

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A well-balanced nutrition program is the first step in optimizing athlete performance [1]. Sports nutrition is generally dominated by a normal Western diet and meals containing animal-derived protein (e.g., red meat and eggs). Popular diets (gluten-free, ketogenic, intermittent fasting, and vegetarian diets) are less commonly embraced, considering their health and ergogenic effects [23]. Athletes must follow a well-balanced nutrition program because they have high energy demands and metabolic cycles [4]. Plant-based foods should be part of a nutrition program that reflects the nutritional quality and sufficiency. Plant-derived foods form the basis of a healthy diet because they include polyphenols and dietary fiber, and the availability of plant-derived components determines the diet quality [5]. Integrating plant foods into a diet is also vital for achieving environmental sustainability. Food production of animal origin requires more energy, land, and water. Therefore, plant-based diets use fewer natural resources and have less environmental impact than animal-based diets [6]. A recent study highlighted the relevance of sustainable production and healthy consumption among athletes [7]. The Mediterranean diet model is the most healthful, sufficient, and practical of sustainable diets [8]. The Mediterranean diet provides a high intake of vegetables, fruits, nuts, and olive oil; a moderate intake of fish and poultry; a low intake of dairy products, red meat, and processed meat; and moderate alcohol use, preferably in the form of red wine [9]. Following a Mediterranean diet and lifestyle can induce physiological changes in athletes, promoting their health and performance. Plant-based foods are high in carbohydrates, which help glycogen storage replenish efficiently. The antioxidants they contain mitigate inflammation and oxidative stress [10]. High fiber intake modulates the intestinal microbiota and enhances variety [11]. These physiological mechanisms establish a robust scientific basis that the Mediterranean diet might improve athlete performance. Nevertheless, the performance benefits of diet remain elusive because of the paucity of dietary intervention studies and data.
The high ability to recover is essential to optimizing an athlete’s performance. Recovery is crucial because it is during this time that all exercise-related adaptations take place [12]. Lactate accumulation during exercise leads to muscular fatigue and a lower repeat performance in sequential training if not eliminated during recovery. Blood lactate elimination is used to assess the recovery rate [13]. Some dietary components can help reduce the lactate levels during and after exercise. These are antioxidant vitamins and polyphenols found abundantly in the Mediterranean diet [141516]. In addition, alkaline beverages and foods are reported to help reduce lactate accumulation [1718]. Most fruits and vegetables are alkaline. They are abundant in the Mediterranean diet in the form of fresh, cooked, or freshly squeezed [919]. The Mediterranean diet score is negatively associated with the dietary acid load. Therefore, the Mediterranean diet is suitable to be adjusted as alkaline [20]. Previous studies reported that alkaline diets and the Mediterranean diet have beneficial properties for physical performance [2122]. This research was designed assuming that an alkaline diet prepared according to Mediterranean diet principles will have a greater impact on athlete performance and lactate levels. Young athletes, in particular, have been reported to have weaker adherence to the Mediterranean diet [23]. As a result, adolescent athletes are considered the best candidates for a Mediterranean diet intervention. This study examined how an isocaloric, low-acid load Mediterranean diet model affects aerobic performance, anaerobic power, fatigue (perceptual measures), and recovery (lactate measurement) in adolescent athletes.
Go to : 
SUBJECTS AND METHODS
Location, time, and duration of research
In June 2021, the research was conducted with athletes from TOHM (Turkey Olympic Preparation Center) and SEM (Athlete Training Center), which are affiliated with the Bolu Provincial Directorate of Youth and Sports in Turkey. In the research performed at Gerede Arkut Skiing Center, the performance, lactate, body composition, and anthropometric measurements of athletes lasted 4 days, whereas the dietary intervention took 15 days. This study was approved by the Ankara University Faculty of Medicine Human Research Ethics Committee with a decision dated 14.01.2021 and numbered 11-27-21.
Characteristics of the participants
The research included 15 male athletes who were interested in ski-running sports. The inclusion criteria were male athletes between the ages of 13 and 18, who followed a high-protein sports diet, did not have any chronic diseases, could follow the nutrition plan supplied by the researcher, and voluntarily participated in the study. Athletes and their families who met the inclusion criteria were informed about the research purpose, method, expected benefits, and risks. The participants were included in the research after obtaining informed consent.
Data collection
The data were collected by a multidisciplinary team consisting of a dietitian, trainer, doctor, and cook. During the study, the research coordinator provided regular training to the team and volunteer participants. The research participants were given a Mediterranean diet to follow for 15 days. In studies investigating the effects of Mediterranean-style and low-acid-loaded nutrition on performance, the duration of the dietary intervention varied between 2.5 and 9 days [22242526]. Because the main aim was to determine the effects of diet on performance, the duration of the dietary intervention was determined to be 15 days. The performance, lactate, body composition, and anthropometric measurements of the athletes were taken before and after the dietary intervention. The information collected was entered into a questionnaire form that included a personal information section and the sections for the measured parameters.
Dietary intervention
An expert dietitian carried out the menu planning and diet intervention process. The diet was planned according to the Mediterranean diet model, considering the athletes’ energy and nutrient requirements. While planning the menu, care was taken to include vegetables, fruits, and cereals in every main meal. Low-fat dairy and plant-based non-dairy products (e.g., coconut and almond milk) were preferred. Seafood and legumes were provided twice or more per week, white meat once per week, red meat once per week, and eggs 4 times a week. Sugar was excluded from the diet. Spices, onion, and garlic were frequently preferred, and olive oil was used in all meals [9]. Drinks were prepared from honey and dried and fresh fruits to meet the energy requirement.
The menu was prepared so that the potential renal acid load (PRAL value) was negative to increase the alkalinity in bodily fluids. PRAL was calculated as follows [27]: PRAL (mEq/day) = 0.4888 × Protein (g/day) + 0.0366 × Phosphorus (mg/day) − 0.0205 × Potassium (mg/day) − 0.0125 × Calcium (mg/day) − 0.0263 × Magnesium (mg/day) in the menu consisting of 6 meals, the PRAL value was set to negative. Thus, it was desired to maintain alkalinity in the bodily fluids. A negative adjustment of the PRAL value of each meal enabled the total PRAL value from the daily foods to be far from zero. This reduced the probability of returning the total PRAL value from all meals to positive at the end of the day because the participants chose and consumed foods with positive PRAL values. The combination of a low renal acid load diet and the Mediterranean diet rules restricts the variety and quantity of some foods on the menu. Foods, such as seafood, rice, pasta, oats, and walnuts, whose consumption is more unrestrained in the Mediterranean diet, were kept low because of their PRAL levels. Seasonal foods were chosen with care. Despite this, out-of-season frozen products were also included in the diet to adjust the PRAL value and provide diversity.
The recommended daily energy requirement for active male adolescents is 2,800–3,200 kcal [28]. The amount of nutrients and portion sizes in the meals and drinks in this research were designed to provide energy from the upper limit (3,200 kcal/day). The amount of food consumed was recorded by checking the athletes’ plates at the end of each meal, and their adherence to the diet was followed up. They received an average of 2,973.5 ± 186.4 kcal energy. The recommended ratios for the energy distribution derived from the macronutrients were 55–65% for carbohydrates, 15–20% for protein, and 20–30% for fats [28]. The energy from macronutrient ratios in the given meal was within the recommended range (carbohydrate 56%, protein 16%, and fat 28%). Athletes should consume vitamins and minerals in line with the recommended daily allowance [28]. The given menu satisfied more than the recommended amounts because of the nutritiveness of the Mediterranean diet and high energy demand.
The standard and specially prepared recipes used the ingredients and amounts included in the meals and drinks [29]. The athletes’ chefs prepared the meals. The amounts of food and portioning were calculated using precision kitchen scales. All the athletes remained in the athlete training center during the diet intervention (15 days). This study ensured that the athletes consumed just the food provided throughout the camp because there was no place to buy food around the training center.
Performance and lactate measurements
The hand grip strength, vertical jump test, and 20-meter shuttle run test were used to evaluate the participants’ performance. The Borg fatigue scale was applied during the shuttle run test. The lactate levels were measured while at rest after the test. The athletes’ trainers took the performance and lactate measurements.
1) Hand grip strength
A Takei T.K.K. 5401 Grip-D (Takei, Tokyo, Japan) hand dynamometer was used for the hand grip strength measurements. The measurements were taken while the athletes stood with their elbows and wrists fully extended [30]. The measurements were repeated 3 times in the dominant and non-dominant sides, and their averages were calculated.
2) Vertical jump test
Active and squat jumps were performed for the vertical jump testing. In active jumping, as soon as the athletes felt ready, they quickly collapsed from the upright position by placing their hands on their waists and jumped upwards with the maximal strength. In squat jumping, the athletes jumped upwards by applying the maximal force without any downward movement by placing their hands on their waists and flexing their knees 90°. The jump heights were recorded in centimeters. The vertical jump heights were calculated using the My Jump 2 program. The My Jump 2 application is reported to provide extremely valid and reliable values as a force platform [31].
Body weight is factored out in the vertical jump test. Heavier athletes may have a shorter jump distance but more power. For this reason, the anaerobic power was calculated using the Lewis method from the body weight and jump height. The anaerobic power was calculated using the following formula [32]:
3) Twenty-meter shuttle run test
The shuttle run test is a field test used to estimate cardiovascular fitness in situations where the maximum oxygen consumption of individuals cannot be calculated using a laboratory-based test. A meta-analysis study reported that a 20-meter shuttle run test has medium-high validity in predicting cardiovascular fitness [33]. The test was conducted on a flat surface with marks at the start and finish of a 20-meter area. The athletes were given a signal tone and asked to be within a 2-meter area in front of the start and finish lines at each signal tone. The athletes were requested to step on the start and finish lines at the end of each shuttle, which started at 8.5 km/h and was increased by 0.5 km/h every minute. Each signal received by the athletes was recorded as a shuttle, and each shuttle missed was considered a mistake. The test was terminated when an athlete committed 2 consecutive mistakes [34]. The maximum heart rates were recorded with a polar watch at the end of the shuttle run test. The following formula was used to calculate the maximum oxygen consumption [34]:
4) Borg fatigue scale
The Borg fatigue scale was used to determine the perceived difficulty level during exercise; the scale ranged from 6 to 20 [35]. The participants were asked to rate their level of fatigue on a scale before each speed increment (1-min intervals) during the shuttle run test.
5) Lactate levels
Using a lancet and needle, 12 blood samples were taken from the athletes, including once before the shuttle run test and 11 times (3-min intervals for 30 min) after the shuttle run test (at the resting state). The blood samples were analyzed using the Arkray Lactate Pro2 device (Arkray, Kyoto, Japan) and the appropriate strips. The lactate measurement interval, measurement time, and lactate elimination were established according to Fleming et al. [36]. The time elapsed during a 50% reduction of the peak lactate concentration was calculated in seconds [36].
Body composition analysis
Using the bioelectrical impedance method, the Tanita MC 780 body analyzer (Tanita, Arlington Heights, IL, USA) was used to determine the body composition. The body weight, body fat percentage (%), lean body mass (kg), total percentage of body water (%), and bone mass (kg) were all calculated using this method.
Anthropometric measurements
The athletes’ anthropometric measures were taken using an inelastic tape measure in the morning following an overnight fast. The height, waist circumference, hip circumference, and upper-middle arm circumference were measured. The athletes’ heights were measured with their feet together, head position in the Frankfort plane, and eyes and superior border of the earlap at the same level. The waist circumference was measured as the circumference passing through a point between the lower rib bone and crista-iliaca while holding both arms and feet together. The largest region of the hip was measured to calculate the hip circumference. The waist-to-hip ratio was computed by dividing waist circumference (cm) by hip circumference (cm). While the athletes were standing and upright, their upper-middle arm circumference measurements were performed by flexing the arm 90° from the elbow and designating a point between the acromion process on the shoulder and the olecranon process on the elbow. The circumference measurements were recorded in cm starting at the designated point [3738].
Statistical analysis
The Nutrition Information Systems (BeBiS) program (full version 8.2; Nutrition Information Systems, Istanbul, Turkey) was used to calculate the energy and nutrient values of foods in the study. The Statistical Package for Social Sciences 21.0 (SPSS 21.0; IBM Corp., Armonk, NY, USA) program was utilized to analyze data and produce tables. Descriptive analyses with the mean and standard deviation were used for continuous data. The categorical data are presented as percentages. The Kolmogorov-Smirnov and Shapiro-Wilk tests were used if the data had a normal distribution. The Kolmogorov-Smirnov and Shapiro-Wilk tests were applied to test whether the data showed a normal distribution. In the pre- and post-intervention comparisons, the dependent sample t-test was used to analyze normally distributed data. In contrast, the Wilcoxon t-test was employed to analyze non-normally distributed data. A P-value > 0.05 was considered statistically significant in all statistical analyses. Graphics were produced using the GraphPad Prism 9 program (GraphPad Software Inc., San Diego, CA, USA).
Go to :
RESULTS
General characteristics of the participants
Table 1 lists the general characteristics of the participants. Their average age was 14.9 ± 1.3 yrs, and they had been participating in sports for 3.9 ± 1.6 yrs. Their mothers had an average age of 39 ± 5.6 yrs, while their fathers had an average age of 42.1 ± 5 yrs. All the participants had siblings, with the average number being 3.3 ± 1.3. Regarding parental education, 40% of mothers completed primary school, and 53.3% of fathers completed high school. In 46.7%, a family member had a sporting background. The rate of those with a nuclear family structure was 80%. The rate of those who stayed in the sports training center was 86.7%.
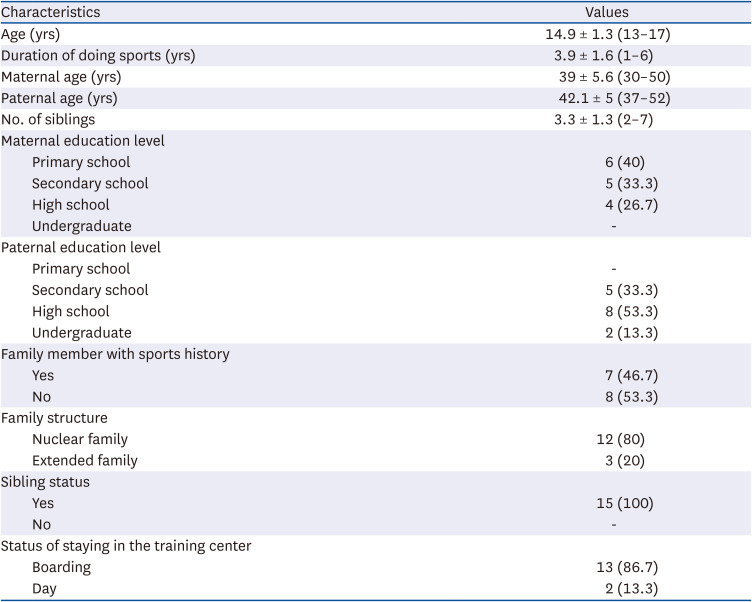
Table 1
Data on the general characteristics of the participants (n = 15)
![]()
Energy and nutrient intakes of the participants
Table 2 lists the daily mean energy, macronutrient, and PRAL values of the foods consumed by each participant. The average amount of energy intake was 2,973.5 ± 186.4 kcal. Carbohydrates, proteins, and fats provided 56.6%, 15.8%, and 27.6% of the daily energy on average, respectively. The average PRAL value of the diet they consumed was −36 ± 3.3 mEq/day. All participants conformed well to the diet for the entire 15 days.
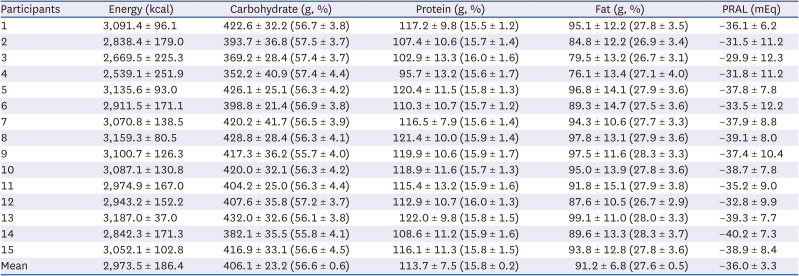
Table 2
Daily mean energy, macronutrient, and PRAL values of the foods consumed by each participant (n = 15)
![]()
Body composition and anthropometric measurements before and after diet
Table 3 lists the participants’ body composition and anthropometric measurements before and after diet. There was no statistically significant difference in waist circumference, hip circumference, and waist-to-hip ratio before and after the diet (P > 0.05) among the anthropometric measurements of the participants. Although the height increased at the end of the intervention (P = 0.00), the upper middle arm circumference decreased (P = 0.01). The body composition measurements were similar before and after the diet (P > 0.05).
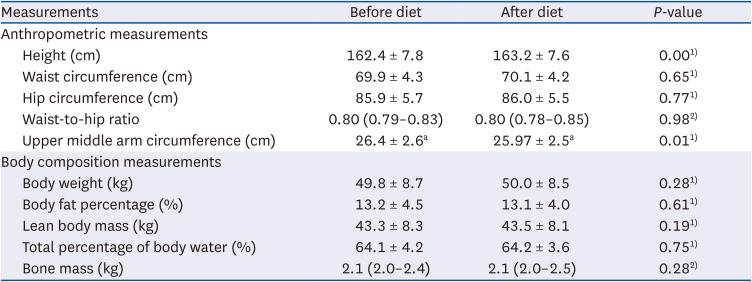
Table 3
Findings of body composition and anthropometric measurements of participants before and after diet (n = 15)
Data are presented as mean ± SD or median (25th–75th percentiles).
1)Analyzed by dependent sample t-test; 2)Analyzed by a Wilcoxon test.
![]()
Performance results before and after diet
Table 4 lists the performance measurements of participants before and after the diet. The average height of active and squat jumps increased significantly after the diet intervention (P < 0.05). Anaerobic power in the active jump was similar before and after the diet (P = 0.865). The median anaerobic power of the squat jump increased after diet (P = 0.011). The increase in mean grip strength for the right and left hand was statistically significant after the diet (P < 0.05). In the shuttle run test, the test duration was extended, and the total distance, number of shuttles, and maximal oxygen consumption increased following the diet (P < 0.05). The maximum heart rate was similar before and after the diet (P = 0.075).
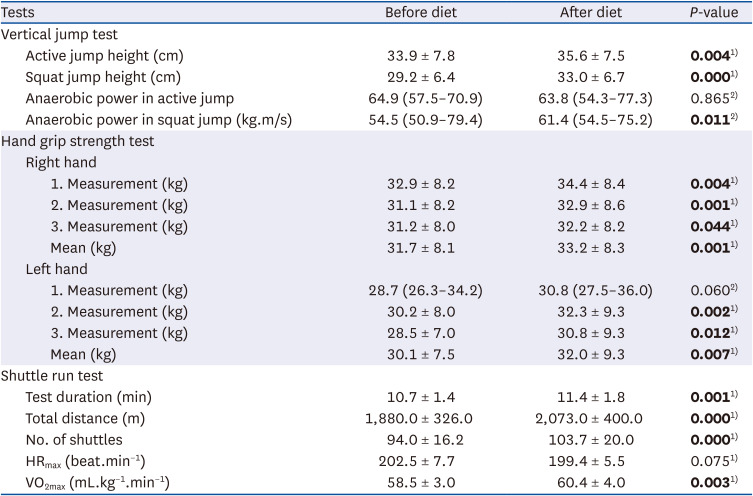
Table 4
Findings of the pre- and post-diet performance measurements of participants (n = 15)
Data are presented as mean ± SD or median (25th–75th percentiles). Bold P-values are less than 0.05.
HRmax, maximum heart rate; VO2max, maximum oxygen consumption.
1)Analyzed by dependent sample t-test; 2)Analyzed by Wilcoxon test.
![]()
Fig. 1 presents the perceived fatigue scores of the participants during the shuttle run test before and after the diet. There was a statistically significant decrease in the perceived fatigue scores (P < 0.05) in the 4th, 5th, 9th, 10th, and 11th stages. Furthermore, the number of athletes who proceeded to the 11th, 12th, 13th, and 14th stages increased after the diet.
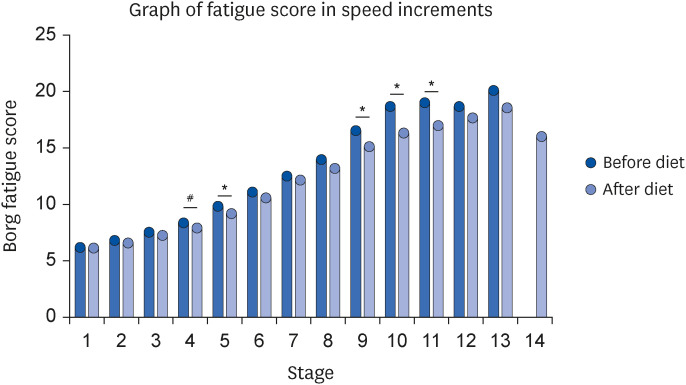 | Fig. 1Perceived fatigue scores during speed increment in the shuttle run test (n = 15). Mean values, n = 15 at the 1st, 2nd, 3rd, 4th, 5th, 6th, and 7th stages; n = 14 at the 8th and 9th stages; n = 13 at the 10th stage. Before the diet, n = 6 at the 11th stage, n = 3 at the 12th stage, and n = 1 at the 13th stage. After the diet, n = 9 at the 11th stage, n = 6 at the 12th stage, n = 4 at the 13th stage, and n = 1 at the 14th stage.
*P < 0.05: Wilcoxon analysis; #P < 0.05: dependent sample t-test.
|
Lactate levels before and after diet
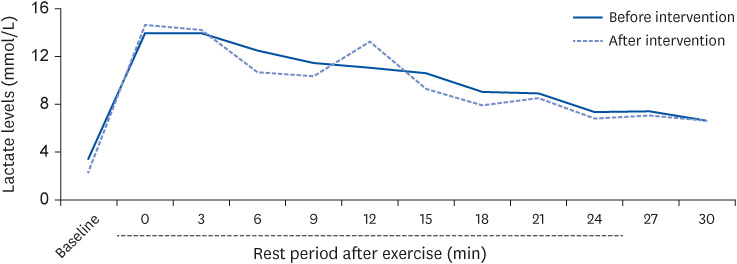
Fig. 2 shows the mean lactate levels of the participants before and after the shuttle run test. The lactate levels before and after the diet were similar in all periods examined (P > 0.05). Fig. 3 indicates the lactate half-life of the participants while at rest. The mean lactate half-life before and after the diet was 890.2 ± 374.7 and 917.9 ± 361.2 s, respectively, and remained unchanged (P = 0.838).

Go to :
DISCUSSION
The athletes were consuming a high-protein athlete’s diet prior to dietary intervention. The given menu was rich in fiber, complex carbohydrates, polyphenols, and micronutrients according to the usual diet of the athletes. The energy density, saturated fat content, and animal protein on the menu were low compared to their usual diets. The present study showed that the athletes consumed an average of 2,974 kcal/day of the Mediterranean diet (3,200 kcal/day) provided to them as much as they needed. Previous studies reported that the daily energy intake of the athletes in different countries was suboptimal. Professional adolescent male athletes may experience an energy deficit corresponding to approximately 800 kcal per day [3940]. The largest energy deficit generally occurs on the days of intensive training [41]. This study also found that the energy intake was less than recommended. On the other hand, the daily energy intake for adolescent male athletes in various sports was reported to be lower (e.g., 2,831 kcal, 2,640 kcal, 2,051 kcal) in this study [394042]. All approaches to measuring the dietary intake have their constraints [43]. In the present study, however, the experts recorded their food consumption by checking the plates of the athletes after each meal. Those records tended to reflect the truth. This might explain the greater daily energy intake than previous studies based on retrospective reminders and self-report. Positive feedback showed that the variety, satiety, and taste of the menu applied in this study were sufficient. The lower energy intake than the recommended level can be explained by the observation that the Mediterranean diet decreases food intake by enhancing satiety because of its high fiber content [44].
In this study, athletes received 56.6%, 15.8%, and 27.6% on average of their daily energy from carbohydrates, proteins, and fats, respectively; all were within the recommended range [28]. The average amount of protein the athletes consumed per body weight in this study was 2.34 g/kg. The minimal protein intake (1.4 g/kg/day) recommended for adolescent athletes to maintain a positive nitrogen balance was satisfied [45]. All micronutrient intakes were above the recommended levels in this study. These findings corroborate a study reporting that the Mediterranean diet scores of adolescents were positively correlated with the micronutrient adequacy [46]. The greater intake of micronutrients by athletes is due most likely to their higher energy requirements, use of dietary supplements, and attention to nutrition plans. In one study, following a Mediterranean diet was linked to a better nutritional profile, even when the micronutrient intake was adjusted to the total energy intake [47].
The average PRAL value for the foods consumed by the athletes was −36 mEq/day. Previous studies on the effects of low-acid dietary interventions on the exercise performance included lower (−21 mEq/day) and higher (−117 mEq/day) dietary PRAL levels [2448]. A study with a lower PRAL value found that the diet raised the fasting morning urine pH of the participants [24]. Consequently, the PRAL value of the foods consumed in this study appeared sufficient for increasing the systemic alkalinity.
The anthropometric characteristics and body composition are factors that determine the athletic success. These factors were also utilized to evaluate the athlete’s nutritional status or the effectiveness of a diet [49]. The average waist and hip circumferences of the athletes in this study were approximately 70 cm and 86 cm, respectively. The literature reported higher and relatively close values for adolescent male athletes [505152]. This study found that the waist and hip circumferences remained unaltered following the dietary intervention. Increased adherence to the Mediterranean diet was related to a decrease in the waist circumference of non-athlete adolescents. In contrast, the adherence to the Mediterranean diet was not associated with the waist and hip circumference of the adolescent athletes [5354]. According to one study, different diet patterns did not affect the waist circumference of athletes [55]. The dietary intervention did not impact the body fat or lean body mass. The average body fat ratio was approximately 13%, which is consistent with those ranging from 12.6 to 15.4% for adolescent male athletes [505256]. Studies on the different sports branches and age groups have demonstrated no relationship between adherence to the Mediterranean diet and the body fat ratio, muscle ratio, or any body composition [57585960]. Adherence to the Mediterranean diet, however, may influence the body composition in the non-athlete groups. Adolescent males with higher adherence to the Mediterranean diet had a lower body fat ratio [61]. Professional athletes maintain their body composition and anthropometric measurements within a specific reference range for their performance and are followed up regularly [6263]. Therefore, dietary intervention-derived alterations in anthropometric measurements and body composition can be more difficult to observe in the athletic group.
The present Mediterranean diet intervention decreased the upper mid-arm circumference of the athletes. While some studies found a negative relationship between the Mediterranean diet score and upper mid-arm circumference, others reported no correlation [646566]. The decrease in upper mid-arm circumference may be related to a decrease in muscle mass or subcutaneous adipose tissue [67]. The improvement in hand grip strength following the dietary intervention suggests that the change in arm circumference is a poor sign. The dietary intervention resulted in an increase in athletes’ height. The average change in height over the 15-day period was 0.8 cm. A 28-day Mediterranean diet resulted in an average height gain of 0.7 cm in adolescents [68]. The growth-stimulating components present in the Mediterranean diet may have contributed to the rapid short-term increase in height. Omega-3 fatty acids and calcium are dietary components linked to a faster increase in length by stimulating growth [6970]. Adolescents who stick to a healthy diet rich in vegetable protein and white meat had open growth plates and were taller [71]. The Mediterranean diet may have positive impacts on the bone mass and height of adolescent individuals by increasing the calcium bioavailability [68]. In this study, the bone mass did not change after dietary intervention. Similarly, Julián et al. [72] observed no link between the Mediterranean diet scores and the bone mineral content of adolescents. Another study found that, in addition to sufficient calcium intake, adequate vegetable and fruit intake improved the bone mineral contents in children and adolescents [73]. While a low-sodium Mediterranean diet lowers calcium excretion, it promotes bone remodeling through its high contents of zinc and vitamins A, C, and K [74]. A positive change in their bone mass may not have been observed in this study because the athletes continued their routine training schedules with dietary intervention. Strenuous training performed by professional athletes negatively impacts bone health and mineral density [75].
In this study, the 20-meter shuttle run test was used to determine the aerobic capacity of professional athletes, and the results were positive. Aerobic capacity is a critical success criterion in many sports branches (volleyball and football) [76]. Therefore, the results apply to some athletes where aerobic endurance is important. Some cross-sectional studies investigated the association between shuttle run performance and adherence to a Mediterranean diet. Manzano-Carrasco et al. [57] reported that the KIDMED scores of 1,198 prepubertal and pubertal athletes were positively connected with the duration of the shuttle run. The adherence of young athletes to the Mediterranean diet at a football academy was not connected with their shuttle run performance [54]. Similarly, the adherence of non-athlete adolescents to the Mediterranean diet had no connection with their shuttle run performance [77]. Previous studies with conflicting findings used the KIDMED questionnaire to determine adherence to the Mediterranean diet. This study adds to the weaknesses of cross-sectional studies that rely on participants’ self-report. The Mediterranean diet intervention enhanced shuttle run parameters. Furthermore, there was an improvement in running performance with no change in heart rate and a reduction in perceived fatigue scores. The treadmill performance improved without a change in heart rate in a study that adopted a short-term Mediterranean dietary intervention, which is consistent with these findings. While the run performance improved, the perceived fatigue level remained unchanged [22].
In young athletes, the Mediterranean diet boosted the hand grip strength and vertical jump height. A 4-day Mediterranean diet intervention did not affect the handgrip strength or vertical jump height of active individuals. Results contradicting this study are most likely due to the duration of dietary intervention [22]. A cross-sectional study showed that the Mediterranean diet score and hand grip strength were negatively correlated in female athletes but not in male athletes [58]. Another study reported that male child and adolescent athletes with high adherence to the Mediterranean diet had greater hand grip strength than those with low and moderate adherence. On the other hand, jump test results were not related to adherence to the Mediterranean diet [57].
The recovery process is a critical component of athletic performance. Full and quick recovery after exercise is essential, particularly in sports involving repetitive training and insufficient rest periods between training [78]. Lactate is one of the metabolic indicators used to objectively assess the adaptation and recovery processes of athletes [79]. Previous studies examined the effects of diet on lactate elimination both during and after exercise. An animal experiment reported that lactate elimination increased during resting following the treadmill test in the group given an antioxidant drink in addition to the standard diet for 6 wk compared to a control group [14]. Another study found that lactate elimination enhanced after exercise in subjects supplemented with the antioxidant astaxanthin for 4 wk [16]. More studies have been conducted on the effects of diet on lactate elimination during exercise. Magnesium, vitamins C and E, and thiamine were reported to reduce lactate accumulation during exercise [15808182]. Although this is the first study to examine the effects of the Mediterranean diet on lactate elimination after exercise in professional athletes, a surprising result was achieved. The Mediterranean diet may benefit lactate elimination because foods with a low acid load are favored in the used menu. Dietary intervention, however, did not affect the duration of lactate elimination. A normal protein diet rich in vegetables and fruits reduced the body acid load during exercise and rest compared to a high protein diet [83]. Furthermore, alkaline diets do not have as powerful an effect on the acid-base balance and blood buffering capacity as alkaline ergogenic aids but may enhance performance [84]. Improved performance and decreased perceived fatigue during performance were noted. The low-acid load Mediterranean diet may have effectively eliminated lactate and improved lactate tolerance during exercise but not after exercise.
This study presents the features of the sample group and research protocol, objective analysis, and significant outcomes. Because this study was conducted with a multidisciplinary team, it has significant strength in terms of menu planning, food intake follow-up, and performance measures in a precise and reliable manner. This study revealed some preliminary findings that will contribute significantly to the literature. Therefore, it is considered a critical initial step to developing evidence-based dietary approaches for athletes. The study does, however, have some limitations. The sample size was small (15 male athletes) because the research was conducted with a special group with the resources needed to carry out the research. Nevertheless, power analysis indicated that it represents the population. Adolescent athletes were included in the study based on their chronological age, without considering their developmental stages. The involvement of individuals at the same developmental stage can help achieve better standardization. Field-based performance measurements were favored instead of laboratory-based performance measurements. Therefore, maximum oxygen consumption was calculated using an equation based on the shuttle run test. Although this equation is commonly used and accepted, more precise results may be obtained using a gas analyzer in a laboratory setting. Only lactate measurements were taken to evaluate the recovery process. Furthermore, the dietary intervention might affect recovery if different recovery biomarkers were examined. Further in-depth studies considering these limitations will be needed to understand the different effects of the Mediterranean diet on athletic performance.
The results show that a low acid load Mediterranean diet may represent a safe and viable dietary approach for aerobic performance and strength enhancement. Only males were included because the elements of physiology unique to females, such as fluctuating female sex hormone concentrations throughout different phases of the menstrual cycle, will affect the results. The findings must be confirmed in a larger sample, different ages, genders, and sports branches. New research on the “Mediterranean diet and sport” will expand understanding of the effects of diet on athletes, with or without evidence supporting the diet. Future research may address aspects of the Mediterranean diet relevant to athlete health and performance. Thus, the holistic benefits of the Mediterranean diet for athletes will be understood.
Go to :
 XML Download
XML Download