

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer is one of the most common cancers worldwide, and its incidence and mortality rates continue to rise.1 This trend is closely associated with changes in dietary habits, a major risk factor for colorectal cancer. The increase in colorectal cancer incidence in countries previously considered low-risk and of low socioeconomic status is most likely the result of lifestyle and dietary changes.2 Therefore, understanding the influence of dietary factors on the onset of colorectal cancer plays a crucial role in preventing and treating colorectal cancer.
This review examines the complex interplay between dietary factors and colorectal cancer, focusing on the critical nutrients and dietary habits that influence the onset and progression of colorectal cancer. This paper discusses the impact of diet on the colorectal microbiota, the influence of diet on early-onset colorectal cancer, and reviews recent research on how dietary interventions affect the treatment and recurrence of colorectal cancer. Finally, future research directions for developing and applying effective dietary interventions are discussed.
Go to : 
RELATIONSHIP BETWEEN DIETARY NUTRIENTS AND COLORECTAL CANCER
1. Hypothesis and in vitro experiments
The incidence of colorectal cancer (CRC) is influenced by various host and environmental factors. These risk factors can be broadly divided into non-modifiable and modifiable.3 Nonmodifiable factors include age, family history of CRC, hereditary cancer syndromes, low-penetrance genetic variations and aberrations, and a history of inflammatory bowel disease. Modifiable factors, however, include diet, lifestyle, smoking, alcohol consumption, physical activity, and obesity. In 1981, Doll and Peto4 estimated that as many as 35% of cancer-related deaths and 90% of the stomach and colorectal cancer- related deaths could be linked to dietary factors. An analysis of the proportion of colorectal cancer cases associated with sporadic and hereditary factors showed that most CRCs occur sporadically through acquired somatic genomic alterations. In contrast, 35–40% of cases are associated with inherited CRC susceptibility.5 These sporadically arisen CRCs, accounting for 60–65% of cases, are influenced by environmental factors in their carcinogenesis. Consequently, numerous in vitro studies have investigated the relationships between dietary nutrients and colorectal cancer. Calcium, vitamin D, fiber, omega-3 polyunsaturated fatty acids (PUFAs), and sulfur are among the most representative of these well-investigated dietary nutrients (Fig. 1).6
Calcium has been studied extensively in relation to colorectal cancer, making it one of the most well-studied micronutrients. Despite being an essential nutrient for maintaining bone and dental health, increasing scientific evidence regarding its association with CRC exists. One hypothesis proposes that calcium has an anti-cancer effect by forming insoluble precipitates with tumor-promoting free fatty acids and bile acids, rendering them ineffective in the colonic mucosa. When analyzing colon carcinogenesis and genetic aberrancy through the supplementation of various nutrients in a mouse model, the significant effects were particularly evident when supplemented with vitamin D and calcium. Among the different nutrient supplements, only the combined supplementation of calcium and vitamin D resulted in a significant decrease in colon tumor occurrence and genetic variability over two years.7 Calcium can affect the risk of CRC through various additional mechanisms. These include their ability to suppress oxidative DNA damage8 and modulate cell signaling pathways9 associated with CRC. These effects are believed to be mediated by extracellular calcium-sensing receptor (CaR) signaling, which plays a role in maintaining the integrity of the intestinal barrier function and the balance between the gut microbes and the immune response.10
In 1980, Garland and Garland11 attributed the higher mortality rate of CRC in populations with limited exposure to solar UV-B radiation to the low vitamin D status. Subsequent research supported this hypothesis, showing a consistent inverse relationship between the vitamin D levels and the incidence of adenoma,12 CRC, and mortality.13 Vitamin D exerts its effects by binding to the nuclear vitamin D receptor (VDR) and activating it, which is associated with various anti-cancer activities, including CRC. The vitamin D-VDR complex plays a critical role in regulating the immune response against tumors in colorectal cancer. Studies have consistently shown an association between specific single-nucleotide polymorphisms, such as BsmI, ApaI, and TaqI, in the VDR gene and CRC.14 Therefore, numerous clinical cohort studies focusing on the impact of vitamin D have been conducted, which will be discussed in detail in the following section.
Burkitt15 proposed that a high-fiber diet could protect against CRC. This hypothesis was based on observational studies showing a low CRC incidence among Africans who consumed fiber-rich diets. Several mechanisms have been proposed to explain this hypothesis. First, a high-fiber intake could lead to reduced concentrations of intestinal carcinogens because of the increased stool mass, decreased adiposity, transit time, and the bacterial fermentation of resistant starch into short-chain fatty acids (SCFAs).15 Among these SCFAs, butyrate is a major product of colonic fermentation and serves as the preferred energy source for colonocytes.16 Butyrate promotes apoptosis and inhibits the proliferation of cancer cells in various in-vitro studies.17 SCFAs produced by high fiber intake have immune-modulatory and anti-inflammatory effects, leading to a healthy gastrointestinal environment.18
Fish oil consumption has protective effects against chronic degenerative diseases, including cardiovascular and autoimmune disorders, type-2 diabetes, rheumatoid arthritis, dementia, and cancer.19 These can be attributed to the high omega-3 PUFA contents in fish oil, such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). EPA and DHA play a role in producing resolvins and other lipid mediators with pro-resolving and anti-inflammatory effects.20 The impaired conversion of these fatty acids has been linked to various human diseases, including CRC. Experimental studies using IL-10−/− mice with induced colitis21 reported that the administration of DHA demonstrated ameliorating effects. This was observed through the reduced production of pro-inflammatory cytokines (TNF-α, IFN-γ), decreased infiltration of inflammatory cells, and improved histology scores of the proximal colon mucosa.
On the other hand, it is not just the absolute intake of PUFAs that matters, but also the balanced omega-3 to omega-6 ratio of PUFAs in the diet for normal growth and development. An Italian population22 study showed that higher levels of total omega-3 PUFAs (DHA, EPA, and α-linolenic acid) in the serum decreased the production of pro-inflammatory markers (IL-6, IL-1ra, and TNF-α) and increased the production of anti-inflammatory markers (e.g., soluble IL-6r, IL-10, and TGF-β). In contrast, lower omega-6 PUFAs levels have been linked to higher IL-1ra levels and lower TGF-β production.
Sulfur, a micronutrient that has recently gained attention, was hypothesized to influence the gut microbiome and affect the incidence of CRC.23 Diets high in sulfur microbes, such as red or processed meats and French fries, and low intake of fruits and leafy vegetables have been linked to an increased risk of both CRC and early-onset colorectal cancer.23 Sulfur-containing amino acids from proteins, such as methionine, cysteine, and taurine, are metabolized to hydrogen sulfide (H2S) by the gut bacteria through reduction and fermentation reactions.24 This process involves the metabolism of inorganic sulfur, such as sulfate and sulfite, commonly found in the preservatives used in processed foods. H2S can easily permeate the membranes of the colonocytes and epithelial cells because of its high permeability. The overproduced H2S also serves as an inorganic electron donor, stimulating mitochondrial electron transport in CRC cells.
This section explored the mechanisms through which nutrients have been most extensively researched and hypothesized to influence the incidence of CRC. Herein, the clinical evidence and controversies surrounding these nutrients were discussed.
2. Clinical studies and dietary interventions
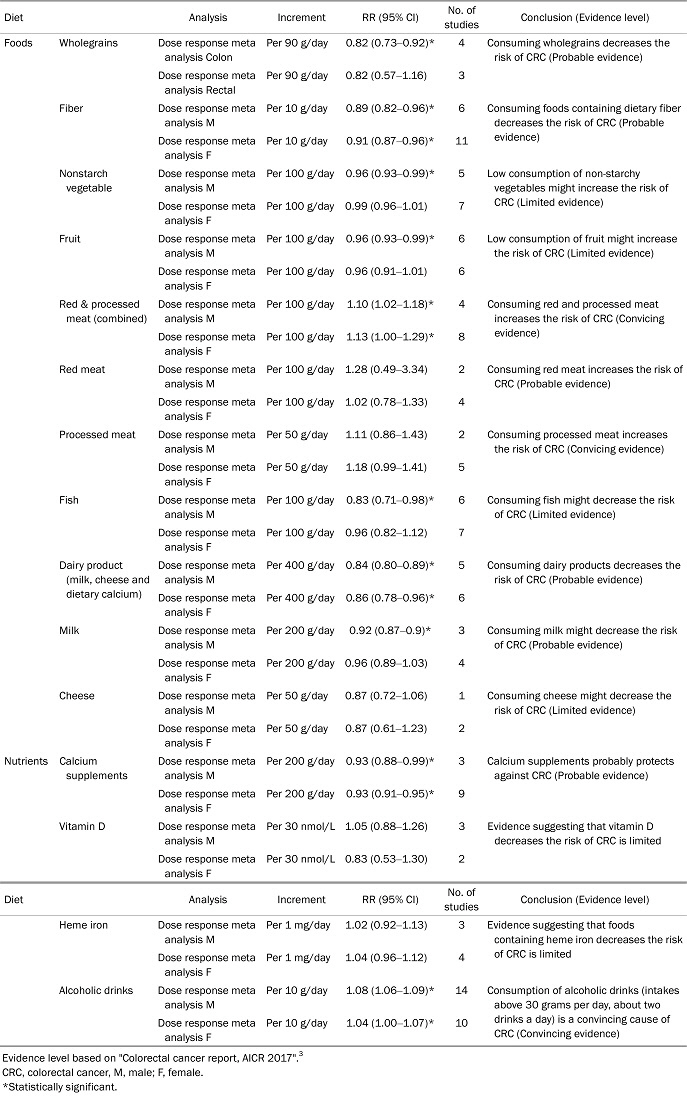
The World Cancer Research Fund and American Institute for Cancer Research (WCRF/AICR)3 provide the latest research on diet, nutrition, and physical activity related to cancer prevention and survival (Tables 1, 2). They classified the dietary and nutritional factors related to colorectal cancer into strong and limited evidence. Regarding micronutrients, there is strong evidence that fiber and calcium supplements probably decrease the risk of colorectal cancer. On the other hand, there is limited evidence with foods containing vitamin C, vitamin D, and multivitamin supplements, suggesting a decreased risk of colorectal cancer. Dietary omega-3 PUFAs, folate, vitamins A, B6, E, and beta-carotene have limited evidence with no conclusion. Therefore, fiber, calcium supplements, and vitamins C and D are nutrients that can be recommended for intake with substantial evidence.
Table 1
Effects of Dietary Interventions Related to the Prevention and Treatment of Colorectal Cancer
|
![]()
Table 2
Major Nutrients associated with CRC or Colon Polyps and Their Related Mecha
![]()
1) Calcium
The consumption of calcium-rich dairy products appears to protect against colorectal cancer. According to a dose-response, pooled meta-analysis3 of dietary calcium and CRC that analyzed 13 studies, the consumption of an additional 200 mg of calcium daily through foods, such as dairy products, milk, and cheese, showed a statistically significant effect (RR 0.93, 95% CI: 0.89–0.97) and demonstrated no or little heterogeneity among papers. On the other hand, the evidence for cheese consumption was weaker than that for exposure to other foods. On the other hand, for additional calcium supplements, a decreased risk of CRC of approximately 14–26% per 1,000 mg/day was reported, confirming that men benefitted more (RR 0.76, 95% CI: 0.65–0.89).
A double-blind, placebo-controlled clinical trial called The Women’s Health Initiative study25 was conducted. In that study, 36,282 postmenopausal women in the United States were given 1,000 mg of elemental calcium carbonate plus 400 IU of vitamin D3 daily, with an average follow-up period of seven years. No significant associations with CRC risk were observed for calcium and vitamin D supplementation compared to placebo use in all trial participants (RR 1.06, 95% CI: 0.85–1.32). This randomized clinical trial had the limitation of being conducted in a limited population, but there was sufficient evidence of plausible mechanisms through which calcium supplements probably protect against colorectal cancer in humans.
2) Vitamin D
The dietary consumption of vitamin D reduces the risk of CRC. Despite the limited evidence, the results are generally consistent. A dose-response meta-analysis3 of foods containing vitamin D showed a significant reduction in the risk of colorectal cancer, with a 5% risk reduction per 100 IU per day (RR 0.95, 95% CI: 0.93–0.98). Similarly, for vitamin D supplements, a 7% decrease in CRC risk was observed for every 100 IU/day (RR 0.93, 95% CI: 0.88–0.98). Furthermore, a study26 analyzing the relationship between the serum vitamin D levels and CRC found a significant inverse association when comparing the highest and lowest levels of serum 25-hydroxyvitamin D (RR 0.66, 95% CI: 0.54–0.81). Although it is premature to conclude whether dietary vitamin D intake or the serum vitamin D levels are more important, there is limited evidence suggesting that the vitamin D intake protects against colorectal cancer.
3) Fiber
Despite the significant experimental evidence, human studies on the relationship between fiber intake and CRC have produced inconsistent results. Fourteen cohort studies found no association between the fiber intake and CRC risk. In contrast, nine other cohorts detected an inverse association in at least some subgroups or certain fiber types.6 There are several potential reasons for these conflicting findings. The association between the fiber intake and CRC may be confounded by other behaviors closely linked to the fiber intake, and this confounding factor may vary across studies. Indeed, adjusting for other dietary and lifestyle factors, such as folate intake, red and processed meat consumption, and physical activity, weakened the inverse association between fiber and CRC in several cohort studies.27-29 While a recent meta-analysis reported a linear dose-response relationship, some studies suggested a threshold effect,29,30 with an increased risk of CRC among very low fiber consumers and no apparent benefit of fiber intake among those with high consumption. Most randomized clinical trials (RCTs)31,32 that tested fiber supplementation in patients with a history of colorectal polyps found no benefits. On the other hand, these RCTs were not entirely reliable because of poor patient compliance. Currently, the WCRF/AICR shows a 10% decreased risk of CRC per additional 10 g/day o total dietary fiber intake, and it is reasonable to recommend a high-fiber diet.
4) Omega-3 PUFAs
Omega-3 PUFAs have protective effects in clinical studies because of their potential anti-inflammatory effects in experimental models and excellent preventive effects against other cancers and age-related diseases. A placebo-controlled RCT33 showed that the administration of omega-3 PUFAs at 2 g/day for six months reduced the number, size, and overall burden of polyps in patients with familial adenomatous polyposis. A prospective cohort study was conducted on omega- 3 fatty acids and colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC),34 which followed an average of 14.9 years in prospective cohorts from 10 European countries and had 6,291 CRC incidents during this period. The intake of dietary fish and omega- 3 fatty acids from these fish, e.g., eicosapentaenoic acid (EPA), diphenylalanine (DPA), and DHA, was significantly lower in the case group. In addition, good results are expected from the largest ongoing RCT, the SeAFOod Polyp Prevention Trial.35 On the other hand, a double-blind, randomized, placebo-controlled trial36 and a cohort study37 with the Health Professionals Follow-up Study (HPFS) and Nurses' Health Study (NHS) showed that omega-3 PUFAs intake did not affect the overall CRC risk and CRC recurrence. Therefore, the anti-CRC efficacy of n-3 PUFAs remains inconclusive, making it difficult to establish dietary recommendations or guidelines on ω-3 PUFAs for CRC. One reason for these results is that the anti-inflammatory and cancer-preventive effects of omega-3 fatty acids occur in epoxy-fatty acids (EpFA). Nevertheless, the soluble epoxide hydrolase that metabolizes them has an inter-individual variance. In addition, the omega-6 to 3 ratio may be more critical than the omega-3 PUFAs intake. In particular, the excessive omega-6 PUFAs content and high omega-6 to omega- 3 ratio found in a westernized diet affected the anti-inflammatory functions of alpha-linolenic acid.38
5) Sulfur
Inorganic sulfate is used primarily to preserve processed foods and beverages, leading to a sulfur-rich diet. This also occurs through the consumption of sulfur-containing amino acids, such as methionine, cysteine, and taurine.39 Such a high-sulfur diet produces H2S, a metabolic byproduct associated with chronic inflammatory diseases, such as ulcerative colitis (UC), through reduction and fermentation reactions by the gut microbiota. Experimental evidence has linked this to CRC. Subsequent prospective clinical studies that addressed the role of H2S in inflammation or carcinogenesis in UC patients40 showed that chronic H2S exposure is associated with factors promoting carcinogenesis, such as impaired colonocyte nutrition, DNA damage, epithelial hyperproliferation, inflammation, and alterations in immune cell populations and function.41,42
A noteworthy point in sulfur-related research is that depending on the type and amount of sulfur-containing food consumed, a preventive effect, rather than a provocative one, may appear concerning CRC occurrence. When colorectal cancer cells are exposed to hydrogen sulfide donors that are slowly released at low concentrations (typically 0.2–0.3 micromoles), they activate H2S-generating enzymes, leading to increased glycolysis for mitochondrial function and energy production, enhancing cancer cell proliferation. The enzymes responsible for H2S generation have not been found in colonic epithelial cells.43 On the other hand, high H2S concentrations (typically approximately 1 mM) induce apoptosis (programmed cell death) in colorectal cancer cells. This suggests that, at high concentrations, H2S can have cytotoxic effects on cancer cells and inhibit their growth.44 Other dietary sources of sulfur, such as the allyl sulfur components from garlic and the sulfur- containing glycosinolates from cruciferous vegetables, such as cabbage and broccoli, have antineoplastic effects via multiple mechanisms, including inhibition of carcinogen-activating enzymes, detoxification of carcinogens, induction of apoptosis, arrest of cell-cycle progression, modulation of inflammation, and suppression of angiogenesis.45-47 Therefore, rather than analyzing all types of food as a sulfur-rich diet, it is essential to divide and analyze them separately depending on what kind of sulfur-containing food it is, and more research is needed on its role in CRC prevention.
3. Impact of diet on the colorectal microbiota
The human intestine is a habitat for billions of microorganisms, collectively known as the "microbiota," and their collective genetic material is called the "microbiome."48,49 The gut microbiota supports intestinal homeostasis and anti-tumor responses but can also contribute to carcinogenesis by causing chronic dysregulated inflammation.50 Significant shifts at the phylum level have been reported in the intestinal bacterial community of CRC patients. Among them, increased Bacteroides, Fusobacteria, and Proteobacteria, while decreased Firmicutes are found in the intestinal mucosa and feces of patients with CRC.51,52
The interaction between the gut microbiota and host diet plays a crucial role in disease development by regulating the human metabolic and immune functions. In particular, enterotoxic strains of B. fragilis, polyketide synthase (PKS) positive strains of Escherichia coli, and Fusobacterium nucleatum are the three most well-known strains involved in colorectal tumorigenesis.53,54 Dietary fiber can shape the structure of the human gut microbiota by promoting the growth of butyrate- producing bacteria over other bacteria. Children from rural Africa, where the diet is high in fiber, have a strikingly different composition of gut microbiota from those from urban Europe.55 Switching from a low-fat, plant-rich diet to a Western diet changes the composition, metabolic pathways, and gene expression of the gut microbiome.56 Furthermore, probiotics, prebiotics, and synbiotics play a significant role in future CRC prevention and treatment through cancer cell immunomodulation and chemopreventive effects.57 In particular, probiotic strains, such as B. infantis, LGG, L. acidophilus, and L. casei, have reported some positive research outcomes.
4. Diet and early-onset colorectal cancer (EO-CRC)
Despite the decreasing trend in colorectal cancer among the elderly population over the past few decades, the consistent increase in the incidence among adolescents and young adults contradicts this trend. EO-CRC is defined as colorectal cancer diagnosed before the age of 50, accounting for approximately 10–12% of newly diagnosed colorectal cancer.58 EO-CRC differs from late-onset CRC in terms of its epidemiology, anatomical localization, histopathology, and clinical pathology.58 EO-CRC cases are often discovered at clinically late stages, predominantly occurring in the left colon. Furthermore, EO-CRC exhibits higher proportions of specific histological characteristics, such as signet ring cell, mucinous histology, and poor differentiation.59 The cause of EO-CRC is genetic factors in approximately 20% of cases. The remaining 80% can be attributed to environmental factors without genetic mutations. Extensive research is being conducted on these environmental factors, which include the lack of routine screening, sedentary lifestyle, consumption of red and processed meat, and adoption of Western dietary patterns.60
The regular consumption of red meat, such as beef, veal, pork, and lamb, as well as processed meats that undergo salting, smoking, marination, air-drying, or heating processes, can lead to the formation of advanced glycation end products (AGEs). AGEs are formed through non-enzymatic glycation reactions during processing and cooking, particularly in low-fiber diets. They contribute to oxidative stress and chronic inflammation, leading to adverse health effects and an increased risk of chronic diseases. AGEs are increasingly associated with various chronic conditions, and their detrimental effects on health are becoming increasingly evident. Furthermore, AGEs can influence the microbial population in the gut, promoting the development of a microenvironment favorable for colorectal carcinogenesis.61,62
A prospective cohort study was conducted on 29,474 women who underwent colonoscopies before the age of 50. Their dietary patterns were investigated. The findings revealed significant associations between a Westernized diet and the occurrence of adenomas in the distal colon or rectum. In contrast, dietary approaches aimed at preventing hypertension (DASH), the Mediterranean diet, and adherence to healthy eating indices, such as the Healthy Eating Index (HEI) and Alternating Healthy Eating Index (AHEI), which assess the consistency of diets with the dietary guidelines for Americans and assign ratings to foods and nutrients predictive of chronic diseases, showed a reverse association with early-onset adenoma development.63-65
Therefore, consuming foods that can lower the risk of colorectal cancer, maintaining a healthy weight from a young age, and practicing dietary habits that prevent obesity and high blood pressure, such as DASH, the Mediterranean diet, HEI, and AHEI, can help reduce the incidence of EO-CRC.
5. Undiscovered areas and future directions in research
As discussed previously, various dietary factors have been identified as potential contributors to the CRC risk. In particular, the ingestion of alcohol and red and processed meats has been strongly associated with an increased risk of developing CRC. On the other hand, the consumption of white grains, fiber, dairy products, calcium, and vitamin D has been studied as factors that decrease the risk of CRC. On the other hand, the precise mechanistic underpinnings of these associations remain unclear and require further scientific investigation.
Another field that warrants further exploration is the identification of subpopulations for whom dietary interventions may be particularly efficacious. For example, the protective effects against colorectal adenomas and colorectal cancer conferred by increased calcium supplement intake (1,000 mg) vary significantly between males and females.3 Moreover, the location of colorectal cancer tumors can differ according to the excess or deficiency of specific nutrients,34 and the nutrients primarily involved in the onset of EO-CRC may differ from those involved in late-onset CRC.60 The effects of certain nutrients, such as dietary omega-3, may also vary depending on the presence or absence of specific enzymes, such as soluble epoxide hydrolase.66 Therefore, a long-term objective for public health improvement should be to identify colorectal cancer- associated subgroups through long-term cohort studies and conduct prospective interventional studies based on these findings.
Another promising research topic is the effect of dietary interventions on cancer survivors undergoing or having completed treatment for colorectal cancer. Some studies have been published on the effects of prebiotics and probiotics in these patient groups. In contrast, others suggest that improvements in treatment prognosis have been achieved with nutritional management before and after colorectal cancer surgery and during cancer treatment. On the other hand, few studies have examined this topic, necessitating multi-institutional studies involving a broad range of patients.
The most crucial tools in nutritional research are validated nutritional assessments, such as food frequency questionnaires. Traditional tools are labor-intensive and prone to bias, making the conduct of reliable studies challenging. With the advances in modern information technology and the development of image-perception artificial intelligence, a more thorough investigation of individual nutritional intake will become possible. Consequently, the reliability of nutrition-based epidemiological research is expected to increase. The results of various multicenter prospective studies on dietary nutrient intake and endoscopic outcomes should be published. The publication of such studies will increase the capacity to conduct comprehensive long-term interventional studies and provide more precise insights into the role of dietary factors in colorectal cancer risk. This enhances the capacity to conduct in-depth, long-term studies, providing more precise insights into the role of dietary factors in CRC risk.
Go to :
CONCLUSION
Understanding the influence of dietary factors on the onset of CRC is essential for its prevention and treatment. Future studies should cover the development and application of efficient nutritional assessment tools, the selection of appropriate subpopulations, the formulation of intervention strategies, and the execution of long-term interventional programs. The establishment of personalized dietary strategies will alleviate the global burden of CRC.
Go to :
 XML Download
XML Download