

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
It is recommended that infants and children should be exclusively breastfed for 6 months, and from 6 months thereafter, breastfeeding (BF) is encouraged while supplementary meals are provided.1 According to the American Academy of Pediatrics and the World Health Organization/United Nations Children’s Fund, the desirable total BF duration should be at least ≥ 12 and 24 months of age, respectively.12 According to many previous studies, exclusive breastfeeding (EBF) for 6 months has been reported to have many advantages for the health of both babies and mothers, including reducing the common respiratory and gastrointestinal infection rates, allergic disease in children, more postpartum weight loss, and longer periods of amenorrhea for mothers compared with those who did not receive EBF.34567 In addition, the longer the total BF period, the stronger the various advantages of BF, including higher intelligence and physical development, lower risk of obesity in children, and lower risk of breast cancer, ovarian cancer, and gestational diabetes to type 2 diabetes in mothers.891011 Therefore, the Korean Society of Pediatrics also adopted the international authorities’ recommendation of EBF for the first 6 months of life, particularly after launching the National Health Screening Program for Infants and Children (NHSPIC) in 2007 as part of the national health examination project in 20081213; however, it does not officially suggest the maximal desirable period of BF such as 12–24 months.
Meanwhile, the BF rate in Korea has been examined through the Korean National Health Examination and Nutrition Survey (KNHANES) by Korea Disease Control and Prevention Agency (KDCA) and the National Childbirth Ability and Family Health and Welfare Survey by the Korea Institute for Health and Social Affairs (KIHSA). A study with the nationwide data of KIHSA shows that the full BF at 6-month of age declined from 1994 until 2000 but was on the rise until 2012.14 However, there is no up-to-date study analyzing the current status of BF, particularly prolonged breastfeeding (PBF), for ≥ 12–24 months. Through the 4th National Health Promotion Plan 2020, the Ministry of Health and Welfare has enacted a policy to increase the BF rate for the first 6 months after birth from 60.8% in 2010 to 66.8% in 2020,15 and efforts have been made to increase the number of baby-friendly hospitals.16 A study analyzing mothers’ lifelong BF rates for > 1 month based on the KNHANES data17 reported an increase over the past 10 years; however, considering the BF rates released by KDCA, the 1-month and 6-month BF rates for infants do not appear to have increased.18 Therefore, further analysis is needed to understand the trend of recent BF rates in Korean children.
Until now, demographic, socioeconomic, educational, or health status-associated factors related to mothers and babies, which have been reported to be related to BF rates, have differed depending on the BF period, BF type, the participants, and the years investigated.192021222324 According to the 2018 KIHSA report, the mother’s educational level and residence area were significantly related to BF within an hour of birth.21 Based on the 4th data of the KNHANES (2007–2009), which is a study that analyzed the associated factors of full BF at the age of 6 months, was significant in the region, mother’s childbirth age, and delivery method, but employment status was not significant.24 A recent study on the factors related to a mother’s lifelong BF for ≥ 1 month based on data from the KNHANES (2010–2018) showed that the maternal health status and smoking history were also significant17; however, no data exist on the factors related to PBF for ≥ 12 months.
Therefore, we aimed to examine the status of PBF for ≥ 12 months in children aged 12–23 months for the past 10 years based on the data from the KNHANES (2010–2020) and analyze the characteristics of infants and their mothers to encourage PBF and provide a suitable education for nursing mothers.
METHODS
Study design and study population
This study was based on data from the KNHANES, which is a national surveillance system designed to assess the health and nutritional status of non-institutionalized civilians in Korea. This nationwide cross-sectional survey has been conducted every year since 2007 by the KDCA, which is composed of 3 component surveys as follows: health interviews, health examinations, and nutrition surveys. Using a stratified and multi-stage clustered probability sampling design, the representative households were selected according to the 3-year rolling sampling cycle, where individuals aged ≥ 1 year were targeted for the survey. The health interviews and examinations were performed by a trained survey team using face-to-face interview methods at a mobile examination center. The nutrition surveys conducted by dieticians’ visits to the home consisted of information on dietary behavior, food security, and food/nutrient intake. The detailed description of the KNHANES design and data profile has been published as a separate paper.25
We obtained data on participants aged 12–23 months from the 5th wave of the KNHANES (2010–2012) to a part of the 8th wave (2019–2020). The participants whose response to the nutrition surveys for feeding practice was missed were excluded from the study population. To determine BF-associated maternal factors, data from the infants were matched to their mother’s information, including socio-demographic status, health-related behaviors, and medical conditions; the mother’s condition was analyzed according to BF practice patterns.
Measurements
Breastfeeding practice
To define the BF practice patterns, the responses to the dietary behavior questionnaire designed for infants and young children aged 12–48 months in the nutrition survey were extracted and included feeding types (BF or formula feeding), starting age (weeks), and duration (months) of each feeding modules. With the data, the feeding types at 1, 3, 6, 9, 12, 15, 18, and 23 months of age were determined. When the infants were reported as being breastfed regardless of simultaneously having formula feeding, they were defined as having “any BF.” However, those who were reported to be breastfed without formula feeding during each month of age were defined as “full BF.” In addition, the infants who were fully breastfed at 1,3 and 6 months of age were defined as “EBF for 6 months.” The BF rate of each BF practice of the study population was calculated by grouping according to the study surveys as follows: KNHANES V (2010–2012), KNHANES VI (2013–2015), KNHANES VII (2016–2018), and part of KNHANES VIII (2019–2020).
Measurement for infant and maternal conditions
From the health interviews and nutrition surveys, the response to the self-reported questionnaires were extracted to evaluate the maternal and infant condition that could be associated with BF practice. Detailed information on socio-demographic characteristics, such as marital status, residential areas, family size, household income, current economic activity status (employment status), and maternal education level, was obtained. The residency area was categorized into urban and rural areas; household income was classified by quartiles and divided into 3 groups of the household equalized income as low (< 25 percentile), middle (25–75 percentile), and high (≥ 75 percentile). The maternal educational level was classified into 2 categories as high school graduates or under (≤ 12 years) and college and university graduates or over (> 12 years). Maternal nutritional knowledge was assessed with the questions from the nutrition surveys, “Have you ever received nutritional education or counseling conducted at public health centers, district offices, community centers, welfare facilities, schools, and hospitals, among others, during the past year?” “Do you understand and read the food label when buying or choosing processed foods?” “Does the food label affect your food choices?” indicating the variables of “received nutritional education,” “use of nutrition label,” and “nutrition label impact,” respectively.
Information regarding health-related behavior and medical condition of infants and mothers was also obtained from the response to self-reported questionnaires. As variables of maternal health-related behaviors, information of maternal current smoking and alcohol consumption status in the past 1 year was collected. To evaluate the maternal health condition, information of maternal postpartum health was obtained; maternal age at the first delivery, maternal age at the current child delivery that was calculated with the infant’s age subtracted from the maternal current age, the infant’s birth weight, multiple births, and the total number of nursed children. Maternal current health condition was assessed using the question “What do you think of your health in general?” where the choices for response were “very good, good, fair, bad, and very bad.” For analysis, responses were categorized into 3 groups as follows: “very good,” “good,” “fair,” “bad,” and “very bad.” In addition, maternal mental health was assessed using the question, “How much stress do you feel in your daily life?” We defined mothers who responded “very much” or “much” as the stress group compared with those who answered “mild” or “none.” Finally, information on the infant's health status was collected on whether the infant had ever been diagnosed with atopic dermatitis.
Statistical analyses
The sample weights were constructed to represent the Korean population by considering the complex survey design, non-response rate, and post-stratification and were applied to any analyses. Complex sample Rao–Scott χ2 test and generalized linear were used to evaluate the differences in categorical and continuous variables, respectively, according to BF practice. To analyze the associations between BF practice and infant or maternal conditions, complex sample multiple logistic regression analyses were used to estimate the adjusted odds ratio (aOR) and 95% confidence intervals (CIs) of the participants’ variables associated with BF after adjusting for possible confounders. Data are presented as weighted percentages and standard errors (SEs) and as weighted mean ± SE for categorical and continuous variables, respectively. All analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at P < 0.05.
Ethics statement
The survey procedures and protocols were approved by the Institutional Review Board (IRB) of the KDCA (IRB No. 2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2C, 2013-07CON-03-4C, 2013-12EXP-03-5C, 2018-01-03-P-A, 2018-01-03-C-A, 2018-01-03-2C-A) and written informed consent was obtained from all participants and/or their guardians for the survey. This study was conducted in accordance with the Declaration of Helsinki and approved by the IRB of Kangwon National University Hospital (IRB No. KNUH-2021-06-006).
RESULTS
Trends of breastfeeding practice from 2010 to 2020
Overall, 933 infants aged 12–23 months were included in this study. The number of participants in this study population recruited from each wave of the surveys is presented in Supplementary Table 1. The rate of full BF at 6 months of age was 34.8% (1.9), and by survey year, it was 42.8% (3.3) in 2010–2012, 41.5% (3.71) in 2013–2015, 28.0% (3.56) in 2016–2018 and 13.1% (3.9) in 2019–2020, showing a statistically significant decreasing trend (P < 0.001). In addition, 26.9% (1.7) of the study population was fully breastfed without formula feeding at 12 months of age, and their rate of full BF also significantly decreased from 2010 to 2020 (P < 0.001).
Over the past 10 years, any BF rates at the age of 1 month and 3 months were 88.3% (1.3) and 72.0% (1.80), respectively. These BF rates were not statistically different between the period of surveys. However, the 10-year any BF rate at 6 months of age was 55.4% (2.0), and by survey year, it was 65.9% (3.2) in 2010–2012, 59.1% (3.59) in 2013–2015, 48.8% (3.90) in 2016–2018 and 33.6% (5.3) in 2019–2020, showing a statistically significant decreasing trend (P < 0.001). At 12 months of age, 33.7% (1.9) of the study population was breastfed; subsequently, 7.1% (1.3) were reported to continue BF until 18 months of age. No one continued BF at the time of 23 months of age among the study population. The rate of infants with any BF at 12, 15, and 18 months of age consistently decreased from 2010 to 2020 with statistical significance (P < 0.001, P < 0.001, and P = 0.030, respectively).
The trend in BF practice rates by infant age and survey year is shown in Fig. 1.
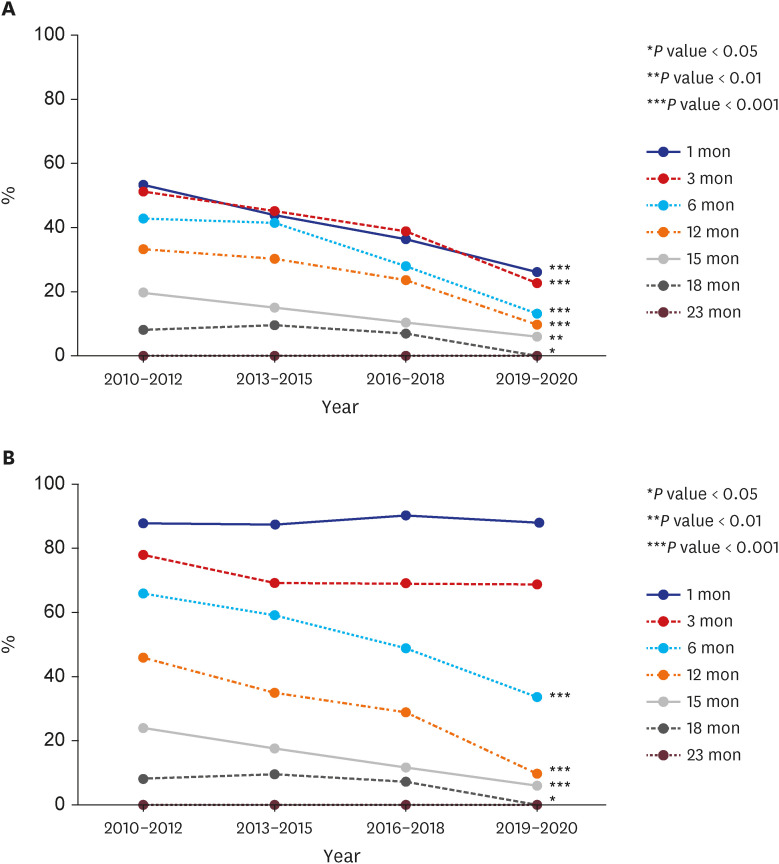
Fig. 1
Breastfeeding practice trends by survey year (2010–2020).
(A) Full breastfeeding rates show a statistically significant decline over the past decade in all age groups except 23 months of age. (B) Any breastfeeding rates for infants aged 6–18 months show a statistically significant decline over the past decade.
![]()
Infant and maternal conditions according to breastfeeding practice
Of the 933 infants, 849 whose maternal data were available were included in the final analysis. The maternal and infant characteristics were analyzed according to the 3 BF practice patterns as follows: EBF for 6 months of age, any BF for ≥ 12 months of age, and any BF for ≥ 18 months of age. The BF practice rates for the 3 types of BF analyzed in the 849 infants were similar to the rates for the 933 infants overall, as shown in Table 1.
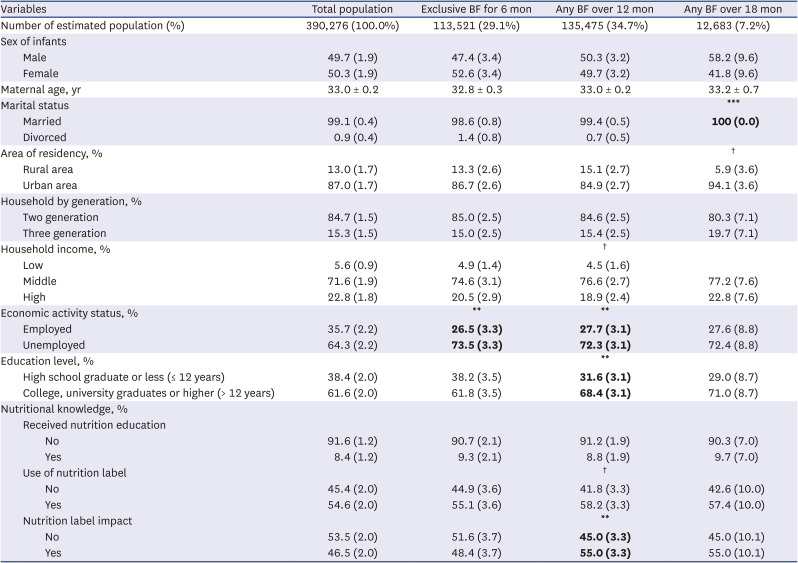
Table 1
Socio-demographic characteristics of infants and mothers according to BF practice pattern (N = 849)
All continuous variables are expressed as weighted means ± standard errors. All categorical variables are expressed as weighted percentages (standard errors). Bold font indicates statistical significance, and the P value was calculated in comparison with the other categorized subjects.
BF = breastfeeding.
*P < 0.05, **P < 0.01, ***P < 0.001, †P < 0.2.
![]()
Among the sociodemographic characteristics, infant sex, maternal age, area of residency, family size, and household income were not significantly associated with the BF practice. However, maternal economic activity was associated with both EBF for 6 months and continued BF for ≥ 12 months of age. Specifically, the mothers who were currently unemployed were more likely to have EBF for 6 months (P = 0.004) and PBF for ≥ 12 months of infants’ age (P = 0.003). The maternal educational level was also significantly associated with PBF for ≥ 12 months; that is, highly educated mothers were more likely to continue BF for ≥ 12 months of age (P = 0.008). However, this was not associated with EBF practice (P = 0.947) or PBF for ≥ 18 months of age (P = 0.349). Particularly, maternal nutritional knowledge was also associated with PBF for ≥ 12 months, indicating that mothers who were more likely to be affected by the food labels showed more continued BF for ≥ 12 months (P = 0.002). The sociodemographic characteristics of intents and their mothers according to the 3 BF practice patterns are presented in Table 1.
The maternal postpartum conditions were analyzed according to the BF practice and then presented in Table 2. EBF for 6 months was significantly associated with both PBF for ≥ 12 and 18 months (P < 0.001). Although maternal age at the first delivery was not significantly associated with BF practice, maternal age at current child delivery was associated with PBF for ≥ 18 months (P < 0.001). This implies that the mothers who were aged < 40 years during the participant’s birth were more likely to continue BF for 18 months of age than those aged ≥ 40 years. Additionally, low birth weight < 2.5 kg of the mother-delivered child and multiple births were negatively associated with EBF practice (P = 0.004 and P = 0.014, respectively); however, no association with PBF was found. The number of previously breastfed children indicating past BF experience also showed only an association with EBF for 6 months (P = 0.002) rather than with PBF.
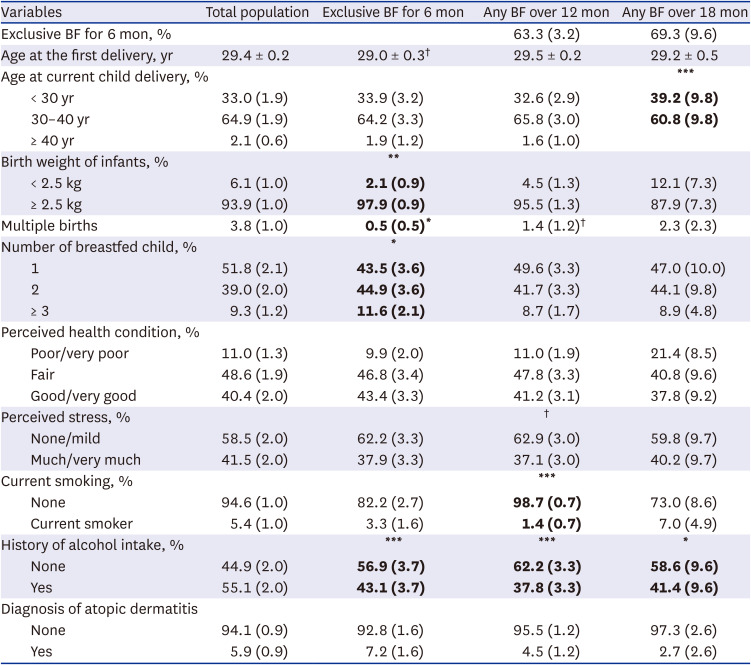
Table 2
Postpartum and current health conditions of infants and mothers (n = 849)
All continuous variables are expressed as weighted means ± standard errors. All categorical variables are expressed as weighted percentages (standard errors). Bold font indicates statistical significance and the P value was calculated in comparison with the other categorized subjects.
BF = breastfeeding.
*P < 0.05, **P < 0.01, ***P < 0.001, †P < 0.2.
![]()
Moreover, the maternal current general or mental health was not associated with the BF practice. However, mothers’ health-related behavior regarding smoking and alcohol consumption was associated with the BF practice. The mothers who were not current smokers were more likely to continue BF for ≥ 12 months than those who were current smokers (P = 0.001). Mothers without a history of recent alcohol intake were more likely to continue EBF for 6 months and PBF for ≥ 12 and ≥ 18 months than those with a history of recent alcohol intake (P < 0.001, P < 0.001, and P = 0.036, respectively). The infants with a history of atopic dermatitis diagnosis were not associated with the BF practice. The current health conditions of infants and their mothers according to the BF practice are presented in Table 2.
Maternal and infant conditions associated with the 3 breastfeeding practices
To determine other maternal conditions associated with each BF practice, logistic regression analysis was performed after adjusting for confounders, and the results are presented in Table 3. EBF for 6 months was most strongly associated with both types of PBF (crude odds ratio [cOR], 14.137; 95% CI, 9.412–21.236 for PBF of ≥ 12 months; P < 0.001 and cOR, 5.956; 95% CI, 2.341–15.152 for PBF of ≥ 18 months; P < 0.001). Among the maternal conditions, the currently unemployed status showed high odds of EBF for 6 months compared with the employed condition (aOR, 1.841; 95% CI, 1.204–2.815; P = 0.005). In addition, the birth weight status of the mother-delivered child was associated with EBF because the delivered infants with a weight of ≥ 2.5 kg were more likely to be breastfed exclusively for 6 months compared with those with a weight of < 2.5 kg (aOR, 3.716; 95% CI, 1.340–10.309; P = 0.012). Particularly, the mothers with BF experience were more likely to perform EBF for 6 months than those without. Notably, mothers who had previously breastfed more babies had a higher likelihood of EBF for 6 months than those who breastfed only 1 baby.
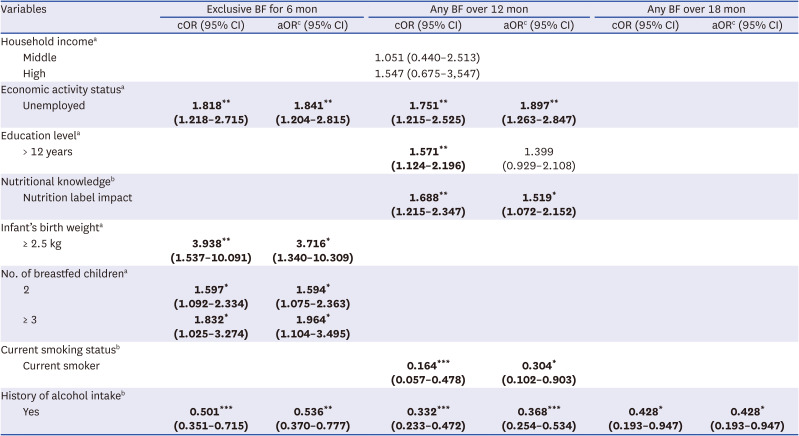
Table 3
Infant and maternal conditions associated with the BF practice pattern
Values are presented as cOR or aOR (95% CI). Bold means statistically significant.
BF = breastfeeding, cOR = crude odds ratio, aOR = adjusted odds ratio, CI = confidence interval.
aReference was low income, employed status, ≤ 12 years, < 2.5 kg, 1 child, respectively; bReference was none; cAdjusted for variables with P value < 0.2 from Tables 1 and 2.
*P < 0.05, **P < 0.01, ***P < 0.001.
![]()
Among the maternal conditions associated with PBF for ≥ 12 months, maternal nutritional knowledge status showed higher odds of continued BF for ≥ 12 months, indicating that mothers who depends on the nutrition labels when choosing foods were more likely to continue BF for ≥ 12 months than those who do not depend on the nutrition labels (aOR, 1.519; 95% CI, 1.072–2.152; P = 0.019). Moreover, mothers who did not currently smoke were more likely to continue BF for ≥ 12 months than those who currently smoked (aOR, 2.822; 95% CI, 1.262–6.310; P = 0.032). Maternal history of recent alcohol consumption status was negatively associated with BF, regardless of BF pattern or duration.
DISCUSSION
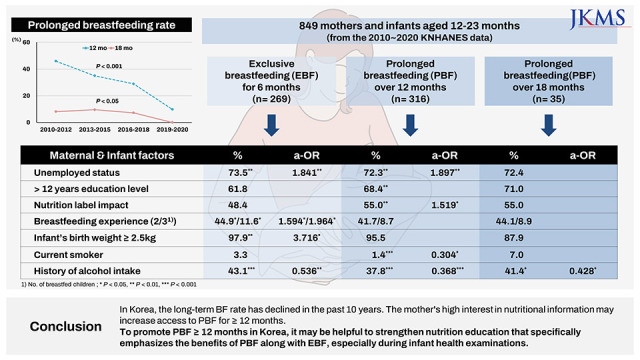
This study provides valuable data on the trends of long-term BF in Korea over the past 10 years as well as the factors that influence PBF of both infants and their mothers. The PBF rate for ≥ 12 months has declined in the past 10 years in Korea, and BF is rare after 18 months. The underweight infants at birth and the mother's inexperience with BF negatively affect EBF for 6 months rather than PBF for ≥ 12 months. The mother's high interest and knowledge in nutrition and diet increase access to PBF for ≥ 12 months but may not lead to continued BF for ≥ 18 months. To our knowledge, this is the first analysis to examine the recent rates of PBF for ≥ 12-18 months and to investigate the infant and maternal factors associated with successful PBF in Korea. It is also the first study to identify that being influenced by nutrition labeling may be one of the significant maternal factors associated with PBF for ≥ 12 months.
Over the past decade, the average PBF rate for Korean children ≥12 months of age was 33.7%, a decrease from the KNHANES IV (2007–2009) release, which reported a rate of 47.5%.18 A similar trend was found in the 6-month full BF rate, which decreased from 49.3% in 2007–2009 to 34.8% in 2010–2020.18 According to a study based on another nationwide survey by KIHSA, the full BF rate at 6 months of age peaked in 2009 (51.0%) and then decreased in 2012 (44.5%).14 After that, it gradually decreased in the 2015 (42.9%) and 2018 (23.6%) reports,1920 showing consistency with our results based on KNHANES data. The recent decline in the 12-month any BF rate observed in our results (45.9%, 35.0%, and 28.9% in 2010–2012, 2013–2015, and 2016–2018, respectively) was also observed in the publication by KIHSA, where BF rate at 12 months was 31.3% and 32.2% in 2012 and 2015, respectively,1920 and 23.3% in 2018.21 In the United States, the 12-month BF rate in 2014–2019 was approximately 35%, and the 6-month any BF rate was 55.3–58.3%,26 which was not significantly different from our results of the 33.7% and 55.4%, respectively.
Considering the BF rate by infants’ age, any BF rates at 1 and 3 months did not show a significant change by the survey period; however, the full BF rate showed a significant decrease in the recent survey, particularly from the 2016 data, at all ages, indicating an increasing trend toward choosing mixed BF before 6 months of age. This increase in early mixed feeding appears to eventually lead to a decrease in the PBF rate. In fact, among the factors positively affecting PBF for ≥ 12 months in this study, whether or not to exclusively breastfeed for 6 months had the largest odds ratio (cOR, 14.1; P < 0.001). Additionally, a recent Korean study of healthcare workers found that those who planned for 6 months of EBF actually breastfed longer than those who planned for mixed feedings from the start.27 Therefore, to increase the EBF and PBF rates, it is necessary to analyze the causes to choose early mixed feeding and establish countermeasures while simultaneously reviewing current policies and determining improvement points. Emphasizing BF through newborn-age screening, which has been added to the NHSPIC since 2021,13 could be used as a countermeasure to the increase in early mixed feeding, and further evaluation of this expectation is needed.
Although EBF for 6 months was the most influential factor leading to PBF for ≥ 12 months, approximately 23% of those who were exclusively breastfed for 6 months discontinued BF before 12 months. Similarly, approximately 37% of infants with PBF for ≥ 12 months were not exclusively breastfed for 6 months. Therefore, it can be predicted that there will be similarities and differences in the factors affecting EBF for 6 months and PBF for ≥ 12 months. Here, the mother’s employment and drinking status were analyzed as common factors for EBF for 6 months and PBF for ≥ 12 months. The association of employment status with full BF at 6 months was significant in the 2012 report by KIHSA but not in the 2015 and 2018 reports.192021 International studies generally report that the duration of BF in early infancy is significantly associated with maternal employment status.282930 Our study showed that PBF was also positively associated with maternal unemployed status. Since parental leave in Korea cannot exceed 1 year, there is a tendency to abstain from BF before returning to work, which appears to be a deterrent to PBF in some mothers with EBF for 6 months. However, compared to EBF, PBF is more sustainable after work if it is motivating and supported at work and at home.3132 There are reports that BF continuation after returning to work is influenced by occupation type and working conditions273133; however, in this study, the association between occupation type and EBF or PBF was not significant and was excluded from the final analysis. In the future, more well-designed national-level data on this topic may be needed for future policy formulation to promote BF.
Previous BF experience was significantly associated with EBF for 6 months; however, no correlation was found for PBF of ≥ 12 months. Recently, the fertility rate has been declining, and there are more cases where only one child is born and raised. In these cases, the EBF rate may decrease, but PBF may not be additionally affected. In contrast, maternal educational level was related to PBF for ≥ 12 months, but no association was found with EBF for 6 months in univariate analysis. Therefore, the issue of EBF for 6 months is believed to be more influenced by other factors, such as previous BF experience, than maternal educational level, and the question of whether to continue BF for ≥ 12 months is considered to be more influenced by the educational level. In previous Korean studies, the association of educational level and 6 months of full BF shows inconsistent results.192024 However, the overall association between BF initiation and cessation in infancy and maternal educational level were most significant in previous Korean and international studies.17192933 Smoking, which was analyzed as a factor related to PBF for ≥ 12 months, is already well-known to be closely related to educational attainment.2434
Particularly, maternal nutritional knowledge itself was an important factor associated with PBF over 12 months regardless of employment status or BF experience. The association of the mother’s affection using a nutrition label with PBF was significant, with an odds ratio of 1.5 after adjustment. Interestingly, only the influence of the nutrition label was significant rather than the experience of nutritional education or the use of nutrition label. Therefore, to promote PBF, a level of detailed education and recommendation that can enable strong motivation of nursing mothers may be required. In particular, from the time of the infant’s first health checkup during maternal postpartum period, nutritional education on the benefits of PBF should be provided to nursing mothers. In a previous survey of 414 mothers, a higher knowledge score on the benefits of BF for babies was associated with a longer intention to fully breastfeed, a longer duration of BF, and a higher intention to use a baby-friendly hospital.16 In the 2016 KIHSA report, the most common reason for ceasing BF in nursing mothers was that BF duration was considered sufficient.22
However, in contrast to the demand for such specific education, a recent survey of pediatricians’ perceptions of BF in Korea revealed that there is currently limited BF counseling for parents, suggesting the need for an appropriate BF counseling program for physicians.35 However, several developed countries has already developed and implemented the well-designed health supervision guidelines for primary healthcare practitioners of infants and toddlers.363738 In Canada, BF is one of the most important guidance items of education and advice, which emphasized PBF until the visit of 2–3 years of age.3637 In United States, the recommendations for a schedule of screening and assessment for children were presented by American Academy of Pediatrics that provide healthcare providers evidence-based practical guidance and supports to help mothers successfully initiate and maintain BF.38 Therefore, more detailed and proactive recommendations on BF guidelines for each screening cycle of the NHSPIC may be needed in Korea. Currently, the NHSPIC has seven waves, and nutrition education on BF is offered at the newborn age, which was added in 2021, and at 4-month age.1213 However, to encourage PBF, it may be necessary to include education at 9 and 18 months of age that identifies and encourages BF and emphasizes the benefits of PBF.
Infant factors investigated in this study were significant influencing factors for EBF for 6 months but had no significant effect on PBF. It is well-known that low birth weight infants, including preterm infants or multiple fetuses, are less prone to exclusive BF.394041 Even some mothers of full-term infants with low birth weight due to intrauterine growth retardation may prefer mixed feeding because of concerns about low birth weight and lower weight gain.41 Therefore, it can be observed that more intensive education and intervention are needed for mothers of low birth weight or multiple births. Although BF is generally recognized as protective against allergic diseases, including atopic dermatitis,517 the association was not significant for either EBF for 6 months or PBF in this study. This might be due in part to the fact that only atopic dermatitis that occurred in the first 2 years of life was included, but a study using KNHANES data for the first 4 years of life, conducted from 2007 to 2012, found similar results to this analysis.42 Although the preventive effect of BF on atopic dermatitis has been questioned recently,43 it seems likely that PBF, as well as EBF, should be strongly recommended for infants at risk of atopy until a definitive conclusion is reached.
For BF for ≥ 18 months, it was significant that the mother was aged < 40 years, did not take alcohol, and had stable marital status. The influence of nutritional labeling or level of maternal education did not show an additional effect on ≥ 18 months of BF compared with < 18 months. However, because the number is small, the interpretation of the results could be limited. Although the World Health Organization recommends BF for ≥ 24 months of age, no breastfed infants were found in this study population at 23 months of age. When all children under 48 months of age were included, although not presented in this study’s results, the 24-month BF rate for the past 10 years was approximately 4.7% based on the KNHANES data. Therefore, realistically, it is believed that more emphasis should be placed on recommending BF for ≥ 12 months rather than for 24 months. The analysis of factors related to BF for ≥ 18 months or 24 months should contain whole data of infants under 48 months of age included in the KNHANES. However, in this case, the disadvantages of the retrospective cross-sectional study can be reflected more in the results; therefore, a large-scale cohort study is required in the future to clarify the factors associated with PBF for ≥ 18–24 months.
This study had some limitations. First, since the KNHANES uses a retrospective survey, there may be a recall bias. Second, since the present study was a retrospective cross-sectional study rather than a cohort study, some of the factors affecting BF, such as household income, mother’s occupation, or mother’s health status, may differ between the time of BF cessation and that of the survey, although we only included the data from the children aged < 24 months. Lastly, not all maternal, infant, and socio-medical factors suggested to influence BF, such as delivery method, father’s support for BF, or access and use of baby-friendly hospital, were included in the analysis. Nevertheless, this is the only study known to the authors that investigated the recent status of PBF and factors affecting it using the KNHANES data, which is representative of Korean children. In addition, it is believed that it has important significance since it was confirmed that the behavior of actively reflecting the knowledge of nutrition into the diet was closely related to the choice of PBF for ≥ 1 year.
In conclusion, this study highlights the declining trend in the prevalence of PBF in Korea and the associated factors with PBF were identified. In-depth and specific nutrition education that provides nursing mothers with information on the exact health and nutritional benefits of breast milk compared to formula or cow’s milk is thought to be an effective motivator to continue BF into the second year of life.
 XML Download
XML Download