

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
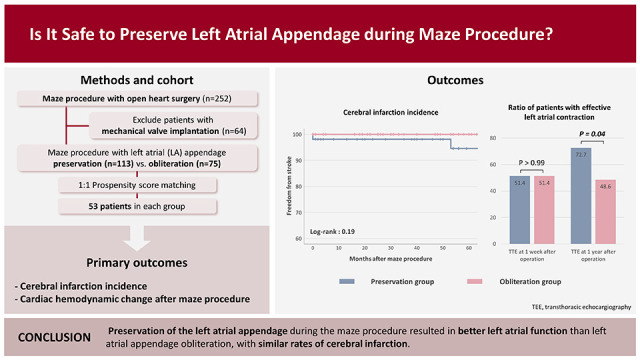
Atrial fibrillation (AF) accounts for 20% of all stroke cases. The risk of stroke is increased 5-fold in patients with non-rheumatic AF, and 17-fold in those with mitral stenosis and AF.1) Furthermore, the left atrial appendage (LAA) is a major source of thrombus formation, which is the main cause of embolization and can trigger atrial ectopic focus.2)3)4) For this reason, LAA occlusion is routinely performed during the maze procedure. However, the LAA contributes to left atrial (LA) mechanical contraction, which is an important factor for increasing cardiac output.5) Moreover, LAA preservation may favorably contribute to appropriate secretion of atrial natriuretic peptides in patients with congestive heart failure.6) Whitlock et al.7) conducted the Left Atrial Appendage Occlusion Study III (LAAOS III; ClinicalTrials.gov number: NCT01561651) and reported that LAA occlusion during cardiac operation reduced the risk of cerebral infarction. However, the preventive effect of LAA occlusion against cerebral infarction remains controversial. In addition, few clinical studies have investigated the hemodynamic effects of LAA occlusion thus far. Therefore, in this study, we compared the surgical, cardiac hemodynamic, and neurologic outcomes between LAA preservation and occlusion performed during the maze procedure.
METHODS
Ethical statement
This study was approved by the Institutional Review Board of the Keimyung University Dongsan Medical Center (Daegu, Korea) (approval number: 2022-12-016; December 13, 2022). The requirement for informed consent was waived due to the retrospective nature of this study.
Study population
This study included patients who underwent the maze procedure using cryoablation (CryoICE Cryoablation Probes, AtriCure, Mason, OH, USA) at our medical center between January 2015 and August 2021 (n=252). Patients who underwent concomitant valve replacement using a mechanical prosthetic valve, or had pre-operative existing spontaneous echo contrast or intra-cardiac thrombus were excluded. We excluded patients with mechanical prosthetic valve because the mechanical prosthetic valve was a well-established risk factor for cerebral infarction after cardiac operation. Patients were classified into 2 groups according to LAA preservation or occlusion during the maze procedure.
Operative techniques
Most patients in this study underwent a maze procedure via complete sternotomy. The techniques for valve replacement, valve repair, and coronary artery bypass grafting were different depending on the surgical period and preference of the surgeon. In the maze procedure, a modified Cox maze procedure using an argon-based flexible cryo-probe was performed with antegrade or retrograde cardioplegia. Patient selection for the maze procedure was based on the factors known to affect sinus rhythm restoration from previous studies, considering LA size and fibrosis, duration of AF, and combined procedure. The absolute indication for LAA obliteration was a history of cerebral infarction or cardiac thrombus; otherwise, the decision to perform LAA obliteration with a maze procedure was made considering the patients’ comorbidity and depending on the surgical period and preference of the surgeon.
Echocardiography and rhythm follow-up
Transthoracic echocardiography (TTE) was performed using commercially available systems with 2.5 MHz transducers (Vivid E95, GE Vingmed Ultrasound AS, Horten, Norway; Acuson SC 2000, Siemens Healthineers, Erlangen, Germany). The results of TTE were reviewed by experienced cardiologists.
During the postoperative hospitalization period, monitoring was performed daily through typical 12-channel surface electrocardiography (ECG). Follow-up TTE was performed prior to discharge and 12 months after surgery. The LA diameter was measured at the apical 4-chamber view or parasternal long-axis view at the end-systole phase. LA volume index and left ventricular volume index were measured using LA or ventricular volume acquired by Simpson’s method from a 4-chamber apical view, indexed to the body surface area.
In patients with sinus rhythm at ECG, transmitral peak velocity and the velocity–time integral of the early (E) and late (A) filling waves were measured at the apical 4-chamber view. The absence of mechanical atrial contraction was defined as the absence of an A wave on TTE,8) and mechanical atrial contraction was defined as there was an A wave on TTE.
During the follow-up period, ECG was performed in the outpatient clinic at 1, 3, and 6 months postoperatively, and subsequently every 6 months. Sinus rhythm restoration was defined as absence of AF recurrence in at least 2 consecutive ECG examinations. The presence of rhythms other than sinus rhythm, including AF, atrial flutter, ectopic atrial arrhythmia, junctional rhythm, or cardiac rhythm of permanent pacemaker (PMK) without atrioventricular synchrony, denoted the failure of sinus rhythm restoration.
Definitions of endpoint
The primary endpoint was the occurrence of major adverse cardiovascular events (MACEs) and the results of TTE during the follow-up period. MACE included the occurrence of cerebrovascular infarction (stroke) suspected to be of thromboembolic origin at any time during the follow-up period, readmission due to heart failure, and PMK insertion. Any symptoms suggestive of neurologic deficit were evaluated by a neurologist through brain magnetic resonance imaging.
Statistical analysis
Normally distributed variables were presented as means and compared using independent t-tests. Categorical variables were compared using Pearson’s χ2 test or Fisher’s exact test and were presented as numbers (percentages). Continuous variables were compared using the 2-sample t-test or Wilcoxon rank-sum test. Continuous data were assessed for normality of distribution using the Shapiro-Wilk test and graphical methods. All statistical tests were 2-sided, with an alpha level of 0.05.
The Kaplan-Meier method was used to estimate stroke-free survival and all-cause mortality; the log-rank test was used for comparisons. Cox proportional hazards regression was used to identify predictors of stroke for the entire patient population tested. Variables with p values <0.20 in the univariable analysis were included in the multivariable analysis.9) The results were reported as hazard ratio (HR) and 95% confidence interval (CI).
Propensity score analyses were used to adjust baseline differences between 2 groups. Prespecified covariates (Table 1) were included in the propensity score calculation. Patients in the non-occlusion and occlusion groups were matched in a 1:1 to 1:4 manner, respectively, using nearest-neighbor matching. After propensity score matching (PSM), the balance between the 2 groups was assessed by calculating the standardized mean difference (SMD) between selected variables, with a standardized mean difference <0.20 suggesting appropriate balance (Supplementary Figure 1), and the discrimination of the propensity score model was assessed using C-statistic (C-statistic, 0.798). Thereafter, continuous variables were compared using the paired t-test, and categorical variables were compared using the McNemar test.
Table 1
Baseline characteristics of the entire cohort
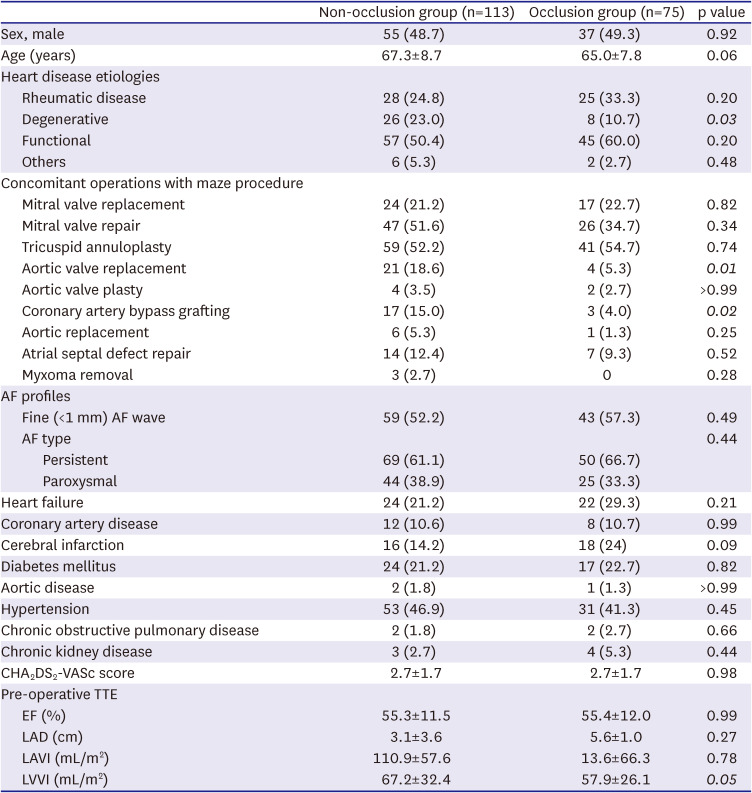
Data are presented as number (%) or the mean±standard deviation. Significant p values are shown in italics. Left atrial volume index and left ventricular volume index were measured using left atrial or ventricular volume acquired by Simpson’s method from a 4-chamber apical view, indexed to the body surface area.
AF = atrial fibrillation; EF = ejection fraction; LAA = left atrial appendage; LAD = left anterior descending artery; LAVI = left atrial volume index; LVVI = left ventricular volume index; TTE = transthoracic echocardiography.
Statistical analysis was performed using the SPSS software version 29.0 (IBM Corp., Armonk, NY, USA) and R statistical software version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Patient characteristics
Between January 2015 and August 2021, a total of 252 patients underwent the maze procedure using cryoablation. Based on the criteria, we excluded 54 (concomitant valve replacement using a mechanical prosthetic valve) and 10 (pre-operative existing spontaneous echo contrast or intra-cardiac thrombus) patients. Eventually, 188 patients were enrolled in the final cohort. The non-occlusion group and occlusion group included 113 and 75 patients, respectively. The median follow-up duration was 44 months (range: 1–94 months).
Patient characteristics are listed in Table 1. Patients in the non-occlusion group were older than those in the occlusion group (67.3±8.7 years vs. 65.0±7.8 years, respectively; p=0.06). The percentage of patients with degenerative valve disease was significantly higher in the non-occlusion group (23.0% vs. 10.7%, respectively; p=0.03). Fewer patients in the non-occlusion group underwent aortic valve replacement (5.3% vs. 18.6%, respectively; p=0.01) or coronary artery bypass grafting surgery (4% vs. 15.0%, p=0.02) as concomitant surgery. Moreover, preoperative cerebral infarction history was less frequent in the non-occlusion group (14.2% vs. 24%, respectively; p=0.09). In pre-operative TTE, the left ventricular volume index was significantly larger in the non-occlusion group (67.2±32.4 vs. 57.9±26.1, respectively; p=0.05).
After PSM, 53 patients from each group were extracted. There were no significant differences in baseline characteristics between the 2 groups (Table 2); the mean follow-up period for the non-occlusion and occlusion groups was 50.0±28.8 and 51.1±24.4 months, respectively.
Table 2
Baseline characteristics of propensity-matched patients
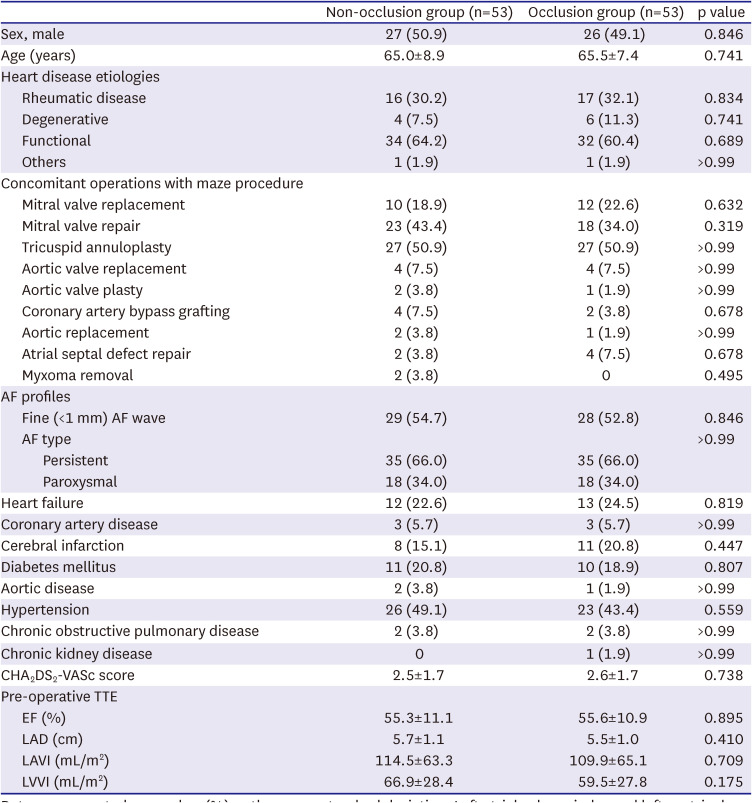
Data are presented as number (%) or the mean±standard deviation. Left atrial volume index and left ventricular volume index were measured using left atrial or ventricular volume acquired by Simpson’s method from a 4-chamber apical view, indexed to the body surface area.
AF = atrial fibrillation; EF = ejection fraction; LAA = left atrial appendage; LAD = left anterior descending artery; LAVI = left atrial volume index; LVVI = left ventricular volume index; TTE = transthoracic echocardiography.
Clinical outcomes
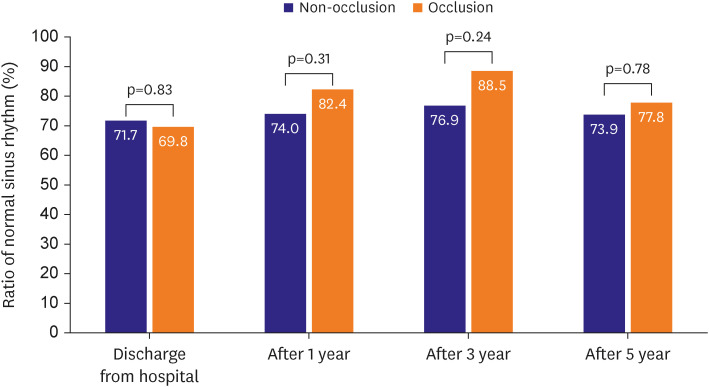
In cohort of propensity-matched patients, hospital stay and postoperative complications were not significantly different between the 2 groups (Table 3). Cardiopulmonary bypass (CPB) time was shorter in the non-occlusion group compared with the occlusion group (143.7±41.2 vs. 160.8±47.4 min, respectively; p=0.06). Significantly more patients in non-occlusion group were managed with warfarin at 1 year after operation (34.0% vs. 18.9%, p=0.03). During the follow-up period, 10 patients underwent PMK insertion (3 vs. 7, respectively; p=0.32). At 1, 3, and 5 years after the operation, the percentages of patients in normal sinus rhythm were 74.0% vs. 82.4% (p=0.31), 76.9% vs. 88.5% (p=0.24), and 73.9% vs. 77.8% (p=0.78), respectively (Figure 1). Likewise, in results of entire cohort, there was no significant difference in ratio of normal sinus rhythm (Supplementary Figure 2).
Table 3
Operative outcomes of propensity-matched patients
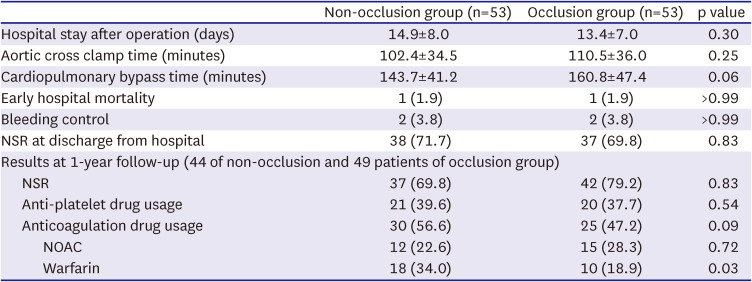
Figure 1
The ratio of patients with normal sinus rhythm after maze procedure of propensity-matched patients.
The results of entire cohort are described in Supplementary Table 1. CPB time was significantly longer in occlusion group (162.7±46.9 vs. 146.2±40.8, p=0.01) and more patients of occlusion group were managed with non-vitamin K antagonist oral anticoagulant (35.7% vs. 20.6%, p=0.03) than occlusion group.
Major adverse cardiac events
In propensity-matched patients, there were 2 cases of cerebral infarction in the non-occlusion group, 5 cases of hospital readmission due to heart failure (non-occlusion group: n=3, occlusion group: n=2), and one case of cardiac death in the occlusion group during the follow-up period (Figure 2). Of the 2 cases of stroke in the non-occlusion group, one patient underwent mitral valve replacement for rheumatic mitral valve insufficiency (5 years after operation, focal infarction at left corona radiate), while the other patient underwent aortic valve replacement for degenerative aortic valve stenosis (7 months after operation, tiny infarction at both postero-cerebral artery territories). Both patients are currently alive, with mild complications from the cerebral infarction.
Figure 2
The results of MACEs during follow-up period after maze procedure.
MACE = major adverse cardiovascular event; PSM = propensity score matching.
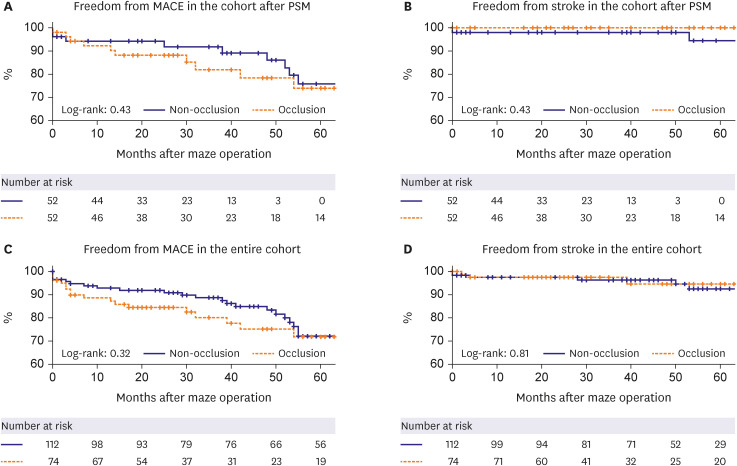
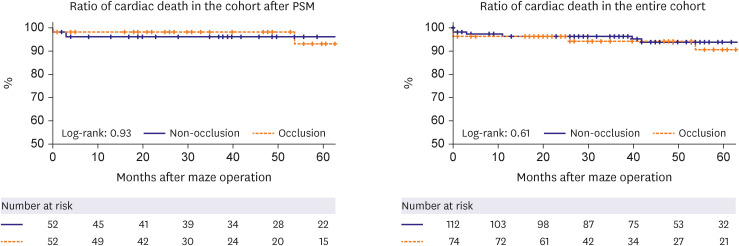
The results of the Kaplan-Meier analysis for long-term freedom from MACE, stroke did not show significant differences between the groups in propensity-matched patients and entire cohort (Figure 2). There was no significant difference in the rate of freedom from stroke (p=0.19), readmission due to heart failure (p=0.74), or permanent PMK insertion (p=0.24) between the 2 groups in propensity-matched patients. The rate of freedom from cardiac death was also not significantly different in propensity-matched patients (p=0.93) and entire cohort (p=0.61) (Figure 3).
Figure 3
The result of freedom from cardiac death ratio after the maze procedure in both groups.
PSM = propensity score matching.
In the entire cohort of patients, multivariable analysis (Table 4) showed that age of patient (HR, 1.085; 95% CI, 1.005–1.172; p=0.04) and rheumatic heart disease (HR, 4.509; 95% CI, 1.115–11.494; p=0.04) were significant risk factors for the occurrence of cerebral infarction.
Table 4
Multivariable analysis for stroke or the entire cohort (Cox proportional hazards regression model)
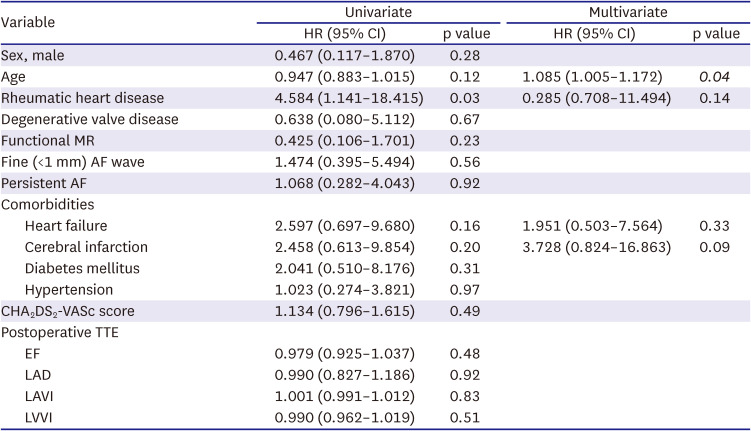
Significant p values are shown in italics.
AF = atrial fibrillation; CI = confidence interval; EF = ejection fraction; HR = hazard ratio; LAD = left anterior descending artery; LAVI = left atrial volume index; LVVI = left ventricular volume index; MR = mitral regurgitation; TTE = transthoracic echocardiography.
Hemodynamic effects of left atrial appendage obliteration
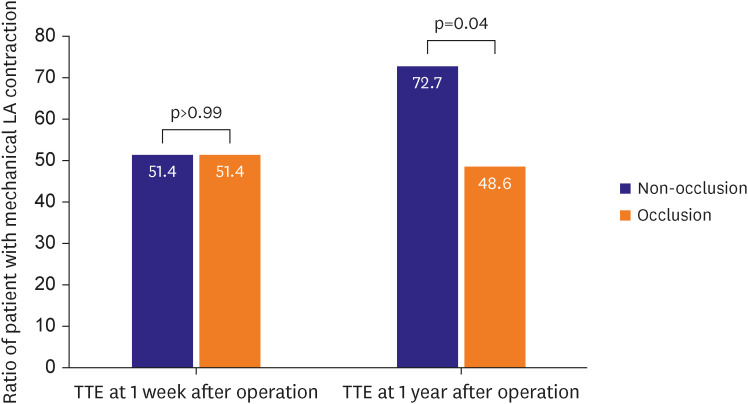
Figure 4 shows the TTE results of patients with normal sinus rhythm in propensity-matched patients. As shown by postoperative follow-up TTE, in those patients, the rate of mechanical LA contraction maintenance was not significantly different between the non-occlusion and occlusion groups (51.4% in both groups; p>0.99). However, this rate at 1-year follow-up was significantly higher in the former group (72.7% vs. 48.6%, respectively; p=0.04). The result of entire cohort (Supplementary Figure 3) was similar, and more patients of non-occlusion group showed effective mechanical LA contraction than occlusion group at 1 year after operation (80.9% vs. 60%, p=0.02).
DISCUSSION
AF is common in elderly patients10) and is responsible for approximately a quarter of ischemic strokes11); of those, many are cardioembolic12) and originate from the LAA.2) In this study, we analyzed the effects of LAA non-occlusion on hemodynamics and the prevention of cerebral infarction. The key finding of this study was that LAA preservation did not significantly increase the rate of cerebral infarction. In addition, LAA preservation significantly improved LA function.
In a recently reported randomized trial (LAAOS III),7) the risk of ischemic stroke or systemic embolism was lower in patients with AF who underwent concomitant LAA occlusion during the cardiac operation than in those who did not. In the LAAOS III clinical trial, the rate of ischemic stroke or systemic embolism occurrence was 7.0% and 4.8% in the LAA non-occlusion group and occlusion group, respectively. These rates were higher than those recorded in the present investigation (3.8% and 0%, respectively) and another study reported by Lee et al.13) (2.5% and 1.7%, respectively). In particular, there was a significant difference in the patients included in the LAA non-occlusion group between the LAAOS III study and the present study. In the LAAOS III trial, only 32.7% of patients (1,562 of 4,770 patients) underwent concomitant surgical ablation of AF. Therefore, although the exact number was not described in this report, most patients may have been at an AF state during the follow-up period. Thus, the LAAOS III trial was focused on patients in an AF state rather than on patients who underwent the maze procedure.
In the multivariate analysis of this study, rheumatic heart disease and advanced age were identified as significant risk factors for stroke, not LAA preservation. In previous studies, rheumatic valve disease and a multiple valvular disease have been linked to worse outcomes, including stroke.9)14)15) However, other reports,9)13) including this study, did not show a significant difference in the rates of stroke between the LAA non-occlusion and occlusion groups. Nevertheless, the relatively small number of patients affected by stroke who are included in studies should be increased to obtain adequate statistical power.
Regarding the effects of LAA occlusion on cardiac hemodynamics, the non-occlusion group showed significantly more frequent LA mechanical contraction on TTE 1 year after the maze procedure compared with the occlusion group. These results showed that preservation of the LAA assisted in the LA booster contribution to ventricular filling, particularly 1 year after the operation. Buber et al.9) and Lee et al.13) also reported superior results of LA contractile in LAA preservation group than LAA obliteration group. This is because the LAA accounts for 17–30% of the total LA volume,14)15)16) and LAA contractile function contributes greatly to the LA transport function.5)9)17) The absence of LA mechanical contraction after the maze procedure should alert physicians to the possible risk of future strokes. Buber et al.9) reported that the absence of LA contraction and an LA volume index ≥33 mL/m2 resulted in a significant increase in the risk of thromboembolic stroke after the maze procedure for patients with sinus rhythm. This finding suggests that LA mechanical standstill is an independent and powerful risk factor for thromboembolic stroke. This should be taken into account when considering anticoagulation treatment for patients following the maze procedure.
This study has several limitations. First, the data in this study were retrospectively analyzed in a small number of cohort. Although several results showed large differences in ratio including the result of more stroke in LAA preservation group despite a more anticoagulant therapy than non-occlusion group, there were not significant differences due to the limited number of cohort. Also, this was not a randomized controlled trial; thus, this study has limited statistical power. Secondly, follow-up screening for AF recurrence was based on serial 12-lead ECG rather than 24-hour Holter monitoring. Hence, it is possible that our results were overestimated because asymptomatic paroxysmal AF may have been present during the follow-up period without appearing on subsequent ECG examinations carried out in outpatient clinics. Third, evaluation for stroke using brain magnetic resonance imaging was performed only in patients with neurological symptoms rather than in all patients. Therefore, it is possible that asymptomatic cases of stroke may have been missed, resulting in an underestimated occurrence rate of stroke in our cohort. Forth, the shapes of appendages are also an important factor for cerebral infarction and LA contractile.18)19)20) However, it is difficult to analyze the shape of LAA on cardiac CT or TTE. The most accurate method to investigate the shape of LAA is external appearance observation during cardiac surgery. Unfortunately, this was a retrospective study using operative records, and most of our hospital's records did not describe the external appearance of the LAA shape. Finally, there was heterogeneity in the indication of concomitant cardiac surgery. For this reason, the impact of concomitant cardiac surgery on outcomes of maze procedure was not totally excluded.
In conclusion, preservation of LAA during the maze procedure effectively maintained LA contractile function. The result of stroke outcome was not significantly different between LAA occlusion and LAA preservation during the maze procedure. However, further long-term studies involving larger patient populations are required to verify the present results.
 XML Download
XML Download