

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Historically, the management of patients with angina or angina-equivalent symptoms is concentrated on the detection and treatment of obstructive coronary artery disease (CAD). However, up to 40% of patients undergoing invasive cardiac catheterization for the suspicion of obstructive CAD have no evidence of hemodynamically significant epicardial CAD.1) This low yield of coronary angiography applies even to patients suffering typical angina pectoris with non-invasive stress testing suggestive for the presence of inducible myocardial ischemia (ischemia with non-obstructive coronary arteries, INOCA). Patients with angina pectoris and no obstructive coronary artery disease (ANOCA) are at increased risk for adverse cardiovascular events. Moreover, ANOCA patients bear high medical expenses due to repeat hospitalization and re-catheterization because of ongoing symptoms leading to a reduction in quality of life.2) This highlights the need to optimize the diagnostic workup and subsequent management of these patients. Whereas the cause of ANOCA is multifactorial, coronary vasomotor abnormalities are increasingly recognized as the dominant pathophysiological substrate in these patients.
Coronary vasomotor disorders include coronary vasospasm in the epicardial coronary artery and/or coronary microvasculature, or to the presence of impaired vasodilatory capacity upon an increase in myocardial demand due to structural and/or functional alterations in the microvasculature.3) Early identification of these pathophysiological substrates in patients with ANOCA, and initiation of targeted treatments improves quality of life of this complex and heterogeneous patient population.4) However, the diagnosis and treatment of ANOCA in clinical practice continues to be challenging, and systematic approaches are lacking.
This review details a practical approach for diagnosis of ANOCA in clinical practice, and a guide to targeted treatment of the individual endotypes.
Go to : 
NOMENCLATURE
It is important to note that 2 acronyms are currently used interchangeably to describe the presence of angina pectoris in the absence of functionally obstructive epicardial coronary stenosis: INOCA and ANOCA. The acronym INOCA is broadly applied, even in expert consensus documents.5) However, “ischemia” implies that myocardial ischemia has been objectively documented in these patients. In this regard, it is important to realize that patients with angina pectoris often exhibit false-negative results on non-invasive ischemia stress testing, and this occurs more frequently in patients without obstructive CAD.1) As such, many patients with angina and no obstructive epicardial coronary stenosis will not have evidence of ischemia. Moreover, due to the increased use of the coronary computed tomography angiography (CCTA) in patients with stable CAD (as will be discussed in this review), even more patients will undergo a coronary angiography without any information on the presence of ischemia. Therefore, in this review we use the ANOCA acronym to depict the broader and heterogeneous patient population.
Second, various terminology is used to describe the heterogeneous underlying pathophysiology that can be identified in ANOCA patients. The observed patterns of abnormal vasoconstriction of the epicardial coronary artery (epicardial coronary vasospasm), abnormal vasoconstriction of the coronary microcirculation (microvascular vasospasm), and/or abnormal vasodilator capacity of the coronary microcirculation tend to be summarized into various definitions that may lead to unintended perplexity. As we discuss the specific entities subsequently, we will argue why we prefer a direct description of the different pathophysiology identified in the individual patient to improve clarity and facilitate research efforts across the pathophysiological substrates.
Go to :
ANATOMY OF THE CORONARY CIRCULATION
In general, the coronary arterial circulation can broadly be divided into a proximal epicardial compartment and a distal microvascular compartment.6) The epicardial vessels function as conduit arteries and, in the absence of atherosclerotic narrowing, offer limited to no resistance to coronary blood flow (CBF). Consequently, in the healthy coronary circulation, these vessels have no role in the regulation of CBF. The coronary microcirculation consists of the larger pre-arterioles (100–500 µm) and the smaller distal arterioles (<100 µm), which exhibit a particular resistance to blood flow and present the main site of coronary flow regulation. The proximal pre-arterioles predominantly react to changes in shear stress on the vessel wall. The myogenic vasoconstriction in these pre-arterioles is adjusted to maintain coronary arterial pressure at the origin of the arterioles, a process termed coronary autoregulation.7) The smaller arterioles, naturally at a high resting tone, react to the release of vasodilatory metabolites by the myocardial cells during increased myocardial oxygen demand, a process called metabolic adaptation. By reducing or increasing vascular tone and increasing or decreasing vessel diameter, respectively, coronary autoregulation and metabolic adaptation together ensure that microvascular resistance is adapted to accommodate CBF to myocardial demand and maintain perfusion pressure.8)
Go to :
ANGINA WITH NON-OBSTRUCTIVE CORONARY ARTERIES ENDOTYPES AND PATHOPHYSIOLOGY
The clinical syndrome of ANOCA encompasses a broad spectrum of pathophysiological disturbances resulting in coronary vasomotor abnormalities. A normal vasomotor function of the coronary circulation enables the regulation of CBF in order to match myocardial demand by the aforementioned coronary autoregulation and metabolic adaptation.7)8) In response to alterations in myocardial demand, these processes act through dilatation or constriction of the coronary resistance vessels to adapt CBF. Abnormal vasodilator and/or vasoconstrictive responses result in a supply-demand mismatch of CBF accounting for myocardial ischemia of non-obstructive origin.
Evidence regarding the distinct vasomotor disorders in ANOCA is rapidly accumulating and different clinical endotypes of ANOCA have been introduced. These endotypes are based on the presence of abnormal vasodilatation in response to potent pharmacological vasodilators, and/or the presence of vasospastic vascular responses during pharmacological provocation of vasoconstriction. Further, these endotypes are characterized by the vascular compartment where the pathological response is identified, e.g., the epicardial coronary arteries and/or the coronary microcirculation.
Notwithstanding the clinical and scientific importance of identifying all specific pathological substrates and the affected vascular compartment, a practical approach to diagnosis and treatment in ANOCA may first be based on the underlying pathological vascular response, vasospasm or abnormal vasodilatation, which then leads to specific endotyping in the individual patient.
Go to :
ABNORMAL VASODILATION
Pathophysiology of abnormal vasodilation
An impaired vasodilator capacity of the coronary circulation may be associated with angina once the vasodilator reserve capacity of the coronary circulation to accommodate increased myocardial oxygen demand is reduced to levels that interfere with normal activities. As mentioned before, the vasodilator capacity of the coronary circulation is largely owed to the most distal part of the arterial bed: the arterioles. At rest, these arterioles naturally have a high vascular tone, which can be lowered in the presence of increased myocardial oxygen demand by the release of potent vasodilatory substances.9) Of these substances, the most well-known are nitric oxide (NO) and adenosine (Figure 1).
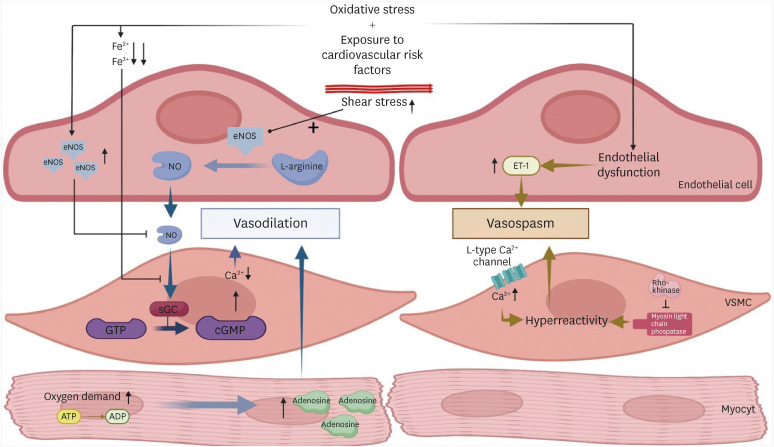 | Figure 1Cellular processes of coronary vasodilation and vasospasm. Schematic overview of the most important pathophysiological processes of coronary vasomotor disorders and the interplay between the endothelial, VSMCs and the myocytes.ADP = adenosine diphosphate; ATP = adenosine triphosphate; Ca = calcium; cGMP = cyclic guanosine monophosphate; eNOS = endothelial nitric oxide synthase; ET-1 = endothelin-1; Fe = iron; GTP = guanosine triphosphate; NO = nitric oxide; sGC = soluble guanylate cyclase; VSMC = vascular smooth muscle cell.
|
NO, considered the most potent vasodilator, is produced and released by the vascular endothelium.10) NO is generated from L-arginine through the activity of the endothelial NO synthase (eNOS). When released from the endothelium in response to physiologic stimuli (i.e., shear stress), NO initiates a cascade through the activation of soluble guanylate cyclase (sGC) that leads to a vast increase in the conversion of guanosine triphosphate to cyclic guanosine monophosphate (cGMP). This in turn leads to a decrease in intracellular calcium (Ca) within the vascular smooth muscle cells (VSMCs) and subsequent vasodilatation. One major prerequisite for the NO-induced activation of sGC is the presence of the reduced (Fe2+) heme moiety. Both heme iron oxidation (Fe3+) and heme removal, which occur due to oxidative stress in the setting of chronic exposure to cardiovascular risk factors, render sGC unresponsive to NO. In addition, NO bioavailability may decline due to a decreased expression of eNOS, reduced substrate or cofactors for this enzyme, alterations of cellular signaling, eNOS inhibition, and accelerated NO degradation by reactive oxygen species. As such, with prolonged exposure to cardiovascular risk factors, endothelial dysfunction may lead to low bioavailability of NO and hence to impairment of the endothelium-dependent vasodilator response of the coronary circulation.
Adenosine, a ubiquitous molecule partaking in several physiological processes within human biology, also acts as a potent vasodilator within the coronary vasculature.11) Adenosine is produced within the cardio myocytes and released by these cells in the presence of increased myocardial oxygen demand. Adenosine subsequently exerts its effects through 4 subtypes of adenosine receptors (A1, A2A, A2B, and A3), which are, amongst others, expressed on cardiomyocytes, vascular endothelium, and VSMCs. Adenosine leads to vasodilation through both endothelium-dependent and endothelium-independent pathways. The A2A receptor is dominant in the endothelium, and its activation leads to the release of NO from the endothelium, which diffuses to the underlying smooth muscle cells and causes relaxation. This effect is mediated by the activation of sGC and the subsequent increase in cGMP levels within the smooth muscle cells. The resulting decrease in intracellular Ca levels leads to smooth muscle relaxation and vasodilation. Adenosine can lead to endothelium-independent vasodilation of VSMCs by directly binding to adenosine receptors on these cells. Activation of adenosine receptors on VSMCs leads to an increase in intracellular cAMP levels, which in turn activates protein kinase A (PKA). Activated PKA phosphorylates various ion channels, pumps, and contractile proteins, leading to VSMC relaxation and vasodilation. This characteristic of adenosine governs its use to study endothelium-independent vasodilatation in the evaluation of coronary vasodilator capacity in daily clinical practice.
Diagnosis of abnormal vasodilation
Traditionally, abnormal vasodilation has been attributed to a reduction in the maximally achievable CBF after pharmacological vasodilatation using adenosine. Secondary to structural changes in the coronary microvasculature (e.g., microvascular obstruction, luminal narrowing, and capillary rarefaction), the vasodilator capacity of the coronary circulation is reduced due to diminished maximal CBF.12) Higher myocardial oxygen demand, such as during exercise, may then cause myocardial ischemia and angina due to CBF supply-demand mismatch. More recently, evidence has accumulated that abnormal vasodilation due to elevated resting CBF carries the same association with myocardial ischemia and increased risk for adverse clinical outcomes.13)14)15) This pattern, typically referred to as functional coronary microvascular dysfunction, is thought to arise from higher resting myocardial oxygen demand at a given myocardial workload, and an ineffective metabolic resting state.16) Disrupted coronary autoregulation could provide an alternative explanation for this pattern. Importantly, abnormal vasodilator reserve capacity can be considered pathologic, regardless of whether it originates from elevated resting CBF or a reduction in maximal CBF.
As mentioned before, the endothelial cells have a crucial role in the regulation of the vasomotor function of the coronary vessels. Endothelial dysfunction is related to an abnormal vasodilator reserve of the coronary circulation as the release of potent vasodilators (mainly NO) is hampered.17) The use of the endothelial-dependent vasodilator acetylcholine (ACh) is the most widely used approach to assess the endothelium-dependent vasodilatory capacity of the coronary circulation. Simultaneous assessment of the vessel diameter and blood flow changes may identify endothelial dysfunction based on an abnormal response to infusions of ACh, as will be discussed later on.18) It is important to note that, as ACh also impacts other vasomotor pathways within the coronary circulation and it may also induce vasospasm.
Importantly, impairment in endothelial-dependent and independent vasodilation can occur solitarily or co-exist in patients with ANOCA.3) Although the exact therapeutic implications are yet to be studied, both entities are associated with impaired clinical outcomes. Therefore, the identification of these endotypes seems important for a comprehensive understanding of abnormalities in coronary vasodilator function.
Go to :
VASOSPASM
Pathophysiology of vasospasm
Coronary vasospasm is characterized by the occurrence of abnormal vasoconstriction and may occur diffuse or focally within the epicardial and the microvasculature compartment of the coronary circulation. Coronary vasospasm is an established cause of anginal symptoms and is often accompanied by evidence of myocardial ischemia on electrocardiography.19) Although the exact pathophysiology is still to be clarified, it is suggested that endothelial dysfunction and hyperreactivity of the VSCMs are the main contributors to the presence of coronary vasospasm.20)21)
In healthy coronary arteries, the interaction between the endothelial cells and the VSMCs is crucial for the regulation of the vascular tone. Various stimuli influence both of these cells in order to alter the vascular tone to accommodate the myocardial blood supply. The endothelial cells act as a moderator by synthesizing and releasing both potent vasodilators and vasoconstrictors that impact the contractile state of the VSMCs. In general, the net effect of these modulators favor vasodilation, but endothelial dysfunction may induce an imbalance in the regulation of the vasomotor tone and for example, reduce the bioavailability of NO in the VSMCs.20) As such, making the VSMCs more susceptible for spasm inducing triggers. In addition, dysfunctional endothelial cells have shown to release a surplus of potent vasoconstrictors, such as endothelin-1. Likewise, it is suggested that coronary vasospasm could also originate from hyperreactivity of the VSMCs. The exact mechanism of VSMC hyperreactivity is yet to be elucidated, but is thought to originate of alteration in the signal transduction pathway between the cellular receptor and contractile proteins within the VSMC. Animal studies have shown that Ca entry through L-type Ca2+ channels into the VSMC is the initial trigger for vasospasm and that these channels are upregulated at a focal site of spasm.22) Moreover, animal studies have also indicated the upregulation of rho kinase at these sites. Rho kinase has a key role in inducing VSMC hypercontraction by inhibiting myosin light chain phosphatase.23)
Diagnosis of vasospasm
Although it is frequently thought that endothelial dysfunction and the presence of VSMC hyperreactivity should co-occur to induce vasospasm, recent clinical observations indicate that coronary vasospasms could be induced in the presence of normal endothelial function and vice versa.3) It is unclear whether a distinction between endothelial dysfunction and VSMC hyperreactivity portends clinically significant value. It is hypothesized that VSMC hyperreactivity is more associated with the presence of focal epicardial spasm and endothelial dysfunction may be the leading cause of diffuse and microvascular spasm. Nevertheless, a systematic understanding on how the interaction between the endothelial cells and the VSMC may induces different phenotypes of coronary spasm is still lacking. At this stage, it is relevant to maintain a general approach to the assessment of vasospasm, and a more tailored approach warrants further elucidation of the underlying pathophysiology.
Go to :
DIAGNOSIS OF ANGINA WITH NON-OBSTRUCTIVE CORONARY ARTERIES DISORDERS
Medical history taking
The clinical presentation of ANOCA is heterogeneous and can be difficult to differentiate from obstructive CAD or non-cardiac pathological conditions. Patients can present with the triad of typical angina pectoris, but often present with atypical anginal symptoms. Breathlessness, indigestion, nausea, extreme fatigue or weakness are frequently reported as the expression of ANOCA.24) On the other hand, there are some key features in the medical history to suggest the presence of vasomotor disorders. In the presence of coronary vasospasm, patients often describe short-lasting and spontaneously occurring episodes of chest discomfort, described as chest tightness, chest pain, or breathlessness.25) These episodes predominantly occur at rest or at night and are often preceded by a period of increased exertion or (emotional) stress. However, exercise-induced symptoms remain common in patients with coronary vasospasm. A clinical response to sublingual nitrate use when symptoms occur further suggests a potential vasomotor disorder, and a trial period of sublingual nitrate use may be helpful in more ambiguous cases. With respect to abnormal vasodilation, the pattern of symptoms can be very similar to that of obstructive CAD, but there is an important sex-difference since female patients are more likely to have ANOCA than men.26) This is importantly related to the clinical presentation since female patients are more likely to present with breathlessness upon exertion as the presenting symptom, making the condition prone to under recognition. Moreover, in our experience, patients with microvascular disease due to abnormal vasodilation, may very well present with long-lasting symptoms, moderate response to nitrates, and symptoms occurring after exertion. In addition, it is important to identify any non-cardiac risk factors related to vasomotor disorders, such as migraine, pregnancy-related hypertension and chronic inflammatory diseases.
Invasive coronary function testing
Ultimately, a comprehensive diagnosis in ANOCA requires evaluation of both vasodilator function and the susceptibility to coronary vasospasm. This requires an invasive coronary study, usually referred to as intracoronary function testing (ICFT). ICFT entails routine coronary angiography to rule out obstructive CAD with certainty, after which the coronary response to pharmacological stimuli is evaluated to document potential vasomotor disorders.
ICFT protocols vary across centers, and the order in which pharmacological stimuli are used is different between centers.27) Specifically due to the impact of the pharmacological stimuli given on the vasomotor function of the coronary arteries. For example, testing for vasodilator function requires the administration of nitrates for maximal CBF measurements that may inadvertently prevent inducible coronary spasm during spasm provocation studies. Despite these differences, coronary spasm provocation is generally performed using intracoronary administration of high-dose ACh, either by bolus administration or by continuous intracoronary infusion. Ergonovine (ER) is used in some centers as an alternative.28) Endothelium-dependent vasodilatation, referred to as endothelial function testing, can be assessed with the administration of low-dose ACh and the change in CBF or coronary artery diameter in response to this administration. The endothelial-independent vasodilator function is assessed by evaluation the CBF response to adenosine, adenosine triphosphate, nicorandil, regadenoson, or papaverine.
Combining these tests, the ICFT provides a comprehensive assessment of the potential pathophysiological substrates of ANOCA. The following paragraphs will discuss our approach to the individual ICFT components in more detail.
Vasospasm provocation testing
The most established way to accurately diagnose coronary vasospasm is by provocation testing with intracoronary administration of high-dose ACh or ER. ACh mediates the release of several endothelium-dependent relaxation factors. Simultaneously, ACh has a direct vasoconstrictor effect on the VSMC. In the presence of a healthy endothelium, the vasoconstrictor effect is normally attenuated by the more potent vasodilator effects. Hence, ACh administration normally leads to a dose-dependent vasodilator response of the coronary artery. However, in presence of endothelial dysfunction or hyperreactivity of the VSCM, the vasoconstrictor response is aggravated and/or the vasodilator effects of ACh are abolished, whereby ACh infusion induces vasoconstriction. ER acts directly and only on the VSMC by activation of serotonergic receptors. ER as such tends to provoke more proximal and focal coronary vasospasm, whereas ACh provokes more distal and diffuse vasospasm patterns.29) Some reports suggest that spasm provocation testing with both ACh and ER increases diagnostic efficacy of vasospasm provocation testing, but this approach is not used in contemporary clinical practice.
As mentioned before, there is a lot of variation in spasm provocation protocols. Only the Japanese Cardiac Society provides a standardized protocol in its guidelines.30) Other centers use center-specific protocols, mainly based on the use of ACh, that differ according to administration routes, infusion times, and doses. To ensure a clinically feasible and comprehensive test including all vascular domains and to allow its routine application in clinical practice, we employ an ACh provocation protocol using manual bolus injections. In our experience, manual intracoronary administration of escalating doses of ACh over a 1-minute period appears to be the most practical and safe method, which allows both evaluation of endothelial function and spasm provocation. Manual intracoronary bolus administration enables the operator to adjust the administration speed in the presence of atrioventricular-conduction disturbances. Hereby, the risk of important cardiac arrhythmias is limited. This approach has a high diagnostic efficacy without the need for temporary cardiac pacemaker, which enhances feasibility of routine ICFT in clinical practice. Furthermore, a protocol including both low-dose and high-dose infusions increases the diagnostic yield of ACh provocation testing. The low-dose administrations (2, 20, and 100 μg i.c.) combined with flow measurements and/or quantitative coronary angiography analysis allow to evaluate the presence endothelial dysfunction. The fourth dose (200 μg) is the spasm provocation dose. It is important to note, that if definitive epicardial vasospasm is induced during the lower doses, there is no indication for further dose escalation. If no spasm is provoked during the interrogation of the left coronary artery, we routinely test the right coronary artery with a single ACh dose of 80 μg. If vasospasm is provoked, we routinely perform a re-challenge with the highest provocative dose leading to spasm during the initial test after intracoronary nitrate administration.31) As microvascular spasms are less likely to resolve by nitrate administration, this allows an enhanced distinction between epicardial and microvascular vasospasm patterns and provides useful insight into the clinical effectiveness of organic nitrate therapy.
Invasive measurement of vasodilator function
During invasive coronary angiography, the use of sensor-equipped guidewires allows to measure the CBF response to endothelium-dependent and endothelium-independent pharmacological vasodilators. Some ICFT protocols apply their use during spasm provocation testing to concomitantly assess endothelium-dependent vasodilator function, whereas other limit their use to study endothelium-independent vasodilator capacity after completion of spasm provocation testing. One of the main coronary arteries is instrumented with a sensor-equipped coronary guide wire, typically the left anterior descending. Currently, a coronary guide wire equipped with a temperature-sensitive pressure sensor (PressureWire; Abbott, Chicago, IL, USA) is employed to measure CBF using either the bolus or continuous flow coronary thermodilution technique. Alternatively, a guide wire equipped with a Doppler flow velocity crystal can be used to measure coronary flow velocity, although the current coronary Doppler flow system (ComboMap and ComboWire/FloWire; Philips-Volcano, San Diego, CA, USA) has been discontinued and its successor has yet to come to market. Nonetheless, the Doppler system is the only one allowing for measurement of beat-to-beat changes in coronary flow in endothelial function assessment, although protocols are emerging for the application of coronary thermodilution for this purpose.32)
As mentioned before, the endothelium-dependent vasodilatation, or endothelial function, can be evaluated during low-dose ACh administration (2, 20, and 100 µg). For this purpose, the change in volumetric CBF is measured before and at the end of each ACh administration. A change in CBF of 0–50% compared to baseline is considered indicative of mild endothelial dysfunction, and a reduction of CBF as severe. Changes in coronary artery diameter on quantitative angiography can be used as an alternative.18) In this case, mild endothelial dysfunction is defined by a change in diameter between +20% and −20%. A reduction in epicardial coronary diameter of less than 20% identifies severe endothelial dysfunction. Severe endothelial dysfunction is most strongly related to adverse events. However, because not all ICFT protocols include endothelial function testing, its position and relevance across the spectrum of vasomotor disorders is subject of on-going studies.
The endothelium-independent vasodilator capacity of the coronary circulation is typically expressed by indices based on invasive coronary pressure and flow measurements at rest and during hyperemia. We use intracoronary (for Doppler flow velocity) or intravenous (for bolus coronary thermodilution) administration of adenosine to induce coronary hyperemia.11) The most frequently used indices to describe the vasodilatory capacity of the coronary circulation are the coronary flow reserve (CFR), the ratio of hyperemic to basal coronary flow, and indices of minimal microvascular resistance (the hyperemic microvascular resistance [HMR] index for Doppler flow velocity, or the index of microcirculatory resistance [IMR] for bolus coronary thermodilution).33) CFR directly reflects the reserve vasodilatory capacity of the coronary circulation to accommodate increases in myocardial demand. Like all biological measurements, CFR reflects a continuum and there is currently no definitive threshold for the presence of abnormal vasodilatation. Previous consensus documents apply a binary cut-off value of 2.0, based on the agreement with the presence of myocardial ischemia in patients with obstructive CAD.5) More recently, evidence emerges that a binary cut-off of 2.5 more accurately identifies patients with an abnormal vasodilatory capacity, and it has been suggested that this threshold equally applies to Doppler flow velocity and bolus coronary thermodilution.34) A CFR of 2.5 was found to be the lower limit of normal in healthy subjects and more accurately correlated with inducible ischemia and impaired clinical prognosis in ANOCA patients.14)15) The indices of minimal microvascular resistance—the ratio between distal coronary pressure and flow at maximal hyperemia—may additionally stratify between abnormal vasodilatation due to an impaired maximal flow (structural abnormal vasodilatation, increased hyperemic resistance) or due to increased resting flow (functional abnormal vasodilation, preserved minimal resistance).13) Although it seems that the prognostic value of this distinction is limited, the clinical value is still to be elucidated. Therefore, the assessment is still warranted in order to identify potential therapeutic targets. Contemporary thresholds for abnormal minimal microvascular resistance are >2.5 mmHg/cm/s for HMR and >25 U for IMR.
Go to :
MANAGEMENT OF ANGINA: INTEGRATING ANGINA WITH NON-OBSTRUCTIVE CORONARY ARTERIES
Ruling out obstructive coronary artery disease
Traditionally, after initial assessment of patients with stable angina, the diagnostic approach is focused on the detection or exclusion of obstructive CAD. In this respect, non-invasive functional modalities (stress magnetic resonance imaging, positron emission tomography, echo) are used to either detect the presence of ischemia-related abnormalities in high-risk patients and anatomical modalities (CCTA) are used to exclude obstructive CAD in low-risk patients.35) Hereafter, the invasive coronary angiography with physiological assessment is the golden standard to rule out obstructive CAD and/or to guide coronary revascularization.
To date, a realignment of diagnostic workup is warranted; including ANOCA disorders in the differential diagnosis of anginal symptoms. The yield of functional non-invasive tests is low in ANOCA patients and does not differentiate between epicardial and/or microvascular disease. As such, either a negative or positive result falsely guides future therapeutic decisions. A more practical approach should include the early distinction between obstructive epicardial disease and potential microvascular disease as the origin of anginal symptoms by CCTA.36) In this respect, it is important to note the potential overestimation of stenosis severity by CCTA and treating physicians should refrain from the dogma of revascularization of every lesion found.37) As such, early distinction and a comprehensive assessment of the clinical presentation enables the trial of early targeted medical therapy and invasive diagnostics reserved to those with persistent symptoms.
Go to :
INVASIVE DIAGNOSTICS: COMPREHENSIVE CORONARY ANGIOGRAPHY
Invasive diagnostics by coronary angiography should be considered only in patients unresponsive to initial treatment or those with high-risk anatomical features of coronary lesions. Ideally, the independent component analysis (ICA) should function as a one-stop diagnostic and include a comprehensive assessment of the epicardial and microvascular coronary circulation (Figure 2). First, the presence of hemodynamically important epicardial lesions should be identified either based on the anatomical characteristics or in combination with physiological measurements (i.e., quantitative flow ratio, non-hyperemic pressure ratios or fractional flow reserve [FFR]).38) If obstructive CAD is excluded, an ad-hoc ICFT should be considered according to recent clinical trial data, limiting the exposure to the risks of the ICA to a single procedure to obtain a definitive diagnosis.4) In this respect, it is important to note the potential influence of nitrate administration prior to ICFT (needed for the assessment of the instantaneous wave-free ratio/FFR and CFR) on the results of spasm provocation testing. However, as we advocate a protocol that could be performed subsequently to a standard diagnostic ICA (ad-hoc ICFT in contrast to the abovementioned elective CFT), ICFT should logically start with the assessment of endothelial-independent vasodilatory capacity of the coronary circulation. Although the feasibility of this protocol is still under evaluation and currently tested within the ILIAS ANOCA study, previous data from the CorMiCa trial has suggested that, likely due to the short half-life of i.c. nitrates (2–3 minutes), spasm provocation testing after routine ICA leads to a similar prevalence of positive ICFT results as those obtained with the conventional ICFT order.4) In clinical practice, this procedure then hardly interferes with the course of the procedure, and allows for comprehensive diagnostics in chest pain syndrome patients referred to the catheterization laboratory. ICFT then enables the ad-hoc identification of the presence of abnormal vasodilation, coronary vasospasm, a combination of both or the absence of both. Moreover, it assesses the presence or absence of endothelial dysfunction and may differentiate between epicardial and microvascular spasm. As such, treatment can be adjusted, stratified and optimized based on the corresponding targets.
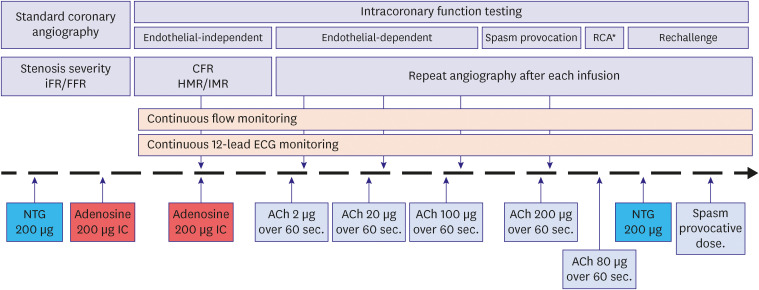 | Figure 2Proposed stepwise protocol for ad-hoc invasive intracoronary function testing. Overview of a stepwise protocol for the ad-hoc assessment of the coronary function, assessing the stenosis severity, endothelial-dependent and independent vasodilatory function and the presence of coronary vasospasm.ACh = acetylcholine; CFR = coronary flow reserve; ECG = electrocardiogram; FFR = fractional flow reserve; HMR = hyperemic microvascular resistance; iFR = instantaneous wave-free ratio; IMR = index of microvascular resistance; NTG = nitroglycerine; RCA = right coronary artery.
|
Go to :
TARGETED TREATMENT
First, it is important to note the lack of large randomized trials providing information on the therapeutic options for patients with vasomotor disorders. Nevertheless, it’s importance is increasingly recognized and recent publications indicate the feasibility of such trials.39) The focus of these trials and of treatment in general should be the reduction of the clinical burden of anginal symptoms, improvement of quality of life, and ultimately, the prevention of future adverse cardiac events.
Pending the results of these trials, there are some potential therapeutic targets that could guide the treatment of vasomotor disorders. First, standard life-style interventions should always be the foundation of treatment in patients with angina pectoris, limiting the progression of CAD and the exposure to vasospasm inducing conditions.40) In addition, it has been shown that early detection and endotype-based treatment strategies of ANOCA improves patient-reported clinical outcomes significantly.4) It is important for physicians treating patients with anginal symptoms to familiarize themselves with the specific strategies. Figure 3 depicts an overview of the respective treatment algorithms that are part of the randomized ILIAS ANOCA trial.
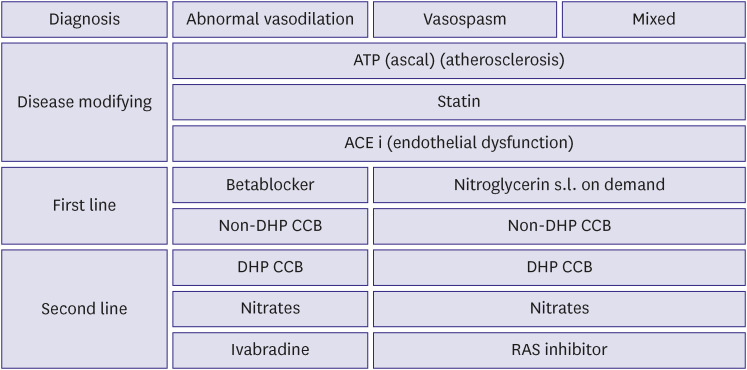 | Figure 3Proposed stepwise protocol for the pharmaceutical therapy of vasomotor disorders. General overview of possible pharmaceutical options in the treatment of vasomotor disorder.ATP = adenosine triphosphate; ACEi = angiotensin-converting enzyme inhibitor; CCB = calcium channel blocker; DHP = dihydropyridine; RAS = renin-angiotensin system.
|
Treatment of abnormal vasodilatation
The pathogenesis of abnormal vasodilation is similar to that of obstructive epicardial CAD. These patients are often exposed to similar risk factors and show similar increased risks of adverse cardiac events.15) Hence, if isolated abnormal vasodilation is diagnosed, the first step in therapy is the reduction of cardiovascular risk factors and induce endothelial regeneration by initiating statin therapy and angiotensin-converting enzyme (ACE)-inhibition.41) In addition, anti-platelet therapy should be considered in patients with a high atherosclerotic burden. Simultaneously, medical therapy reducing myocardial oxygen consumption in order to decrease anginal burden in these patients should be considered with beta-blockers or Ca channel blockers. If symptoms persist, combining multiple modalities could be considered.
Treatment of coronary vasospasm
In contrast to the treatment of abnormal vasodilation, the treatment of coronary vasospasm is more diverse and challenging. Similarly, these patients may benefit from baseline therapy with statins and ACE-inhibitors for cardiovascular risk reduction and endothelial regeneration. However, standard pharmacological therapy to reduce angina burden often disappoints and treatment with beta-blockers might even increase the risk of vasoconstrictive episodes.42) Nitrate therapy may be beneficial in some patients, but the efficacy varies and the use of nitrates should optimally be guided by the results of the re-challenge during spasm provocation testing.31) Patients with abnormal vasoconstriction, especially those with evident abnormal vasoconstriction in the epicardial arteries, often benefit from Ca antagonist therapy.43) Sometimes in unusual high-dosage or in combination with other drugs. Several studies have been conducted with respect to other potential therapeutic targets to reduce angina burden in these patients. Ranolazine, trimetazidine and nicorandil were all found to improve microvascular perfusion.44)45)46) However, medical treatment of coronary spasm remains largely empirical, and future research is critical to explore the potential of these medications and to identify novel therapeutic targets.
Go to :
CONCLUSION
The interest and recognition of ANOCA as a contributor of anginal symptoms is evolving rapidly. As such, it has become increasingly clear that a general understanding of the diagnosis and treatment of ANOCA endotypes is warranted for all physicians encountering patients with anginal symptoms. We provided a general overview of pathology, diagnosis and treatment of different ANOCA endotypes and as such, aimed to provide a practical approach in the treatment of ANOCA.
Go to :
FUTURE PERSPECTIVES
In patients with anginal symptoms, the paradigm of management is shifting from an obstructive-only towards a more inclusive perception with attention for ANOCA. Historically, the use of ICFT was reserved for patients with persistent anginal symptoms, but the CorMiCA-trial indicated that ad-hoc ICFT in patients with stable angina improves quality of life. Future studies, like the ILIAS ANOCA and the iCorMiCA should further determine whether the ad-hoc ICFT should be incorporated as standard of practice. Moreover, several clinical registries are including outcomes of diagnostic ICFT’s and should provide insights in different risk factors.47) Lastly and most importantly, future research should focus on the identification of specific therapeutic targets and the medical treatment of ANOCA.
Go to :
 XML Download
XML Download