)4) this trend is reversed when considering the entirety of Asia as a whole (Figure 1). Comparing mortality rates of individual countries across the same period also reveals considerable differences.
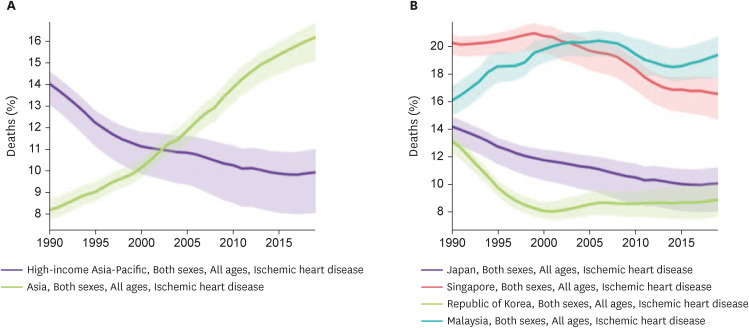 | Figure 1(A) Mortality rate of ischaemic heart disease in Asia versus only high-income Asia-Pacific countries, 1990–2019. (B) Morality rate of ischaemic heart disease in Japan, Singapore, Republic of Korea and Malaysia, 1990–2019. Lighter areas represent 95% confidence intervals for estimates. Data based on the Global Burden of Disease Study 2019.3)
|
These differences are driven by a multiplicity of factors, some of which may not be readily amenable to intervention (e.g., ethnic composition). Nevertheless, systems of care have been shown to play a significant role in determining AMI outcomes, particularly in the context of ST elevation myocardial infarction (STEMI),5)6) and represent an important target for intervention and improvement.
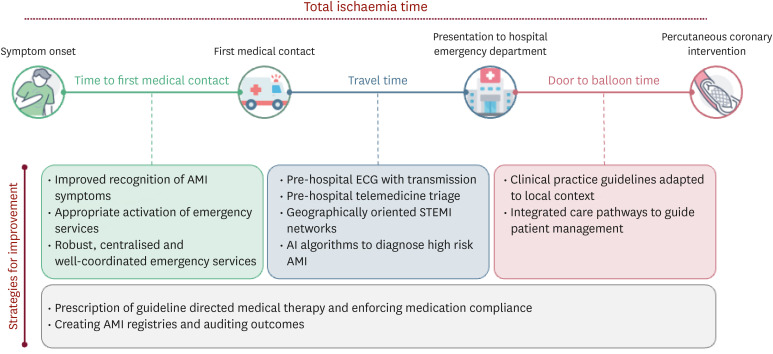
Whilst by no means comprehensive, this narrative review represents the authors’ take on gaps in pre- and in-hospital AMI care in Asia-Pacific (Figure 2). The aim is to highlight present system deficiencies and suggest possible improvements to enhance quality of care. We have chosen to focus on Korea, Japan, Singapore and Malaysia as representative countries given their availability of data.
Go to : 
PRE-HOSPITAL CARE
Prompt and accurate diagnosis and intervention is important in AMI; nowhere more so than in cases of STEMI where “time is myocardium.”7) Every minute of delay in treatment of STEMI results in worse mortality outcomes.8)9) This introduces the concept of total ischemic time (TIT), which comprises both patient delays and systemic delay. Patient delays occur when time is lost between symptom onset and first medical contact (FMC), whilst systemic delays represent the subsequent time taken by healthcare systems to make a diagnosis of STEMI, triage patients to appropriate centers and achieve reperfusion. Both patient delays and systemic delays can and should be optimized to reduce TIT, and this is reflected in the latest European Society of Cardiology (ESC) guidelines on STEMI management.10) Pre-hospital care can be enhanced by reducing time to FMC, improving emergency medical services (EMS), employing pre-hospital 12-lead electrocardiograms (ECGs) and building STEMI networks that allow patients to be right-sited to percutaneous coronary intervention (PCI) capable hospitals.
Time to first medical contact
Time to FMC is primarily affected by the ability of patients to recognize AMI symptoms and seek medical attention. Often, activating EMS represents the most expedient way of obtaining medical assistance, and the public should be educated on calling for an ambulance if they identify AMI symptoms. Nevertheless, public awareness of AMI symptoms and the need to activate EMS remains suboptimal, as captured by nationwide surveys.
In a nationwide survey of 9,600 residents in Korea, 88.7% knew ≥1 symptom but only 10.9% knew all 5 symptoms of AMI. The 67% would call an ambulance if someone showed signs of AMI.11) A similar survey using the Korean Community Health Survey involving 228,281 participants found that only 42.4% were aware of MI symptoms.12) A Malaysian survey of 393 respondents found that 11.5% recognized all 5 AMI symptoms, 82% recognized ≥1 symptom and 35.6% would call an ambulance for AMI symptoms.13) Meanwhile, a survey of 4,192 respondents in Singapore found that 57.8% were proficient in identifying AMI symptoms.14) In Japan, only 11.6% of the 1,200 participants surveyed were aware of the need to call EMS promptly for AMI symptoms.15) More broadly, a meta-analysis by Sharma et al.16) reported a wide variation in the prevalence of awareness of chest pain as a symptom of MI in various Asian countries.
Amongst the abovementioned studies, a common risk factor for not identifying AMI symptoms was a low education level.12)15)17) This may potentially be remediated by a national campaign on AMI symptoms and the need to activate EMS rapidly, especially given how effective the analogous “Act FAST” campaign has been in improving public awareness of stroke symptoms.18)
Making use of emergency medical services
EMS use is associated with substantial reduction in treatment delays and TIT in STEMI,19) and the ESC guidelines on STEMI recommend having an EMS with an easily recalled and well-publicized number.10) Similar findings on the benefits of utilizing EMS have been reported in Asian studies, including significantly improved odds of symptom to door time <60 minutes in Korea20) as well as shorter symptom-to-door time, door-to-ECG time, ECG-to-diagnosis time, door-to-balloon (DTB) time, and symptom-to-balloon time in Singapore.21)22)23)
Given this, a robust and well-coordinated EMS system is imperative. Currently, both Korea and Japan have one-tiered ambulance-based EMS activated by the number “119.” Singapore’s EMS is administered by the Singapore Civil Defence Force via the number “995.” In Malaysia, whilst the Ministry of Health remains the main provider of ambulance services, other agencies such as the St. John’s Ambulance of Malaysia, Malaysian Red Crescent Society, Civil Defence, University Hospitals and private ambulance services also contribute. Consequently, in 2007 the Malaysian government established the Malaysia Emergency Response Service 999 system as well as the Medical Emergency Call Centre to coordinate ambulance services and EMS.24) There remains considerable heterogeneity in EMS system set-up and maturity amongst Asia-Pacific countries.25)26) Countries should consider amalgamating medical first-responder services under a centrally operated public EMS for ease of access.
Use of pre-hospital 12-lead electrocardiogram
One of the advantages of EMS activation over private transport to a healthcare facility is the opportunity to obtain an early 12-lead ECG. Guidelines suggest that EMS providers should be accountable for performing a pre-hospital ECG, making the diagnosis of STEMI and deciding whether or not to transport patients to a PCI-capable hospital.10)27)
A nationwide rollout of 12-lead ECG recording and transmission by ambulance crews was undertaken in Singapore in 2008 and was associated with a significant improvement in DTB times in STEMI patients.28) The National Heart Association of Malaysia Clinical Practice Guidelines for management of STEMI and non-ST elevation myocardial infarction (NSTEMI) also recommends performing and transmitting a 12-lead ECG that should be read in <10 minutes.29)
Pre-hospital ECG has been shown to be beneficial in Japanese and Korean studies, but adoption remains limited and pre-hospital ECGs are not always performed by EMS staff.30) In Busan, Korea, local implementation of a 12-lead ECG transmission system led to reductions in systemic time delay and DTB time.31) Meanwhile, in Kanagawa, Japan, use of pre-hospital ECG was associated with reduced in-hospital mortality in addition to shorter DTB times.32) An alternative system employed “doctor car” systems where EMS providers initiated contact with patients before ambulance services arrived and performed a 12-lead ECG that was uploaded to the cloud, leading to improved DTB time.33) The authors suggest that pre-hospital 12-lead ECGs should be conducted and transmitted routinely, leveraging the growing ubiquity of 4G and 5G networks.
Looking to the future, ambulance-to-hospital transmissions could be augmented even further by the use of telemedicine video consults whilst patients are still enroute, thereby allowing physicians in emergency departments to begin the process of assessment and triage early, especially when there is significant ambulance travel time. Such video consultation services have already been trialed in the context of stroke activations34) and trauma.35) One potential use case could be in the early assessment of patients with out of hospital cardiac arrest such that a decision can be made as to whether cardiac catheterisation laboratories activation is appropriate and required.
ST elevation myocardial infarction networks and appropriate triage
Early reperfusion, ideally via primary PCI, is the mainstay of STEMI management.27) This requires transfer to a PCI-capable hospital should STEMI be diagnosed. Consequently, it makes sense to develop geographically oriented STEMI networks to facilitate timely transfer of patients.10)
Such STEMI networks have been reliably instituted in Korea and Singapore. In Japan and Malaysia, the development of the Tokyo Cardiovascular Care Unit (CCU) network36) and the MySTEMI network37) in the respective countries has proven to be effective, especially in service of the populous capitals of Tokyo and Kuala Lumpur. However, these networks are less well established in more remote parts of these countries. Hub and spoke models have also been trialed, albeit to a limited extent, in other Asia-Pacific countries such as India38) and China.39) Future directions for AMI care in Asia-Pacific should include a nationwide commitment to developing trustworthy STEMI networks. Lessons can be learnt from Korea, where the government passed the Cardio-cerebrovascular Disease Prevention and Control Act in May 2017 that laid the legal frameworks for the establishment of regional treatment networks in the form of regional cardio-cerebrovascular centers, which have now translated to positive improvements in clinical outcomes.40)
Appropriate transfer to PCI centers also necessitates accurate diagnosis of AMI (both STEMI and NSTEMI). In the future, artificial intelligence (AI)-based algorithms may aid EMS staff in identifying patients with AMI. AI algorithms based on symptoms, vital signs and symptoms have already achieved good performance41) and shown to be helpful in triaging chest pain.42) These algorithms have been applied to both STEMI43) and NSTEMI44) cases, with positive outcomes.
Go to :
IN-HOSPITAL CARE
Hospitals are complex systems, and many factors affect the in-hospital care of AMI patients as well as their outcomes. These range from availability of facilities such as cardiovascular laboratories, to appropriate and timely use of pharmacological and invasive therapies, and are often constrained by local resources and funding. The authors would like to focus the scope of discussion to the use of standardized protocols and care pathways, optimizing medical therapy, and maintaining registries for quality improvement.
Local guidelines, standardized protocols and care pathways
Clinical practice guidelines provide an opportunity for standardizing treatment and establish an objective specification on how patients ought to be managed. Nevertheless, they ought to be adapted to the local context. The National Heart Association of Malaysia has developed Clinical Practice Guidelines in 2019 and 2021 for the management of STEMI29) and NSTEMI,45) respectively; the Japanese Circulation Society previously published guidelines on the treatment and diagnosis of acute coronary syndrome in 201846) and the Korean Society of Myocardial Infarction has put together expert consensus recommendations on pharmacotherapy47) and revascularization48) for AMI that take into account evidence gathered from Korean populations. Countries that do not have local guidelines may consider referring to those created by countries with similar patient demographics, in addition to American or European guidelines.
On a more practical level, healthcare teams can be better guided in their management of patients by integrated care pathways, which aim to translate guidelines into clearly laid out stepwise clinical processes that fit into the unique culture and system of a particular healthcare institution. When applied to AMI, care pathways have already been shown to reduce DTB time and length of stay.49)50)51) A Korean study of 2 academic tertiary hospitals found that care pathways standardized patient care and negated time delays even when patients arrived out of hours or on weekends.52) The positive effects of care pathways on clinical outcomes have also been replicated in studies in Hong Kong53) and Pakistan.54)
Additionally, discharge protocols can be employed to ensure that patients have been medically optimized prior to discharge, including being started on the appropriate guideline-directed medications. They can also be used to identify patients who are at low risk and may qualify for early discharge and as such a shorter length of stay.55) These can be supplemented by written advice to patients regarding lifestyle changes, rules around driving, and gradual return to physical activity. The care pathways and protocols should extend beyond the index hospital admission and guide cardiac rehabilitation and follow-up. At present, there is overall poor uptake and compliance to these integrated care pathways, which represents an opportunity for improvement.56)
Pharmacotherapy for secondary prevention
Typical medications for the secondary prevention of AMI include dual antiplatelet therapy (DAPT), lipid lowering therapy, Beta-blockers and angiotensin converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARB). The Asia-Pacific Society of Cardiology and the Korean Society for Myocardial Infarction have summarized expert consensus on appropriate pharmacotherapy post AMI, integrating published European and American guidelines with contemporary studies involving Asian patients.47)57)
Rates of in-hospital prescription of these medications have previously been summarized in a meta-analysis,58) as well as in reported registry data.59)60)61)62)63)64)65) Whilst prescription of DAPT and statins were often in excess of 90%, prescription of beta-blockers and ACEi/ARBs was far more inconsistent. Furthermore, the use of guideline-directed medical therapy declined with time.66) Given that the use of guideline-directed medications has been shown to be inversely associated with mortality,60) the authors recommend that attention be given to improving prescribing rates of these medications where not contraindicated, as well as to ensuring that patients remain compliant to medical therapy at follow-up.
Acute myocardial infarction registries drive audit and quality improvement
Finally, the authors recommend the establishment of more AMI registries for the purposes of audit and quality improvement. Experience from the Get With The Guidelines programme in the United States (US) has shown that registries are effective in driving guideline-concordant care over time in participating hospitals.67)
A few voluntary AMI-based registries are present in Korea and Japan: for example, the Korea Acute Myocardial Infarction Registry,59) the Korean Registry of Acute Myocardial Infarction for Regional Cerebrovascular Centers,68) Japanese Registry of All Cardiac and Vascular Diseases Diagnosis Procedure Combination,60) Japan Acute Myocardial Infarction Registry69) and the registry from the Tokyo CCU network.70) However, the abovementioned registries only involve a limited number of hospitals. In contrast, the Singapore Myocardial Infarction Registry (SMIR)61) and the Malaysian National Cardiovascular Disease-Acute Coronary Syndrome Registry71) are national, and of the 2 only the SMIR is compulsory and mandated by law. Other examples from Asia-Pacific countries include the Thai Acute Coronary Syndrome Registry72) and the Clinical Pathways for Acute Coronary Syndromes in China Registry,73) but in general few countries in Asia-Pacific maintain registries, and quality of data varies greatly.74)
Formal collection of AMI data in the form of registries not only allow for audit and clinical improvement, but also provide insight into local AMI trends and can be used for research or to guide healthcare policy at the national level.58)75) Comprehensiveness of dataset is thus important, and there may be an argument for government mandated nationwide registries. In any case, the authors advocate for the creation of internal registries with data sharing, common data structures and feedback between healthcare institutions, especially within regional STEMI networks. The Mission: Lifeline Accelerator Projects in the US showed that internal registries coupled with training, regional reports and leadership meetings was associated with improvements in treatment times and mortality, which was not apparent in hospitals that were not participating in the project.76)
Go to :
CONCLUSION
Whilst there has been significant progress in the treatment of AMI in Asia-Pacific over the past 2 decades, and especially in high income countries, there remains room for improvement (Table 1). Countries can learn from each other and adopt systems of care that have worked well in contemporaneous circumstances. In this review, we have suggested leveraging on centralized EMS to reduce pre-hospital delays, employing clinical guidelines and care pathways to standardize and streamline care, improving prescription rates of guideline-directed medical therapy and employing registries as data repositories for audit and research as areas to focus future efforts on.
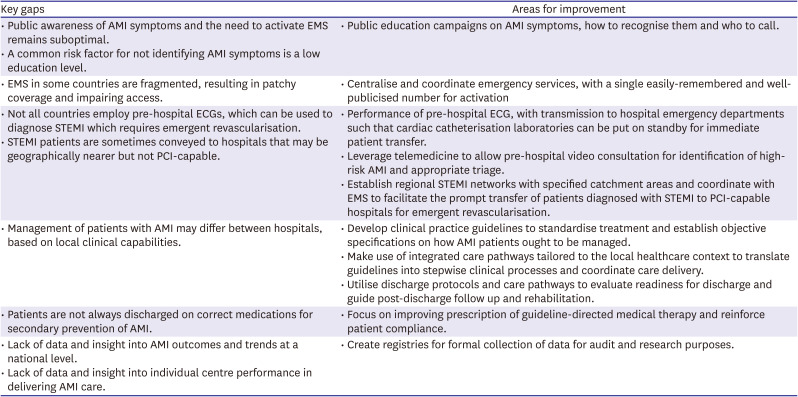
Table 1
Gaps in current AMI care and potential areas for improvement
AMI = acute myocardial infarction; ECG = electrocardiogram; EMS = emergency medical services; PCI = percutaneous coronary intervention; STEMI = ST elevation myocardial infarction.
![]()
Nonetheless, we recognize that AMI care is multidimensional, and there is much more that can be done that has not been captured in the discussion above. Furthermore, the scope of our discussion has centered mostly around a limited number of countries—and we appreciate that different challenges may be present in other Asia-Pacific countries, especially ones that operate in a setting of lower healthcare resources. It is our hope that with continued effort and endeavor, sustained progress can be made in improving AMI outcomes in the decade to come.
Go to :
 XML Download
XML Download