

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The incidence of dementia, a group of degenerative brain diseases, including Alzheimer’s dementia (AD), has been increasing worldwide.12 This not only affects the quality of life of patients and their families but also burdens national healthcare systems.3 Korea is one of the fastest-aging countries in the world and is no exception to the rise of dementia.45 According to a previous study in Korea, as of 2015, dementia’s crude incidence per 100,000 people aged ≥ 60 was 2,218.25, and the prevalence of dementia was reported to be near 10% in the population of ≥ 60 years old.5 Furthermore, it is estimated that by 2050, close to 2 million patients in Korea will be diagnosed with dementia.6 The sharp increase in patients with dementia leads to socioeconomic burdens and impacts the family structure’s capacity for caregiving.7 Hence, there is a significant risk that the socioeconomic burden of dementia may exceed the country’s bearable threshold.8 Therefore, national-level efforts are continuously required for the early diagnosis and timely intervention of dementia.910 Nevertheless, early detection and treatment of patients with dementia in local communities remain challenging.11
In response to these demands in Korea, the National Responsibility Policy for Dementia Care was introduced in 2017, and one of its main projects was the regional dementia centers (RDCs) with 256 operational centers as of 2022.1213 The RDCs are based in public health centers of each region and provide screening and management of patients with dementia comprehensively.14 Through this, efforts are being made to improve the management efficiency of patients with dementia and to address the gap in accessibility to medical institutions due to regional/income disparities.1215 Although a large amount of public funds and human resources have been continuously invested in the centers,12 since the policy was implemented, there has been a scarcity of related studies identifying the role and function of RDCs. In particular, no study has differentiated the roles of RDCs from that of regional general hospitals, or the prognosis of patients with dementia diagnosed in RDCs from those diagnosed in regional general hospitals.
In this context, this study aimed to investigate patients with AD who were diagnosed at RDCs in a region of Korea. We demonstrated the differences in the clinical characteristics and disease progression between two groups of patients, namely those initially diagnosed through an RDC and those diagnosed through a regional general hospital. Through this, we aimed to ascertain that the RDCs have contributed to ensuring that patients with AD, who may not have access to existing medical systems, receive the appropriate treatment.
METHODS
Study design and participants
This single-center retrospective cohort study initially included 2,130 patients diagnosed with AD between January 2019 and March 2022. AD was identified based on the following primary diagnosis codes defined by the International Classification of Diseases, 10th Revision: F000, F001, F002, F009, and G309. Patients previously diagnosed with any dementia (n = 921) were excluded, and the remaining patients with newly diagnosed AD (n = 1,209) were included (Fig. 1). According to the diagnostic criteria of the National Institute on Aging-Alzheimer’s Association (NIA-AA) workgroups,16 a clinical diagnosis of AD can be made if the patient presents the typical features of AD, such as gradual worsening and deterioration of cognitive and non-cognitive functions, while other underlying causes of dementia, such as cerebrovascular disease, are excluded. We also defined AD as a diagnosis made by experienced neurologists under the core clinical criteria for probable AD, as outlined by the NIA-AA workgroups.1617
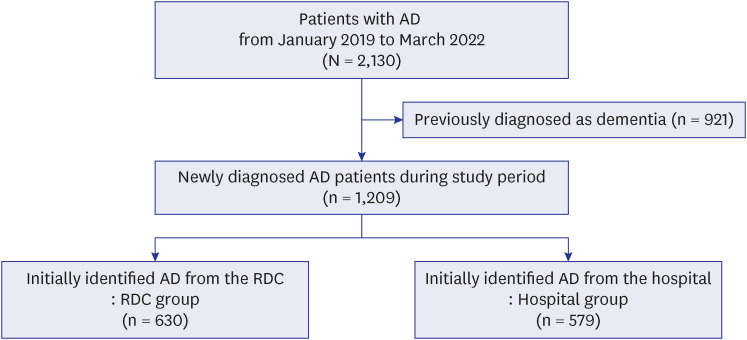
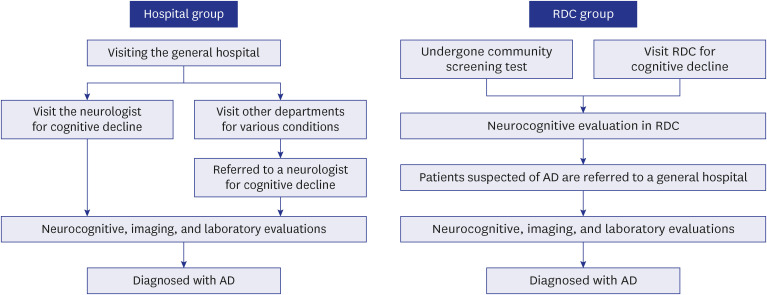
Subsequently, the participants were divided into two groups, the hospital and RDC groups. The hospital group consisted of patients newly diagnosed with AD by experienced neurologists at the general hospital, either by those who visited the hospital’s neurology departments because of worsening cognition or were referred for cognitive decline by other departments in the hospital. The RDC group consisted of patients who were newly diagnosed with AD by neurologists at the general hospital, of whom were suspected of having dementia through screening and neurocognitive tests performed at one of the two RDCs in Pohang region. These patients were subsequently referred to the hospital to consult a neurologist, who confirmed AD diagnosis after the same protocol for brain imaging and blood tests was performed for both groups (Fig. 2). The hospital that performed this study is the secondary general and cerebrovascular-specialty hospital in Pohang city. All included patients were diagnosed by three neurologists who co-authored this study at the same general hospital during the study period. In addition, to give primary care to patients with AD during the study period, they were dispatched to two RDCs in Pohang city.
Clinical assessments
Basic information about patients at the time of diagnosis of AD was obtained from electrical health records, namely age, sex, insurance type (Medical-aid, near poverty, and national health insurance), residential area (dong regions or eup/myeon regions), smoking/alcohol behavior, and comorbidities such as hypertension, diabetes, dyslipidemia, coronary artery disease, arrhythmias, stroke, traumatic brain injury, and thyroid disease. All patients underwent laboratory tests for differential diagnosis at the time of diagnosis.
Patients underwent neurocognitive function tests at the time of diagnosis and 1 year after the initial diagnosis. The education level of the patients was confirmed by the patient or caregiver at the time of their first cognitive function evaluation and was categorized into five categories: illiterate, ≤ 3 years, ≤ 6 years, ≤ 12 years, and > 12 years. In terms of assessing neurocognitive functions, we utilized the Mini-Mental Status Examination (MMSE) and clinical dementia rating sum of boxes (CDR-SB) as the primary evaluation tools, along with additional evaluation for behavioral patterns, mood, and activities of daily living.
Global cortical atrophy was measured through a visual assessment of brain computed tomography (CT) or magnetic resonance imaging (MRI) at the time of diagnosis, and was graded by an experienced neurologist (Supplementary Table 1).18
Statistical analysis
The Shapiro-Wilk test was applied to the normality test of continuous variables, and then expressed as mean ± standard deviation. Categorical variables were expressed as frequency (proportion). For comparative analysis, an independent t-test was used for continuous variables, and the χ2 test was used for categorical variables, respectively. Linear regression models have been established to determine the degree of cognitive change 1 year after initial diagnosis. In the linear models, outcomes were defined as fractions–a percentage change from baseline–as shown in the following equations19:
• ΔMMSE (%) = ([Initial MMSE − 1 Year MMSE]/Initial MMSE) × 100
• ΔCDR-SB (%) = ([1 Year CDR-SB − Initial CDR-SB]/Initial CDR-SB) × 100
Furthermore, we performed binary logistic regression to analyze risk factors for hospitalization within 1 year after diagnosis. For the binary logistic and linear regression models, we applied incremental models to adjust confounders as follows:
• Model I: Hospital or RDC group (univariable)
• Model II: Model I + age, sex, and education level
• Model III: Model II + global cortical atrophy, hemoglobin level, and initial MMSE score
We used the variation inflation factor < 10 to confirm the multicollinearity of each model. Complete case analysis was performed, and a P value < 0.05 was defined as statistical significance. We used the R software version 4.2.2 (R Core Team, R Foundation for Statistical Computing, Vienna, Austria) for all analyses.
Ethics statements
This study protocol was reviewed and approved by the Institutional Review Board of Pohang Stroke and Spine Hospital (approval number: PSSH0475-202205-HR-009-01). Requirement for informed consent was waived due to the retrospective nature of the study design. This study was also conducted in compliance with the Declaration of Helsinki.
RESULTS
Baseline characteristics
A total of 1,209 patients were finally included in this study. There were 579 patients in the hospital group and 630 in the RDC group. The mean age of the RDC group was 80.1 ± 6.6 years, which was significantly higher than that of the hospital group (P < 0.001). Meanwhile, the RDC group had a significantly lower proportion of males (31.9% vs. 38.3%; P = 0.022) and significantly higher alcohol consumption rate (12.4% vs. 3.3%; P < 0.001) than that of the hospital group. In the hospital group, the prevalence of dyslipidemia (21.8%) and previous stroke (33.9%) was significantly higher than that of the RDC group (P < 0.001 and P < 0.001, respectively). The rate of follow-up loss at 1 year was found to be significantly higher in the RDC group (48.3% vs. 39.0%; P = 0.001) (Table 1).
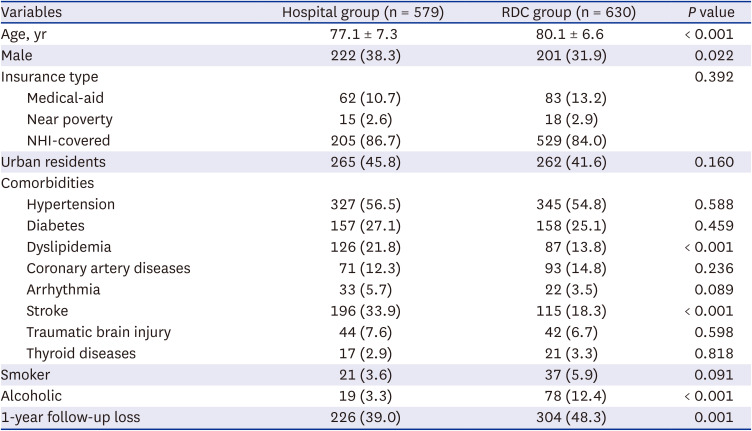
Table 1
Baseline characteristics of participants
Values are presented as mean ± standard deviation or number (%).
NHI = national health insurance, RDC = regional dementia center.
![]()
The initial laboratory findings for each group are presented in Supplementary Table 2. The RDC group showed significantly lower hemoglobin levels (12.2 ± 1.6 vs. 12.5 ± 1.6; P = 0.001) and higher erythrocyte sedimentation rates (26.3 ± 20.9 vs. 23.4 ± 20.7; P = 0.020) than that in the hospital group.
Initial neurocognitive and neuroimaging assessment
We confirmed that the level of education was significantly lower in the RDC group than that in the hospital group (P < 0.001). In the initial neurocognitive function test, the RDC group scored 14.5 ± 5.5, showing a significantly lower MMSE score than those in the hospital group with 16.6 ± 5.9 (P < 0.001). The score of instrumental activities of daily living was also significantly lower in the RDC group than that in the hospital group (17.6 ± 11.2 and 19.4 ± 13.4, respectively; P = 0.017). Conversely, the neuropsychiatric inventory score was 12.1 ± 9.6 in the RDC group, which was significantly higher than that of the hospital group of 10.3 ± 9.6 (P = 0.003). Finally, the global cortical atrophy grade was significantly higher in the RDC group than that in the hospital group (P < 0.001). The initial CDR-SB score did not significantly differ between both groups (Table 2).
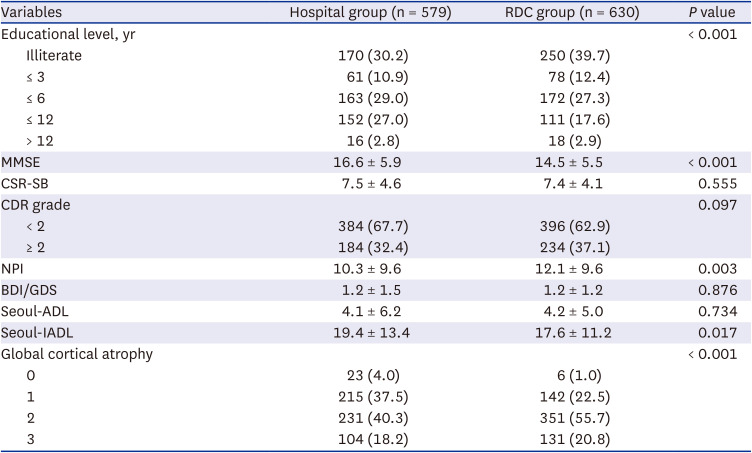
Table 2
Initial neurocognitive features
Values are presented as mean ± standard deviation or number (%).
ADL = activities of daily living, BDI = Beck Depression Inventory, CDR = clinical dementia rating, CDR-SB = clinical dementia rating sum of boxes, GDS = geriatric depression scale, IADL = instrumental activities of daily living, MMSE = Mini-Mental Status Examination, NPI = neuropsychiatric inventory, RDC = regional dementia center.
![]()
One-year follow-up neurocognitive assessment
Of the overall patients, 679 completed the 1-year follow-up, of whom, 326 were in the RDC group, and 353 were in the hospital group. The MMSE score after 1 year was 15.2 ± 5.6 in the RDC group, which was still significantly lower than the 16.5 ± 6.3 score in the hospital group (P = 0.004); however, there was no significant difference in ΔMMSE value (%) between the two groups. Conversely, CDR-SB after 1 year did not show a significant difference between the two groups, but ΔCDR-SB showed a significant increase of 46.2 ± 69.1% in the RDC group compared to the 26.9 ± 64.0% in the hospital group (P <0.001). After 1 year, a total of 51 patients experienced hospitalization events, of whom 19 (5.8%) belonged in the RDC group and 32 (9.1%) belonged in the hospital group; however, this was not a significant difference (P = 0.110) (Table 3).

Table 3
One-year outcome
Values are presented as mean ± standard deviation or number (%).
CDR-SB = clinical dementia rating sum of boxes, MMSE = Mini-Mental Status Examination, RDC = regional dementia center.
![]()
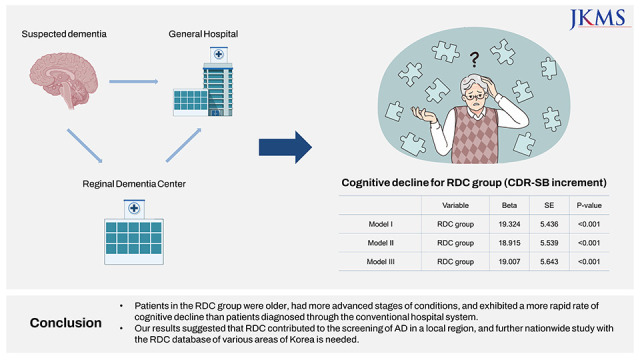
In the linear regression models, the RDC group did not significantly affect the change in MMSE at the 1-year follow-up (β = 3.093 and P = 0.245) (Supplementary Table 3). In the case of CDR-SB change, the RDC group independently associated the CDR-SB increment (for Model III: β = 22.360, R2
= 0.048, and P < 0.001) (Table 4, Supplementary Table 4). In the multivariable binary logistic regression model that evaluated hospitalization within 1 year after initial diagnosis, it was confirmed that the RDC group showed a significantly lower risk for hospitalization within 1 year after AD diagnosis (for Model III: odds ratio, 0.52; 95% confidence interval, 0.28–0.95; P = 0.032) (Table 5, Supplementary Table 5).

Table 4
Linear models for predicting the change of 1-year clinical dementia rating sum of boxes
| Models | Variable | β | SE | R2 | P value |
|---|---|---|---|---|---|
| Model I | RDC group | 19.324 | 5.436 | 0.000 | < 0.001 |
| Model II | RDC group | 18.915 | 5.539 | 0.015 | < 0.001 |
| Model III | RDC group | 22.360 | 5.573 | 0.048 | < 0.001 |
![]()

DISCUSSION
This study investigated the clinical characteristics of patients initially diagnosed with AD at RDCs and a general hospital in Pohang city in Korea. Our findings suggested that patients in the RDC group had a more severe cognitive decline at diagnosis and faster rate of cognitive decline than those in the hospital group. Conversely, the hospital group had a higher prevalence of comorbidities and a relatively higher risk of all-cause hospitalization after AD diagnosis. To the best of our knowledge, this study is the first report on the clinical characteristics of patients with AD screened at RDCs since its implementation in Korea. Moreover, we observed the distinct roles of each institution in the diagnosis of AD through comparisons between the hospital and RDC groups, which sufficiently strengthened this study.
Our results showed that the patients in the RDC group were often diagnosed during the advanced stages of AD. Additionally, it was observed that the education level of those in the RDC group was significantly lower than those in the hospital group, which is consistent with previous findings that the lower the education level, the higher the possibility of delayed AD diagnosis.2021 In contrast, the hospital group had a higher prevalence of comorbidities such as dyslipidemia and stroke, and therefore, might have had more frequent screenings, contributing to early diagnosis and relatively slower rate of neurocognitive decline in functions as opposed to those in the RDC group. This is supported by the finding that the hospital group had a significantly higher risk of hospitalization within 1 year after diagnosis of AD than those in the RDC group.
Bradford et al.,22 through a systematic review, classified the causes of missed or delayed diagnosis of dementia into the following: provider, patient/caregiver, and systemic factors. Aside from identifying patients with dementia on a policy basis, RDCs were implemented to provide easily accessible resources for dementia screening in any region of the country.1323 According to the classification by Bradford et al.,22 this can be said to be an effort in terms of modifying the system factors from a policy perspective. Through our findings, we can infer that RDCs fulfill their purpose to some extent in terms of screening patients with low levels of health-seeking behavior in the community for AD and referring them to general hospitals. However, compared to general hospitals, RDCs may not have fully succeeded in their role of early AD screening in the community. We propose several factors that may have contributed to this aspect. In the hospital group, patients may have possibly sought care at a relatively earlier stage due to worsening cognition or other medical problems. Additionally, in a hospital setting, the clinician’s outlook is crucial in diagnosing AD.24 On the contrary, it should be noted that in RDCs, screening tests could only be performed when patients or caregivers were aware of the symptoms.25 This implies that despite the correction of systemic factors, the influence of patient or caregiver factors still persists.
Socioeconomic status and area of residence generally affect health-seeking behavior,26 and have also been identified as risk factors for dementia in previous studies in Korea.2327 However, our results showed no significant differences between the two groups in terms of insurance type and urban residency rates. This may be attributed to the limitation of using only three categories of socioeconomic parameters based on health insurance types, which may be too simplistic to reflect the actual economic gap. Furthermore, the null finding concerning any difference between urban and rural areas may be due to the fact that this study was based on a single local region.
Our study has the following limitations. First, this was a retrospective study based on RDCs in a single region. To validate the results of this study, a systematic study based on data from RDCs of various regions in Korea is needed in the future. Second, outcomes were based solely on MMSE and CDR-SB values at the 1-year follow-up point. This was due to many missing values and the relatively higher follow-up loss rate among elderly patients, which could potentially bias our results as this study was not a systematized prospective study. As a result, our findings were unable to reflect changes in various neurocognitive features. Meanwhile, the significantly higher follow-up loss rate in the RDC group disproved that an individual’s health-seeking behavior affects the timing of AD diagnosis. Third, we conducted a study targeting only patients with AD, and there was a limitation in not reflecting various types of dementia. Future studies are needed to verify whether the results of this study are valid in other subtypes of dementia. Fourth, though we evaluated global cortical atrophy, we could not assess other essential MRI-based parameters such as white matter hyperintensity and medial temporal atrophy. This was because at initial diagnosis most patients underwent brain CT, not MRI, due to cost-effectiveness and national health insurance service coverage.
In conclusion, patients diagnosed in RDCs presented more advanced AD features and faster rate of cognitive decline than those diagnosed at the general hospital. This is attributable to the differences in educational level, health-seeking behavior, or frequency of exposure to experts. Our results suggest that RDCs have contributed to community-level screening and the healthcare delivery system of patients with AD. It is necessary to establish a well-organized diagnosis, treatment, and long-term care system for patients with AD by combining the RDCs with the conventional healthcare delivery system of Korea. For this, a systematic study based on the RDC database of various regions in Korea is needed in the future, and our research holds significance as a referring study for this purpose.
 XML Download
XML Download