

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Trans-catheter edge-to-edge clip repair (TEER) has emerged as a promising alternative to surgery in patients with severe mitral regurgitation (MR), showing a substantial clinical benefit in high surgical risk populations.1)2)3) The 2020 American College of Cardiology focused update on the MR pathway recommends TEER over surgery for symptomatic functional MR with heart failure.1) However, identifying patients who would benefit from TEER or surgical treatment remains an ongoing debate.
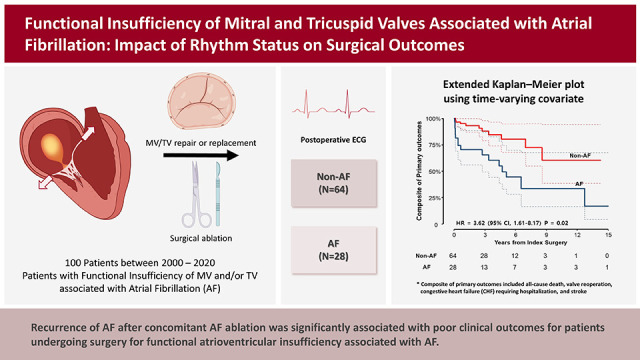
Atrial functional atrioventricular insufficiency refers to atrial fibrillation (AF)-induced functional regurgitation with structurally normal valve leaflets,4) and is mainly caused by atrial enlargement with consequent annular dilatation, most of which are attributable to longstanding AF.5)6)7) Atrial functional atrioventricular insufficiency has received less attention in the past1)8)9); however, there has been growing interest in whether TEER may still be a reasonable option in the presence of AF and annular dilatation.5) Indeed, considering that providing concomitant surgical ablation of AF may be a more desirable therapeutic option, surgical treatment may be preferable over TEER in this particular disease entity. This may also apply to atrial functional tricuspid regurgitation (TR) caused by atrial fibrillation, for which trans-catheter therapy has also increased in recent years.2)3) Intending to contribute to the body of evidence on this issue, we examined the long-term surgical results of atrial functional atrioventricular insufficiency, focusing on the impact of rhythm status on the outcomes.
METHODS
Ethical statement
The study protocol was approved by the Institutional Review Board of Asan Medical Center (approval number: 2021-1683), and the requirement for informed patient consent was waived, considering the retrospective nature of the study.
Patients
We searched the institutional Cardiac Surgery Database of Asan Medical Center (Seoul, Korea) to identify adult patients with persistent atrial fibrillation who showed normal mitral valve (MV)/tricuspid valve (TV) leaflets demonstrated by preoperative imaging and intraoperative findings and underwent mitral valve or tricuspid valve surgery for functional MR or TR between June 2000 and December 2020. Among the 221 eligible patients, those who underwent concomitant coronary artery bypass surgery (n=51) or had a history of major open-heart surgery (n=70) were excluded to form a homogeneous cohort and control for the potential compounding effects of such factors. Finally, 100 patients (mean age, 66.5±10.0 years; 47 males) formed the final study group.
Data acquisition and endpoints
The primary endpoints were adverse clinical events, including all-cause death, reoperation on operated valves, readmission due to congestive heart failure (CHF), and stroke. Readmission for CHF was defined as an unexpected, urgent hospitalization for the management of CHF that meets all of the following criteria: 1) presence of resting dyspnea, 2) radiological signs of pulmonary edema, and 3) need for intravenous diuretics. The secondary endpoint was the incidence of severe TR and/or MR during follow-up.
Surgical procedures
For the surgical approach, a minimally invasive right thoracotomy or a complete sternotomy was used by individualized approach and depending on the attending surgeon’s preference. The techniques used for valve repair, valve replacement, and surgical AF ablation differed depending on the attending surgeon and surgical periods; however, valve repair and concomitant AF ablation were strongly preferred options whenever deemed feasible. A modified version of Cox-Maze III techniques using argon-based flexible cryo-probe has been the standard approach described in a previous study for surgical AF ablation.10)11)
Postoperative management
Standard rhythm monitoring strategy included assessments at 1, 3, 6, 12, 18, and 24 months after surgery and every year after that using 12-lead electrocardiography (ECG), which was augmented by 24-hour Holter monitoring to validate AF-free status in cases that were free-of-AF on snapshot ECGs. Patients with any episodes of AF, atrial flutter, or atrial tachycardia lasting 30 seconds beyond the post-ablation blanking period of 3 months were considered to have AF recurrence,12) and were generally treated with electrical cardioversion or anti-arrhythmic drugs (class I or III). Anticoagulation with warfarin was administered for patients who underwent mechanical valve replacement to maintain a target international normalized ratio of 2.0 to 3.0. In contrast, patients who received annuloplasty rings or bioprosthetic valves were usually prescribed warfarin for 3 to 6 months; subsequent anticoagulation was determined according to the individual patient’s estimated thromboembolic risk and the restoration of sinus rhythm. In the absence of prosthetic mechanical valves, non-vitamin K-antagonist oral anticoagulant was preferred over warfarin in recent years, which was used in individuals who showed persistent AF or in those with a lack of adequate atrial contraction on follow-up echocardiographic assessments even in the absence of AF.
Echocardiographic evaluation
Intracardiac 2-dimensional image and Doppler color flow were obtained in all patients via the transthoracic method. The degrees of valve regurgitation (mild, moderate, or severe) were determined in the standard fashion recommended by the American Society of Echocardiography guidelines.13)14) Follow-up echocardiography was usually conducted 6 months postoperatively; beyond that, echocardiographic tests were done annually or biennially.
Statistical analysis
Continuous variables are presented as means ± standard deviations, whereas non-normally distributed variables are presented as medians with ranges. Categorical variables are presented as frequencies with percentages. One-way analysis of variance or the Kruskal-Wallis test was used to compare continuous variables. In contrast, the χ2 test or Fisher’s exact test was used to compare categorical variables between the three groups. Kaplan-Meier analyses were used to evaluate the conditional probability of overall survival or freedom from reoperation, readmission due to CHF, and stroke, and log-rank tests were used to compare intergroup differences. Univariable and multivariable Cox regression analyses were used to identify the risk factors for primary and secondary outcomes. Factors found significant by univariable analysis (p<0.2) received multivariable analysis with a backward stepwise Cox regression model. Considering the time-varying nature of postoperative AF status during follow-up, postoperative AF was considered a time-varying covariate. The composite primary and secondary outcomes' incidence rates were estimated using an extended Kaplan-Meier method incorporating this time-varying covariate. Time-varying Cox proportional hazard model was used to examine the association between postoperative AF status and clinical outcomes by adjusting for significantly associated baseline variables determined by the multivariable Cox model. The p values of <0.05 were considered statistically significant.
RESULTS
Baseline characteristics and surgical procedures
The baseline characteristics of the 100 study patients are summarized in Table 1. There were 4 patients who had a history of stroke or thromboembolic events. At the time of surgery, 64 presented with predominant TR (≥ moderate), 11 with predominant MR (≥ moderate), and 25 with mixed TR and MR. Surgical AF ablation was performed in 92 patients. The detailed surgical procedures are described in Supplementary Table 1. Most patients underwent valvuloplasty (mitral in 86.1% [31/36]; tricuspid in 98.9% [88/89]), while MV and TV replacements were performed in 5 and 1 patients, respectively. Concomitant AF ablation was conducted only on the left side in 18 (19.6%) patients and on both sides in 74 (80.4%). The left atrium appendage was preserved in 34 (37.0%) patients and excluded in 58 (63.0%) either by resection, clipping, or internal obliteration. Atrial volume reduction plasty was performed on the right side only in 16 patients, left side only in 9 patients, and bilaterally in 9 patients.
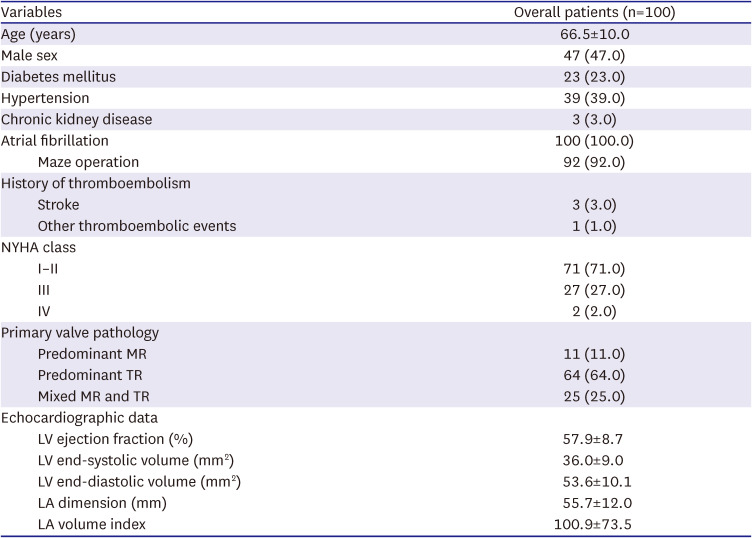
Table 1
Baseline characteristics
Values are number (%) or mean ± standard deviation.
LA = left atrium; LV = left ventricle; MR = mitral regurgitation; NYHA = New York Heart Association; TR = tricuspid regurgitation.
![]()
Clinical outcomes
There were no cases of early mortality (30-day or in-hospital). During a median follow-up of 50.7 months (interquartile range [IQR], 18.4–69.9; 532 patients-years [PYs]), there were 16 all-cause deaths (3.0%/yr), one mitral valve reoperation (0.2%/yr), 14 readmissions due to CHF (2.6%/yr), and five strokes (0.9%/yr) (Table 2). The rate of freedom from composite primary outcomes was 85.7%, 81.5%, and 69.5% at 1, 3, and 5 years, respectively (Figure 1, Supplementary Figure 1).

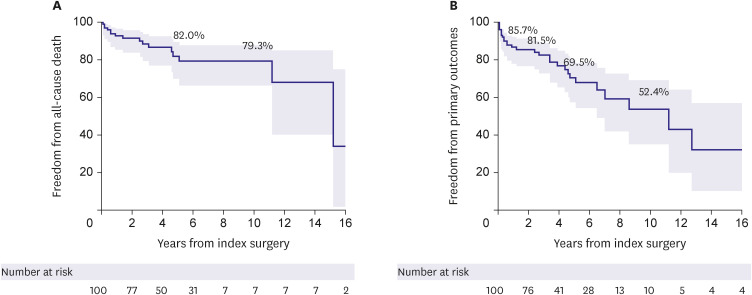
Table 2
The primary outcome with component events
| Variables | No. of patients with event | Event rate* per 1,000 PY | |
|---|---|---|---|
| Primary outcome | 36 | 67.7 | |
| All-cause death | 16 | 30.1 | |
| Reoperation | 1 | 1.9 | |
| Readmission due to congestive heart failure | 14 | 26.3 | |
| Stroke | 5 | 9.4 | |
PY = patients-year.
*Event rates were normalized for the duration of follow-up before the event occurrence.
![]()
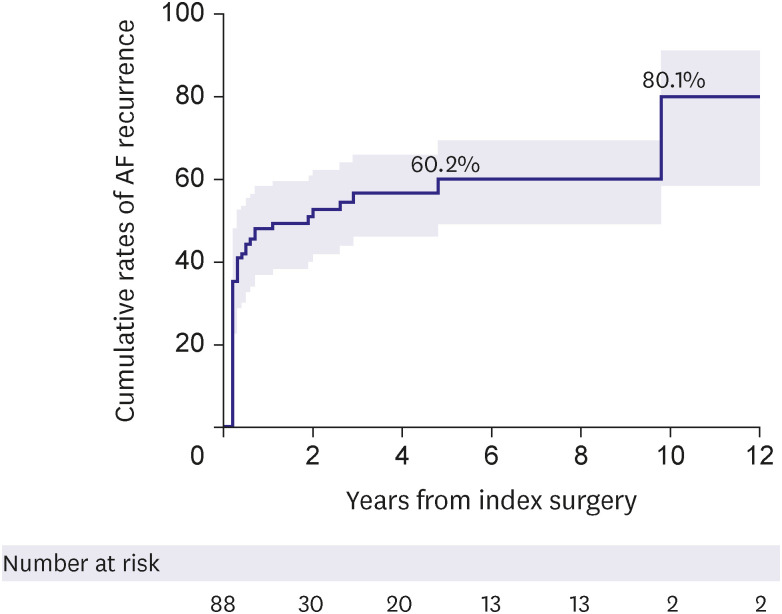
Among 92 patients who underwent surgical ablation, rhythm follow-up over six months postoperatively was possible in 87 patients (94.6%), with a median rhythm follow-up period of 33.6 months (IQR, 16.7–65.1 months). The cumulative incidence rate of AF recurrence was 48.1% at one year and 60.2% at five years (Figure 2). The AF recurrence rates at 1 year were higher in patients who underwent combined MR and TR surgery (65.8%) than in those who underwent TR surgery (43.0%) or MR surgery (36.4%) alone, albeit the difference was not statistically significant (p=0.20) (Supplementary Figure 2).
Risk factor analyses for adverse events
The extended Kaplan-Meier estimator of composite primary outcomes (all-cause death, valve reoperation, CHF, and stroke) based on time-varying postoperative AF status is shown in Figure 3. In univariable analyses, variables that had a p-value <0.2 for the composite primary outcome were age, chronic kidney disease, left atrial appendage exclusion, left atrial volume index (LAVI), New York Heart Association (NYHA) class III/IV, and postoperative AF as time-varying covariates (Table 3). In the final multivariable model, age (adjusted hazard ratio [aHR], 1.06; 95% confidence interval [CI], 1.02–1.10; p=0.005), chronic kidney disease (aHR, 7.76; 95% CI, 2.28–26.38; p=0.001), left atrial appendage exclusion (aHR, 0.35; 95% CI, 0.16–0.78; p=0.010) and postoperative AF (aHR, 3.33; 95% CI, 1.50–7.40; p=0.003) were found as independent risk factors associated with the primary composite outcome (Table 3).
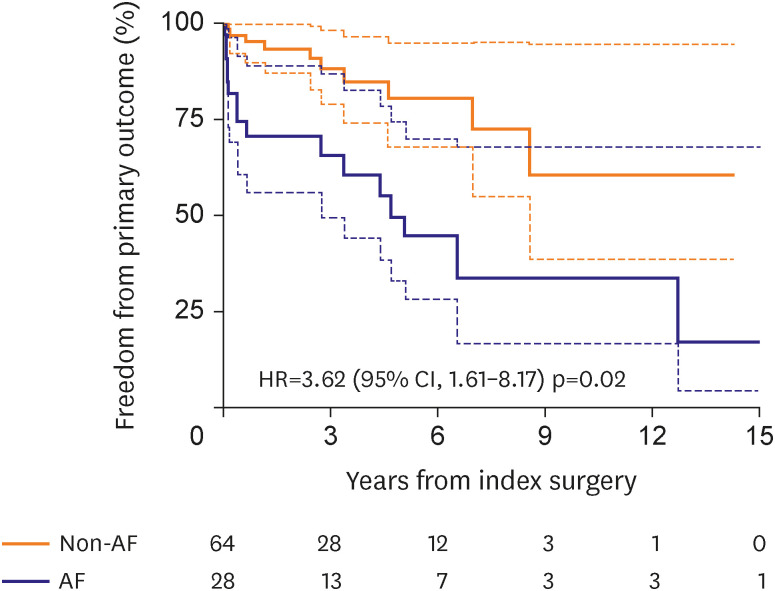
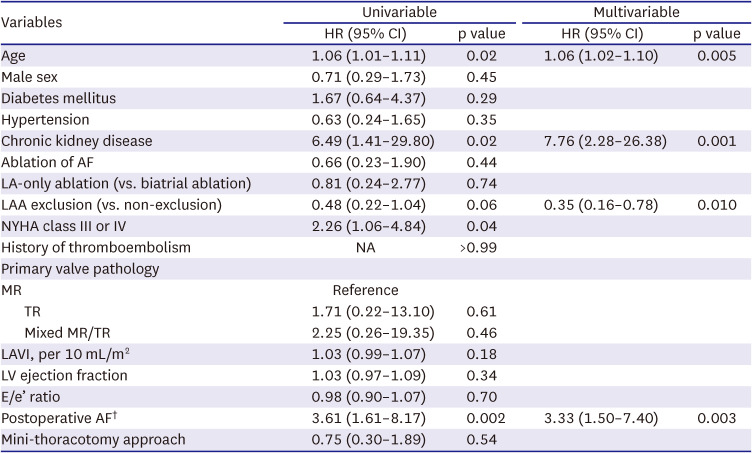
Figure 3
Extended Kaplan-Meier plot using time-varying covariate for the composite of primary outcomes according to postoperative AF.
AF = atrial fibrillation; CI = confidence interval; HR = hazard ratio.
![]()
Table 3
Univariable and multivariable Cox-regression analysis for the composite of primary outcomes*
AF = atrial fibrillation; CHF = congestive heart failure; CI = confidence interval; E = early diastolic mitral inflow velocity; e’ = early diastolic mitral annulus velocity; HR = hazard ratio; LA = left atrium; LAA = left atrial auricle; LAVI = left atrial volume index; LV = left ventricle; MR = mitral regurgitation; NYHA = New York Heart Association; TR = tricuspid regurgitation.
*Primary outcomes: death, reoperation, readmission due to CHF, stroke.
†Considered as time-varying covariates.
![]()
Secondary endpoint: recurrence of mitral and/or tricuspid insufficiency
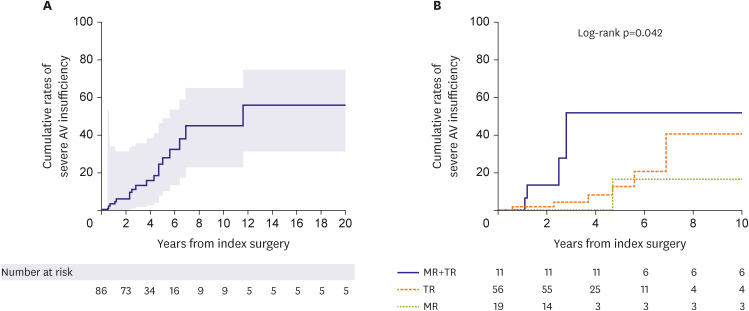
Late follow-up (>6 months) echocardiographic data were available in 85 patients, with a median follow-up duration of 30.2 months (IQR, 10.9–56.7), during which recurrence of severe insufficiency of operated valves was observed in 1 patient in the MV, 7 in the TV, and 4 in both MV and TV. The cumulative rates of severe MR and/or TR recurrence at 5 and 10 years were 18.9±12.1% and 32.4±20.7%, respectively. Patients who underwent combined MR and TR surgery had the highest 10-year rate of recurrence of severe regurgitation (51.9±40.2%), followed by those who underwent only TR surgery (40.6±33.9%) and those who underwent only MR surgery (16.7±20.9%, p=0.042) (Figure 4).
Multivariable analyses that included postoperative AF as a time-varying covariate showed that LAVI (per 10 mL/m2 increment; aHR, 1.06; 95% CI, 1.00–1.13; p=0.049) was an independent risk factor for the recurrence of severe postoperative atrioventricular valve insufficiency (Table 4) while postoperative AF was not significantly associated with the occurrence of the secondary outcome (HR, 1.63; 95% CI, 0.47–5.63; p=0.44).
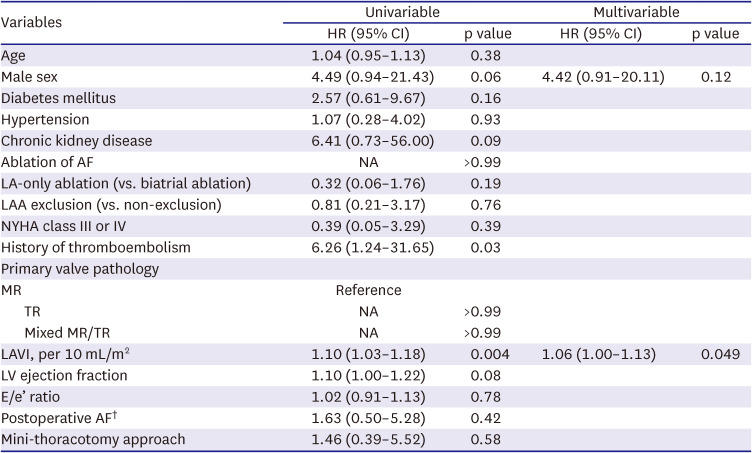
Table 4
Univariable and multivariable Cox-regression analysis for the secondary outcome*
AF = atrial fibrillation; CHF = congestive heart failure; CI = confidence interval; E = early diastolic mitral inflow velocity; e’ = early diastolic mitral annulus velocity; HR = hazard ratio; LA = left atrium; LAA = left atrial auricle; LAVI = left atrial volume index; LV = left ventricle; MR = mitral regurgitation; NA = NYHA = New York Heart Association; TR = tricuspid regurgitation.
*Secondary outcome: severe atrioventricular valve insufficiency.
†Considered as time-varying covariates.
![]()
DISCUSSION
The present study evaluated surgical outcomes of atrial functional atrioventricular insufficiency associated with AF. Despite excellent survival outcomes with no operative mortality and a 10-year survival rate of 79.3% in a cohort with a mean age of 66.5 years, a significant proportion of patients experienced major adverse outcomes such as stroke, CHF, and valve reoperation during long-term follow-up. Moreover, these major adverse events were significantly associated with the recurrence of AF, which was also substantial in its incidence with a cumulative rate of 48.1%, 60.2%, and over 80% at 1 year, 5 years, and beyond 10 years postoperatively. Interestingly, the exclusion of the left atrial auricle (LAA) was significantly protective against the occurrence of primary adverse outcomes, which could be primarily attributed to the lower incidence of stroke compared with preserving LAA.
Functional MRs, in which leaflets of MV are normal, are known to exhibit distinctive pathophysiologic mechanisms in their causes, which have different clinical implications in the corrective intervention of MR.8) Ventricular functional MR—the most common form of functional MR— is primarily caused by the dilated left ventricle (LV) with consequent systolic tethering of MV leaflets in cases such as ischemic cardiomyopathy and dilated cardiomyopathy.15) In this disease entity, TEER is suggested as the preferred option over surgery if intervention is deemed necessary due to high estimated surgical risks stemming from poor LV functions.1) In addition, insufficient evidence for the overt clinical benefits of surgical therapy is another reason for not prioritizing surgery over intervening ventricular functional MR.16)17)18) In contrast, functional MR may also occur by atrial dilation, termed “atrial functional MR.”19) Patients with atrial functional MR are mostly associated with longstanding persistent AF with resultant dilatation of the left atrium (LA) and a mitral annulus; these also induce flattening of the anterior mitral leaflet along the mitral annular plane and posterior mitral leaflet bending toward the LV cavity, traditionally referred as the “hamstringing” phenomenon of the posterior mitral leaflet, all of which are conducive to progressive worsening of MR over time despite essentially normal LV leaflets.5) Given the fairer baseline conditions relative to those with ventricular functional MR and the possibility of eliminating AF—the cause of MR—by the concomitant ablation during surgery, surgery seems to be a more desirable option in atrial functional MR. In particular, as the gap between the anterior and posterior leaflets is more displaced in atrial functional MR by the annular dilatation, capturing these using clipping devices is a technically challenging issue in conducting TEER, which is usually not seen in MR occurring from tethering or prolapse.19)
Functional TR associated with chronic AF is another disease entity that resembles atrial functional MR. As the fibrous skeleton of the TV annulus is less developed than that of MV, atrial functional insufficiency is more easily provoked in the TV than in the MV by longstanding AF, with much overlap in the pathophysiologic mechanisms between the two.20) With the same logic as in the atrial functional MR, surgical therapy may be more justifiable than trans-catheter interventions in atrial functional TR, in which interventional therapy for treating TR has also increased.2)3) With regards to guiding the optimal therapy between surgery and interventional approaches in the atrial functional atrioventricular valve insufficiency, there still are lack of enough data to serve as a reference; therefore, we sought to provide real-world outcomes of surgical therapy, so that the data can be utilized as the benchmark for transcatheter interventions.
The present study demonstrated excellent results of surgical therapy in terms of survival outcome, demonstrating no operative mortality and a fair long-term survival rate. However, major adverse events represented by a composite primary endpoint were not uncommon, with CHF being the most common form of such events with a 10-year cumulative incidence of 24.5%, followed by stroke (15.1%); during the postoperative 10 years, almost 50% experienced a primary outcome. In addition, echocardiographic assessments in the late postoperative periods showed that 18.9% of patients experienced a severe developing insufficiency in the MV or the TV at 5 years and over 30% at 10 years, indicating that the recurrence of atrioventricular valve insufficiency is quite common and occurs in a time-dependent nature. The seemingly disappointing repair durability relative to those observed from previous studies on degenerative MR (mainly prolapse), including those of our series, may be attributable to the different nature of the pathophysiology between these two disease entities.21) More importantly, the durability of valve function yielded by surgery should be compared against benchmark TEER, by which a more significant clinical implication can be obtained to guide the optimal therapeutic option.
Given the limited data available for long-term echocardiographic assessments following TEER for atrial functional MR, a recent large-scale study from the Spanish National Registry Transcatheter MV repair showed this issue.22) In this particular registry, including 1,124 patients undergoing TEER, 48 had atrial functional MR at baseline. At the same time, the degree of atrioventricular valve insufficiency was significantly improved on follow-up echocardiography at 1-year post-TEER, 21.9% still showed advanced MR (grade 3–4), and 33.4% had advanced TR (grade 3–4). Compared with these results from TEER data, the surgical valve durability demonstrated in the present study seems superior, along with excellent early procedural outcomes (i.e., early mortality of 0% in surgery and 2.1% in TEER). Future randomized controlled trials would provide more solid answers for comparative valve durability between surgery and interventional therapy in atrial functional MR.
There has been mounting clinical evidence demonstrating the overt clinical benefit of concomitant AF ablation during cardiac surgery, especially in MV surgery, while the added surgical risks have been perceived to be insignificant.4) While the well-known clinical benefits of this concomitant AF ablation include improvements in long-term survival and reduction in thromboembolic risks, more favorable MV and TV functions should also be noted.23)24)25)26)27) The issue of superior atrioventricular valve function by the AF ablation is crucial in atrial functional MR because the AF contributes as the cause of valve failure, and therefore, combining the AF ablation procedure during valve surgery seems an ideal therapeutic approach.4) The rhythm outcomes, however, seemed relatively poor in the present study. As 92% of patients included in this study underwent concomitant AF ablation, it is regretful that adequate comparisons of outcomes between those with (n=92) and without (n=8) AF ablation are not available due to skewing in the cluster and a small sample size of the “No-ablation” group. Meanwhile, Among those undergoing AF ablation showed high recurrence rates of AF of 48.1% and 60.2% at 1 and 5 years, respectively, which are substantially inferior results as compared with 14.8% and 31.1% in prior studies involving MV for other diseases, such as degenerative prolapse and rheumatic diseases including those from our own experience.11)25) It could be ascribed to different baseline characteristics, including old age, chronicity of AF, the fine wave pattern of AF, and enlarged atria, which have been identified as important risk factors for the recurrence of post-ablation AF.28)29) Of note, patients included in the present study were older (67 vs. 54 years, mean) and had a higher proportion of persistent AF (100% vs. 88%) compared to previous studies.11)25) Also, approximately 20% of patients in this study received left-side-only ablation, which may affect the high incidence of AF recurrence.
Meanwhile, a recent study by Chen et al.4) is noteworthy for speculating the positive impact of concomitant AF ablation in atrial functional MR. In this cited study, 82 patients with atrial functional MR undergoing MV surgery were included, among whom 52 (63.4%) received concomitant AF ablation.4) As a result, patients who restored sinus rhythm showed a significantly superior 3-year rate of freedom from recurrent MR (93.8%) compared with those without AF ablation (44.2%; p=0.035).4) However, these results are somewhat discordant from those of our study because the time-varying Cox proportional models in our study did not show a significant impact of postoperative AF on the development of MR/TR but only with a positive trend in their association (HR, 1.63 on univariable model). Unlike the insignificant association between postoperative AF and valve durability, we observed that postoperative AF as a time-varying factor was significantly associated with primary adverse outcomes. This finding is likely suggestive of the beneficial effect of AF ablation despite its relatively low treatment efficacy in eliminating AF in this cohort, which requires further comparative studies on the intention-to-treat basis. In addition, multiple comparative studies on different methods (i.e., limited vs. full lesion sets) of AF ablation in this particular disease entity should be followed, which would be used for guiding the ideal ablation strategy.
In line with the findings of low AF ablation efficacy and the positive association between postoperative AF and adverse outcomes, LAA exclusion seems to be a reasonable strategy in the surgical treatment of atrial functional insufficiency of MV/TV as demonstrated by our study. As the AF ablation efficacy seems suboptimal due to enlarged atria and chronicity of AF, LAA exclusion may be beneficial in preventing thromboembolic complications, and the present study revealed that LAA exclusion was significantly associated with a lower risk of the primary adverse outcome (HR, 0.35; 95% CI, 0.16–0.78; p=0.010) after adjustment for other significant variables in the multivariable model. Among patients undergoing AF ablation (n=92), the primary discriminatory factor for the risk of primary outcomes between those with LAA exclusion (n=58) and preservation (n=32) was a stroke, which occurred in 1 patient in the exclusion group (0.4%/yr) and 4 patients in the preservation group (2.7%/yr). These findings imply that in cases where the risk of AF ablation failure is expected to be as high as in atrial function MR/TR, the LAA exclusion procedure seems a reasonable approach to prevent long-term thromboembolic events. In addition, if a patient is supposed to undergo transcatheter therapy for atrial functional MR/TR associated with AF, utilizing LAA-occluding devices may also be considered based on the findings of this study.
There are several limitations to this study. First, this study was performed retrospectively at a single tertiary center. Possible selection bias in the choice of surgical procedures for valve repair/replacement or surgical ablation may have affected our study results. In addition, the study population is heterogenous, consisting of predominant MR, TR, or mixed; hence, postoperative outcomes and rhythm control status may differ according to the site of predominant functional regurgitation. Furthermore, as this study included patients who received surgical treatment by 7 surgeons over 20 years, unmeasured confounders such as different levels in surgical expertise and learning curves and evolvement of devices may have yet to be fully accounted for. Second, the number of patients included in this study needed to be larger to provide a robust conclusion; therefore, the results should be interpreted as hypothesis-generating.
In conclusion, surgical outcomes of patients with atrial functional atrioventricular insufficiency were favorable; however, a substantial proportion of patients developed AF recurrence over time despite concomitant surgical ablation for AF, which was associated with poor clinical outcomes. Future studies should focus on the development of more effective ablation strategies to further improve the outcomes of these patients.
 XML Download
XML Download