

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The physiological assessment of coronary artery disease (CAD) in the catheterization laboratory, including fractional flow reserve (FFR) or non-hyperemic pressure ratio (NHPR) measurement, can identify functionally significant lesions that cannot be reliably detected by invasive coronary angiography alone.1)2)3) Currently, a physiology-based approach has become one of the standard methods for revascularization decision-making.4) In the meantime, imaging modalities have been used to identify vulnerable plaque susceptible to rupture, thus enabling risk prediction before coronary events.5)6) Although functional significance and morphological plaque characteristics have traditionally been regarded as distinct characteristics of CAD, the pathophysiological basis and emerging clinical data have shown a close association between coronary hemodynamics and plaque vulnerability.7) Therefore, it is essential to understand the clinical value and pathophysiological basis of coronary physiology in relation to plaque vulnerability and the functional significance of coronary lesions. In this review, we aimed to explore the fundamental interplay between coronary hemodynamics and plaque morphology during disease progression, provide supporting clinical data for their relationship, and examine the independent and additive prognostic implications of a physiology-based approach along with plaque vulnerability.
Go to : 
PATHOPHYSIOLOGICAL BASIS FOR CORONARY HEMODYNAMIC PROPERTIES AND PLAQUE VULNERABILITY INTERACTION
Defining plaque vulnerability
Acute coronary syndrome is a leading cause of death worldwide,8) with over two-thirds of cases attributable to plaque rupture, in which a plaque ruptures suddenly and leads to the formation of a thrombus and myocardial infarction.9)10) Plaque vulnerability typically refers to a specific type of plaque associated with a high risk of acute coronary events. Thin cap fibroatheroma (TCFA), defined as a thin fibrous cap (<65 μm) with a large lipid pool or necrotic core, has been identified as a vulnerable plaque based on postmortem histopathological studies.11) Microcalcifications, inflammatory infiltrates, such as activated macrophages, cholesterol crystals, and intraplaque hemorrhage, are additional precursors of ruptured plaque.12) Various invasive and non-invasive coronary imaging modalities, including optical coherence tomography (OCT), intravascular ultrasound (IVUS), coronary computed tomography (CT) angiography (CCTA), or near-infrared spectroscopy (NIRS), can identify high-risk plaque features as surrogate markers for vulnerable plaque and clinical outcomes.12)13)14)15)16) Additionally, plaque quantity has been proposed as a determinant of the prevalence and prognostic significance of vulnerable plaque. The prevalence of OCT-derived TCFA correlates with anatomical severity in three-vessel OCT studies.17)18) The relationship between high-risk plaque characteristics and adverse cardiovascular events depended on the presence of a large amount of plaque in several studies,14)19)20) implying that plaque quality and quantity should be considered in defining vulnerable plaque. Moreover, plaque morphology observed at a single time point cannot fully determine the fate of plaque.21) The progression from atherosclerosis to vulnerable plaque and subsequent coronary events is a dynamic process involving continuous interaction of a plaque with the surrounding coronary anatomy and environment, particularly with hemodynamic properties.7)
Role of hemodynamic properties in vulnerable plaque development
Wall shear stress, the normalized tangential force exerted on the vessel wall, regulates the pro-inflammatory pathway perceived by endothelial cells.22) At specific sites within the arterial system exposed to low wall shear stress, atherosclerosis can be initiated by increased inflammatory activity involving the interaction of circulating inflammatory cells and adhesion molecules expressed on the activated endothelial cells.23) This results in the transdifferentiation of monocytes into foams cells and the formation of the fatty streak, which initiates atherosclerotic plaque formation.24) As the plaque grows and luminal narrowing progresses, shear stress increases in the upstream segment of a lesion, and high wall shear stress can promote plaque vulnerability.25)26)27) High wall shear stress can inhibit smooth muscle cell proliferation and induce apoptosis, resulting in the thinning of the fibrous cap and a reduction in total fibrous tissue.28)29) Furthermore, high wall shear stress is associated with vascular inflammation, larger necrotic core, and platelet activation, adhesion, and aggregation, which can increase the risk of rupture.30)31) Ultimately, at the stage of coronary events, excessive mechanical strain can weaken the fibrous cap and cause plaque rupture,26)32)33) thereby increasing the probability of fatal coronary events associated with vulnerable plaque.7) Therefore, hemodynamic properties should be regarded as an essential component of coronary events and a surrogate marker for plaque vulnerability throughout the natural progression of atherogenesis to clinical events (Figure 1).
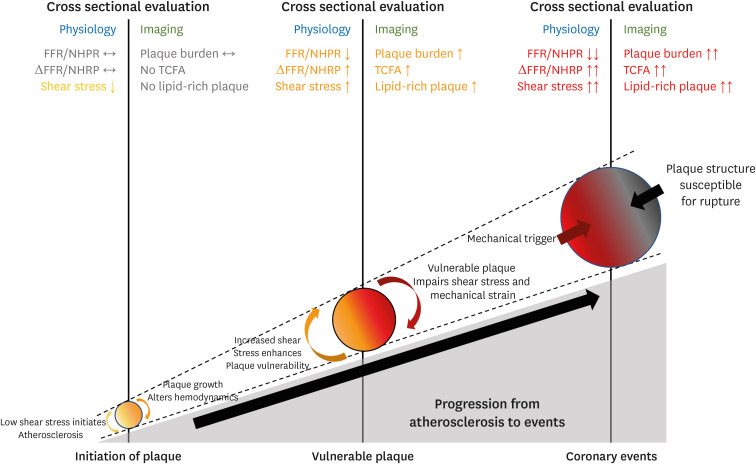 | Figure 1Coronary events developed by the pathophysiological interplay between coronary hemodynamic properties and plaque morphology.Throughout the atherosclerosis progress, coronary hemodynamic properties and plaque morphology continually interact with each other at every step, ultimately leading to subsequent coronary events. At each step, hemodynamic and plaque aspects of coronary lesions can be correlated, which explains the association between physiological indexes and plaque vulnerability on cross-sectional evaluation.
FFR = fractional flow reserve; NHPR = non-hyperemic pressure ratio; TCFA = thin cap fibroatheroma.
|
Go to :
CLINICAL EVIDENCE FOR ASSOCIATION BETWEEN PHYSIOLOGICAL CHARACTERISTICS AND PLAQUE VULNERABILITY
In vivo association between coronary hemodynamics and vulnerable plaque
In vivo studies have demonstrated the relationship between coronary hemodynamics and plaque vulnerability. An initial prospective study using a combination of IVUS and coronary angiography in human coronary arteries reported that non-obstructive lesions with low wall shear stress were associated with increased plaque thickness and outward remodeling.34) This finding was confirmed by the Prediction of Progression of Coronary Artery Disease and Clinical Outcome Using Vascular Profiling of Shear Stress and Wall Morphology (PREDICTION) study, which reported that larger plaque burden and low wall shear stress were independent predictors of plaque progression and luminal narrowing requiring coronary revascularization.35) Another prospective IVUS study further validated the association between low wall shear stress and plaque progression and constrictive remodeling. However, high wall shear stress was related to greater necrotic core progression and expansive remodeling, resulting in a more vulnerable plaque phenotype.27) Furthermore, low and high wall shear stress had a greater predictive value than plaque burden for plaque progression or plaque phenotype,36)37) demonstrating the significant effect of hemodynamics on plaque formation and destabilization.38) Wall shear stress was consistently associated with high-risk plaque features on other imaging modalities. Lipid-rich plaque identified by NIRS and OCT, which are exposed to low wall shear stress, were associated with accelerated plaque growth.39)40) Low shear stress can predict active microcalcifications detected by 18F-NaF positron emission tomography.41) In obstructive lesions, high wall shear stress in the proximal segments was an independent predictor of the presence of OCT-derived TCFA.42) This relationship of low and high wall shear stress with adverse plaque was similarly demonstrated using CCTA-derived adverse plaque characteristics, including low-attenuation plaque positive remodeling, spotty calcification, or napkin-ring sign.43)44)45)46)
Complex association between physiological indexes and plaque quality and quantity
In addition to substantial clinical evidence for the link between hemodynamic properties surrounding a coronary lesion and its vulnerability, several studies investigated the association of physiological indexes that can be measured in the catheterization laboratory with plaque vulnerability (Table 1),47)48)49) demonstrating the prevalence of OCT-derived TCFA was higher in lesions with low coronary pressure or flow indexes. A recent study expanded the association between various physiological indexes and the CCTA-derived plaque quantity and quality.50) High disease burden, characterized by a large plaque burden and small minimum lumen area (MLA), was predicted by resting and hyperemic pressure, and coronary flow reserve. However, resting and hyperemic pressure and microvascular resistance were associated with adverse plaque, defined by low attenuation plaque, and positive remodeling.50) When the association of plaque characteristics with physiological indexes was investigated, impaired myocardial blood flow on [15O]H2O positron emission tomography and FFR were predicted by partially calcified plaques, low attenuation plaque, and positive remodeling, with a value that was incremental over stenosis severity.51) Moreover, in the prediction of FFR ≤0.80, the best plaque metrics interrogated by the machine learning algorithm were MLA, percent atheroma volume, fibrofatty and necrotic core volume, plaque volume, proximal left anterior descending coronary artery lesion, and remodeling index, indicating a complex interaction between luminal stenosis, plaque quantity, and quality, and functional significance.52) How physiological indexes representing a functional status are associated with plaque vulnerability can be appreciated by the correlation of translesional pressure drop with local hemodynamic parameters32)53) and the independent relationship between per-vessel coronary pressure and flow with local shear stress.54)55) Therefore, the use of invasive physiological indexes to define functional significance can also be associated to the identification of plaque vulnerability to some extent.56)
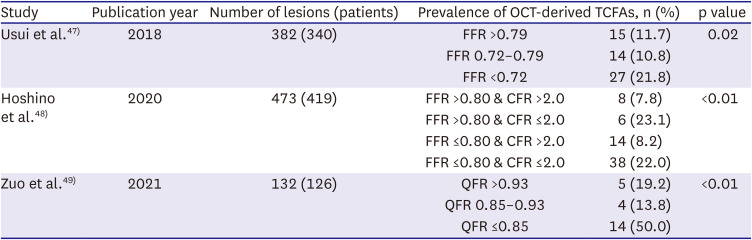
Table 1
Association of physiological indexes with plaque vulnerability
| Study | Publication year | Number of lesions (patients) | Prevalence of OCT-derived TCFAs, n (%) | p value | |
|---|---|---|---|---|---|
| Usui et al.47) | 2018 | 382 (340) | FFR >0.79 | 15 (11.7) | 0.02 |
| FFR 0.72–0.79 | 14 (10.8) | ||||
| FFR <0.72 | 27 (21.8) | ||||
| Hoshino et al.48) | 2020 | 473 (419) | FFR >0.80 & CFR >2.0 | 8 (7.8) | <0.01 |
| FFR >0.80 & CFR ≤2.0 | 6 (23.1) | ||||
| FFR ≤0.80 & CFR >2.0 | 14 (8.2) | ||||
| FFR ≤0.80 & CFR ≤2.0 | 38 (22.0) | ||||
| Zuo et al.49) | 2021 | 132 (126) | QFR >0.93 | 5 (19.2) | <0.01 |
| QFR 0.85–0.93 | 4 (13.8) | ||||
| QFR ≤0.85 | 14 (50.0) | ||||
CFR = coronary flow reserve; FFR = fractional flow reserve; OCT = optical coherence tomography; QFR = quantitative flow ratio; TCFA = thin cap fibroatheroma.
![]()
Go to :
INDEPENDENT PROGNOSTIC IMPLICATIONS OF CORONARY HEMODYNAMICS ON CORONARY EVENTS
Independent role of coronary hemodynamics on coronary events
Given the pathophysiological basis and clinical evidence between coronary physiology and plaque vulnerability, the next question would be whether the hemodynamic assessment is a surrogate marker for plaque vulnerability or an independent predictor for future coronary events. In the Exploring the MEchanism of Plaque Rupture in Acute Coronary Syndrome Using Coronary CT Angiography and computationaL Fluid Dynamic (EMERALD) study that compared CCTA-derived plaque and hemodynamic characteristics between non-culprit and culprit lesions in patients with acute coronary syndrome (ACS),57) the likelihood of culprit lesions significantly increased with the increasing number of adverse plaque characteristics and adverse hemodynamic characteristics (i.e., FFRCT ≤0.80, ΔFFRCT ≥0.06, wall shear stress ≥154.7 dyn/cm2, and axial plaque stress ≥1,606.6 dyn/cm2) (Figure 2). Using the number of adverse plaque characteristics as a mediator in a mediation analysis revealed that adverse hemodynamic characteristics had direct and indirect effects on ACS culprit lesions (Figure 2). These findings indicate that hemodynamic properties may have an independent prognostic impact and a mediating impact through plaque vulnerability on plaque rupture events. Moreover, this notion is supported by previous studies demonstrating a correlation between the shear stress concentration and the plaque rupture site.25)58) High wall shear stress is independently associated with plaque rupture and erosion in patients with ACS.59) Increased plaque structural stress is also associated with a higher risk of ruptured plaque,60) and high wall shear stress derived from three-dimensional quantitative coronary angiography predicted plaque progression61) and impending myocardial infarction (MI).62)63) Therefore, the current evidence suggests that hemodynamic properties can serve as independent prognostic factors for coronary events as well as indicators for vulnerable plaque.
 | Figure 2Prognostic value of coronary hemodynamic properties in relation to plaque characteristics.In the EMERALD study that included 216 lesions from 72 patients with ACS, lesion characteristics were compared between 66 culprit and 150 non-culprit lesions on CCTA taken before ACS events. (A) The correlation of the number of adverse plaque characteristics (i.e., low-attenuation plaque, positive remodeling, spotty calcification, and napkin-ring sign) and adverse hemodynamic characteristics (i.e., FFRCT ≤0.80, ΔFFRCT ≥0.06, WSS ≥154.7 dyn/cm2, and axial plaque stress ≥1,606.6 dyn/cm2) with the proportion of culprit lesions is shown. (B) The mediation analysis investigated the direct and indirect impact of adverse hemodynamic characteristics on ACS culprit lesions mediated by adverse plaque characteristics.
ACS = acute coronary syndrome; CCTA = coronary computed tomography angiography; CT = computed tomography; EMERALD = Exploring the MEchanism of Plaque Rupture in Acute Coronary Syndrome Using Coronary CT Angiography and computationaL Fluid Dynamic; FFRCT = CCTA-derived fractional flow reserve; WSS = wall shear stress.
*The number of adverse plaque or hemodynamic characteristics is shown.
|
Outcome comparison between physiology- and plaque-based approach
The relationship between coronary hemodynamics with coronary events was similarly supported by the clinical data evaluating the relationship between physiological indexes and outcomes. In the international pooled registry with patients who underwent invasive flow and pressure measurement, the 5-year incidence of cardiac death or target vessel MI was higher in patients with low coronary flow reserve or low FFR.64) When treatment decision-making was guided by physiological indexes, revascularized low FFR lesions showed a lower risk of cardiac death or MI than medically treated low FFR lesions in an individual patient-level meta-analysis,65) indicating the efficacy of physiological indexes-based revascularization in treating patient’s vulnerability. In this context that both physiology and plaque assessment may be used to identify and treat the patient’s vulnerability, a recent randomized controlled study tested the non-inferiority of FFR-guided treatment strategy (revascularization if FFR ≤0.80) to the IVUS-guided treatment strategy (revascularization if MLA <3 mm2 or 3 mm2< MLA ≤4 mm2 with plaque burden ≥70%) in patients with intermediate stenosis and demonstrated comparable 2-year outcomes of all-cause death, MI, and revascularization.66) A previous network meta-analysis evaluated the similarity in outcomes following physiology- and imaging-guided treatment, which strongly supports the independent prognostic impact of each modality on clinical outcomes.67) Ongoing studies will shed more light on the direct comparability of physiology-guided and plaque vulnerability-guided treatment.
Go to :
INTEGRATIVE PHYSIOLOGY AND PLAQUE ASSESSMENT AND FUTURE DIRECTIONS
Additive prognostic value of combined physiological and plaque assessment
Since physiological assessment offers prognostic implications independent of plaque vulnerability, obtaining hemodynamic properties and plaque morphology may provide the most comprehensive prognostic data. Several studies have shown the efficacy of integrative physiology and plaque assessment in predicting clinical outcomes. In lesions with FFR >0.80, which can be safely deferred from revascularization according to the current guideline,4) OCT-derived TCFA was present in approximately 25% of lesions and was associated with an increased risk of a composite of cardiac death, target vessel MI, clinically driven target lesion revascularization or hospitalization due to unstable angina until 5-years among patients with diabetes.68)69) This finding was consistent in that IVUS, or CCTA-based adverse plaque features were also independent prognostic indicators in deferred lesions with FFR >0.80.52)70)71) Similarly, in lesions without high-risk plaque, adverse hemodynamic characteristics can distinguish culprit lesions from non-culprit lesions of ACS events,53) indicating that physiological indexes and plaque features can complement each other to define high-risk lesions that a single modality cannot capture. Furthermore, several studies reported that abnormal physiological indexes and adverse plaque features could predict future clinical events synergistically. The likelihood of ACS culprit lesions was higher in lesions with both adverse plaque and hemodynamic characteristics than in those with none.57)72) The risk of vessel-specific composite outcomes was increased proportionally with FFR ≤0.80, high local and global burden, and adverse plaque.73) In a recent report from the first-in-human study of CCTA-derived FFR, the predictability for per-lesion and vessel 10-year outcomes was highest when plaque and hemodynamic predictors were added to baseline clinical and lesion characteristics, suggesting that physiological and plaque components may contribute synergistically even very long-term coronary events.74)
Future perspectives of hemodynamic approach for plaque vulnerability and clinical outcomes
Since standard physiological indexes, including FFR or NHPR, are per-vessel indicators of functional significance, they are limited for assessing the lesion-specific risk for future coronary events.7)21) Recently, novel hemodynamic indexes that can be used in the catheterization laboratory for better lesion-level evaluation, including plaque vulnerability, increased predictability for outcomes, and optimized guiding for appropriate treatment decision-making, have been introduced (Table 2). ΔFFR is a simplified index defined as the difference between the proximal and distal FFR. Several studies have demonstrated that ΔFFR may have additive predictive values for plaque vulnerability and clinical outcomes to FFR.53)57)74) The strength of ΔFFR is its simplicity in that ΔFFR can be obtained using well-defined FFR pullback estimation without additional analysis tools. The prognostic value of ΔFFR or ΔNHPR will be demonstrated further in ongoing studies, such as the Prognostic Impact of Lesion-specific Hemodynamic Index in Patients With Coronary Artery Disease (PRIME-FFR) study (NCT05250557) and the Distal Evaluation of Functional Performance With Intravascular Sensors to Assess the Narrowing Effect: Guided Physiologic Stenting (DEFINE GPS) study (NCT04451044). Pressure pullback gradient (PPG), calculated by the combined maximal pressure gradient and the functional lesion length, can characterize a physiological pattern of a vessel as physiological focal or diffuse CAD.75) Given that percutaneous coronary intervention (PCI) is a local treatment that relieves the pressure gradient of a lesion, the derivation of PPG, in addition to FFR, is expected to define further suitable PCI candidates that benefit from revascularization.76) Radial wall strain is a new index representing lesion-specific biomechanical properties and vessel wall distortion during the heartbeat cycle. Recent studies have shown that high maximal radial wall strain along the lesion segment was associated with a higher prevalence of vulnerable plaque and an increased risk of lesion progression and clinical events in non-ischemic lesions.77)78)79) With these evolving physiological approaches for plaque vulnerability and clinical outcomes, physicians will be in a better position to make decisions and administer treatment to patients with CAD.
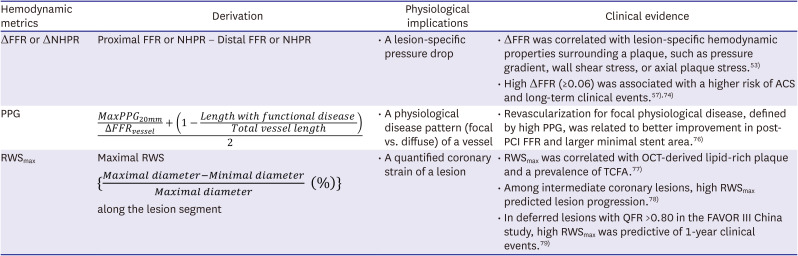
Table 2
New physiological indexes representing plaque vulnerability and lesion-specific hemodynamics properties
| Hemodynamic metrics | Derivation | Physiological implications | Clinical evidence |
|---|---|---|---|
| ΔFFR or ΔNHPR | Proximal FFR or NHPR − Distal FFR or NHPR | • A lesion-specific pressure drop | • ΔFFR was correlated with lesion-specific hemodynamic properties surrounding a plaque, such as pressure gradient, wall shear stress, or axial plaque stress.53) |
| • High ΔFFR (≥0.06) was associated with a higher risk of ACS and long-term clinical events.57)74) | |||
| PPG |

|
• A physiological disease pattern (focal vs. diffuse) of a vessel | • Revascularization for focal physiological disease, defined by high PPG, was related to better improvement in post-PCI FFR and larger minimal stent area.76) |
| RWSmax |
Maximal RWS  along the lesion segment along the lesion segment |
• A quantified coronary strain of a lesion | • RWSmax was correlated with OCT-derived lipid-rich plaque and a prevalence of TCFA.77) |
| • Among intermediate coronary lesions, high RWSmax predicted lesion progression.78) | |||
| • In deferred lesions with QFR >0.80 in the FAVOR III China study, high RWSmax was predictive of 1-year clinical events.79) |
ACS = acute coronary syndrome; FFR = fractional flow reserve; NHPR = non-hyperemic pressure ratio; OCT = optical coherence tomography; PCI = percutaneous coronary intervention; PPG = pullback pressure gradient; QFR = quantitative flow ratio; RWSmax = maximal radial wall strain; TCFA = thin cap fibroatheroma.
![]()
Go to :
CONCLUSION
Plaque vulnerability and subsequent acute coronary events are determined by the continuous interaction between plaque morphology and the hemodynamic properties of the surrounding plaque, which is the basis for the correlation of abnormal physiological indexes with the presence of vulnerable plaque. A coronary physiology-based approach provides an independent and additional prognostic value to a plaque-based approach. Using integrative physiology and plaque assessment, along with emerging physiological indexes, will allow for improved risk assessment and treatment decision-making in the management of CAD.
Go to :
 XML Download
XML Download