

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Congenital cytomegalovirus (CMV) infection affects 0.7% of live births worldwide, and varies from 0.2 to 2.0% of live births according to region.12 About 10% of live births with congenital CMV have variable clinical manifestations during the newborn period. According to a recent multicenter research conducted in Korea, the birth prevalence of symptomatic congenital CMV infection was 0.11% from 2009 to 2015.3 However, the majority of congenital CMV-infected newborns are asymptomatic. Approximately 50% of symptomatic infants will have permanent neurologic sequelae, and 10% of infants asymptomatic in the neonatal period develop hearing loss later due to CMV infection.456 The most common neurologic sequelae among neonates with congenital CMV infection is hearing loss followed by cognitive impairment, retinitis, and cerebral palsy.4
Congenital CMV infection occurs due to vertical transmission through the placenta during pregnancy. In primary maternal CMV infection, the vertical transmission rate of CMV reaches 30% to 40%, compared with only 1% following secondary maternal CMV infection.7 Moreover, severe symptoms at birth and long-term sequelae are seen more frequently among children who born to women with primary infection during pregnancy.8 However, the risk of actually acquiring congenital CMV during pregnancy is relatively high for seropositive women, in nation-wide sight.8 In Korea, since seropositivity for CMV IgG is as high as 95.8% among women of childbearing age,910 it can be assumed that secondary infection will be more significant and diagnosis by maternal serologic tests has limited value.
Unfortunately, there have been very few reports examining congenital CMV in Korea and there are no national data assessing the prevalence of congenital CMV infection during pregnancy. Recently, otolaryngological analyses found that 33.3% of individuals with congenital CMV infections had sensorineural hearing loss (SNHL), confirming CMV as a significant cause of neonatal and infant SNHL in Koreans as well.11 Meanwhile, recent pediatric research identified a correlation between brain magnetic resonance imaging and neonatal neurologic outcomes (or SNHL).12 However, these studies did not include clinical information regarding maternal immune status or neonatal manifestations. The whole spectrum of congenital CMV infection from pregnancy to long-term outcomes of children remains poorly understood.
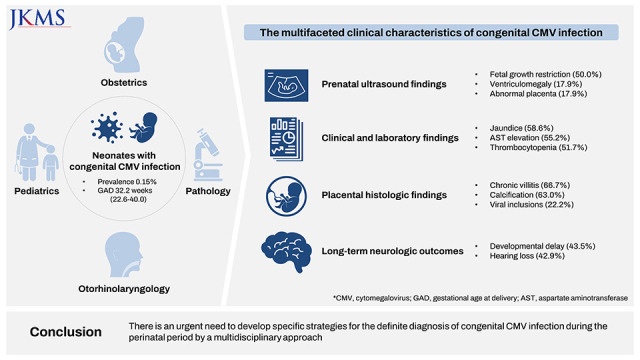
The aim of this study was to analyze multifaceted clinical characteristics of congenital CMV infection from diagnosis to treatment by a multidisciplinary approach including obstetrics and gynecology, pediatrics, pathology, and otorhinolaryngology-head and neck surgery.
METHODS
This is a retrospective descriptive study including 30 consecutive cases of congenital CMV infection diagnosed in our institution, a tertiary hospital located in Seoul, Korea from January 2009 to December 2020.
Congenital CMV infection was defined as a positive result by polymerase chain reaction (PCR) or CMV IgM serology test from neonatal blood, urine, saliva or cerebrospinal fluid within 3 weeks after birth. During the study period, diagnostic tests were performed within 3 weeks after birth for neonates who satisfy one or more of followings: maternal symptoms or sign which suggest primary CMV infection, one or more prenatal abnormal sonographic findings (suspected fetal growth restriction [FGR], abnormal placenta, ventriculomegaly, ascites, pericardial effusion, echogenic bowel, and hydrops) or one or more postnatal characteristics which suggest congenital CMV infection (small for gestational age [SGA], microcephaly, intracranial calcification, ventriculomegaly, jaundice, aspartate aminotransferase [AST] elevation, thrombocytopenia, retinitis, and seizure). After patient selection, we retrospectively reviewed medical records and extracted data for whole clinical characteristics from suspicion during pregnancy to treatment after birth of congenital CMV infection as obstetrics and gynecology and pediatrics aspects. We also obtained data of infant on multidisciplinary approach including pathology, and otorhinolaryngology-head and neck surgery, where possible. Maternal characteristics and obstetrical outcomes included parity, preeclampsia, gestational diabetes, delivery mode, and results of maternal CMV serology tests (when available). Prenatal sonographic findings suggesting congenital CMV infection included suspected FGR, abnormal placenta, ventriculomegaly, ascites, pericardial effusion, echogenic bowel, and hydrops. FGR was defined as fetal ultrasound estimated birth weight < 10th percentiles for gestational age. Abnormal placenta was defined as placentomegaly or placental calcification (≥ grade 2). Placentomegaly was diagnosed if the placental thickness exceeded 4 cm in the second trimester or 6 cm in the third trimester. Placental calcification was classified by the Grannum grading system as previously defined.13 In detail, grade 2 displays echogenic lines throughout all depths and hyperechoic, comma-shaped curves extending from the chorionic plate into the placenta and grade 3 shows extensive basal echogenicity and complete indentations of the chorionic plate. Clinical characteristics of infants included sex, birth weight, SGA, microcephaly, intracranial calcification, ventriculomegaly, jaundice, AST elevation,14 thrombocytopenia, retinitis, seizure, and death. SGA was defined as neonatal birth weight < 10th percentiles for gestational age, and described according to a reference table with data from the Korean Statistical Information Service (2008–2012).15 Microcephaly was defined when a pediatric examination within one year of age confirmed that the head circumference was less than 3 standard deviations for the corrected age at least once. Intracranial calcification and ventriculomegaly were evaluated by first brain sonographic examination within a month of age. Jaundice was defined when phototherapy was administered. AST elevation was defined as AST > 40 U/L within a month of age. Thrombocytopenia was defined as platelet count less than 100,000/mm3. The presence of seizure was judged according to the presence of symptoms or EEG abnormalities. To confirm CMV retinitis, ophthalmic examinations were performed during hospitalization or through outpatient clinics, and the diagnosis was made by an ophthalmologist.
Placental findings were assessed by a single pathologist (JSK) who specialized in placental pathology. The histology of the placenta was reviewed after study enrollment to evaluate chronic villitis, plasma cells, viral inclusions, chorionic vasculitis, calcification, hemosiderin, stromal fibrosis, delayed maturation, acute chorioamnionitis, and funisitis, which are reported to be common histologic findings of CMV infected placenta.16
As for long-term outcomes, developmental delay and hearing loss were also investigated. Developmental delays were clinically assessed by pediatricians or rehabilitation physicians in children at least 1 year of age and/or by Denver II or Bayley II/III tests within 3 years of age. Hearing loss was evaluated as a long-term outcome only when the results of otolaryngology examinations after at least 1 year of age were known. In Korea, the automated otoacoustic emissions (OAE) or automated auditory brainstem response (AABR) test is implemented as a newborn hearing screening test after birth.
After a diagnosis of congenital CMV infection, postnatal antiviral therapy was started according to the decision of pediatric infection specialist. There was a change in the treatment regimen during the follow-up period. Until March 2015, patients were treated with intravenous ganciclovir for 6 weeks. However, six months of oral valganciclovir treatment was reported to improve long-term outcomes of symptomatic congenital CMV disease in 2015.17 From November 2015 on, we applied treatment with oral valganciclovir for six months for moderate to severely symptomatic congenital CMV disease.
Categorical statistics were expressed as number (percentage). Continuous data were expressed as median and range. The presence of abnormal histological findings of the placenta according to long-term neurologic impairment was assessed using Chi-square or Fisher’s exact tests. A two-tailed P value below 0.05 was considered statistically significant. All statistical analyses were carried out using the Statistical Package for Social Sciences version 25 (SPSS Statistics; IBM, Armonk, NY, USA).
RESULTS
Among 19,385 deliveries at our institution during the total study period (January 2009 to December 2020), the prevalence of symptomatic congenital CMV infection was estimated to be 0.15% (n = 30).
Clinical characteristics of prenatal period
As summarized in Table 1, median maternal age was 31 years and parous women accounted for 65.5% of the sample. Median gestational age at delivery was 32.2 weeks (22.6–40.0). Among 29 mothers, 19 (65.5%) delivered preterm (< 37 weeks). Among them, spontaneous preterm delivery occurred in 11 cases (57.9%). The most common indication for preterm delivery was non-reassuring fetal heart rate (6/19; 31.6%), followed by chorioamnionitis (1/19; 5.3%) and maternal severe preeclampsia (1/19; 5.3%). The most common abnormal sonographic finding was FGR (50%) followed by ventriculomegaly (17.9%) and abnormal placenta (17.9%) defined as thick placenta and calcification. Other abnormal sonographic findings included ascites (10.7%), echogenic bowel (10.7%), pericardial effusion (7.1%), and hydrops (7.1%). No abnormal prenatal sonographic findings were observed in one third of births.
Table 1
Maternal characteristics and prenatal USG findings in pregnancies with congenital CMV infection
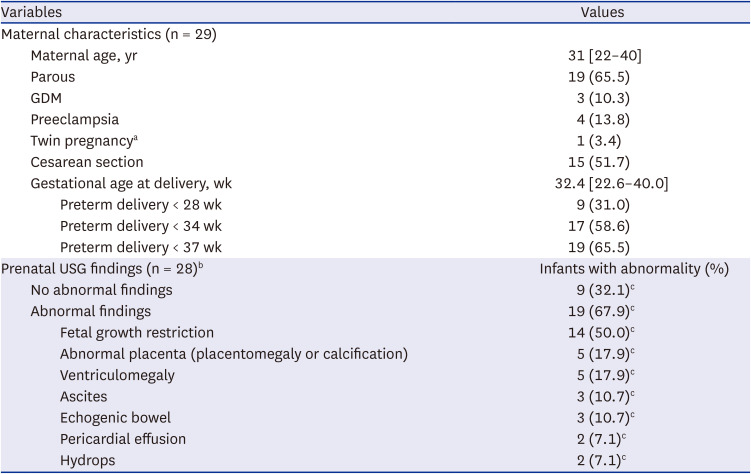
Categorical statistics are expressed as number (percentage) and continuous data are expressed as median and range.
USG = ultrasonography, CMV = cytomegalovirus, GDM = gestational diabetes mellitus.
aBoth babies had congenital CMV infections and were delivered at 32 complete weeks.
bTwo cases were excluded because they were delivered before ultrasound examination, immediately after transfer to our institution.
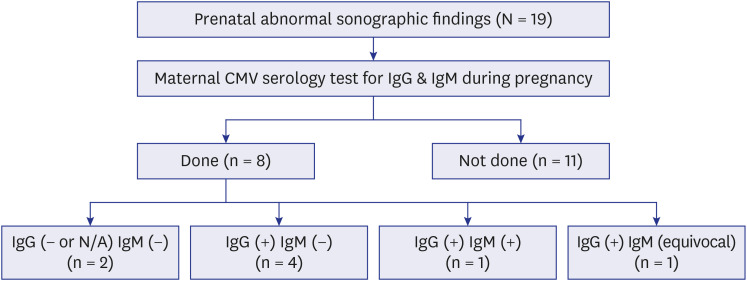
Fig. 1 depicts the flowchart of maternal CMV serology tests among cases of abnormal sonographic findings (n = 19). We found that only 8 mothers underwent maternal CMV serology test for IgM with or without IgG test during pregnancy and there were only 2 cases of positive or equivocal IgM, indicating very low rates of suspected primary infection.
Postnatal findings during neonatal period
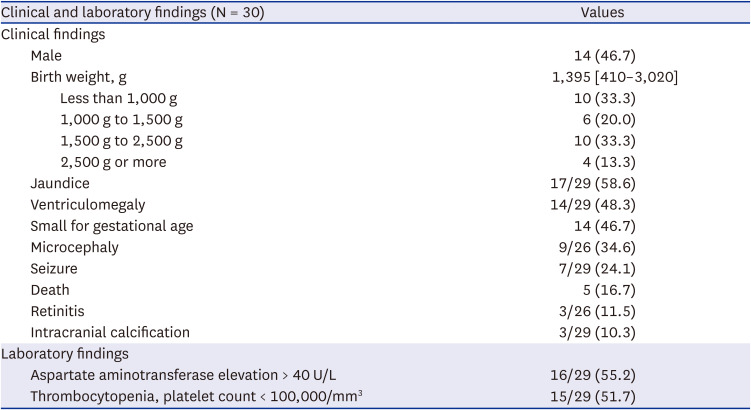
Table 2 summarizes clinical and laboratory findings of infants with congenital CMV infections. Median birth weight was 1,395g [410–3,020]. The most common clinical manifestation of neonates with CMV infection was jaundice (58.6%), followed by ventriculomegaly (48.3%). Among laboratory findings, AST elevation (55.2%) and thrombocytopenia (51.7%) were observed in about half of the subjects. The mortality rate of our CMV cases was 16.7% (n = 5), all of them occurred in extreme preterm birth (range 22.6–26.3 weeks). In detail, three of them died for pulmonary hypertension, and the other two died due to complications from tension pneumonia and extremely low birth weight. Only infants with moderate to severely symptomatic congenital CMV disease were treated, while mildly symptomatic patients were followed without treatment. Infants with moderate to severely symptomatic congenital CMV disease were identified when they showed more than one of the following symptoms and signs: low platelet count, petechiae, hepatomegaly, splenomegaly, intrauterine growth restriction, elevated liver enzymes or total bilirubin, chorioretinitis, CMV DNA detection in cerebrospinal fluid, microcephaly, radiographic abnormalities of the central nervous system such as ventriculomegaly, intracerebral calcifications, periventricular echogenicity, and cortical or cerebellar malformations.6 In our study, 56.7% (17/30) of the congenital CMV infants received antiviral treatment with ganciclovir or valganciclovir in 15 and 8 cases, respectively. Six infants were treated with ganciclovir followed by valganciclovir. Six out of 14 infants who received anti-viral treatment with long term outcome available were found to have developmental delays, whereas 4 out of 9 cases who were followed without treatment showed developmental delays (42.9% vs. 44.4%; P = 1.000). Hearing loss were observed in 8 out of 14 individuals who got anti-viral treatment and in 1 out of 7 cases that were followed without treatment (57.1% vs. 14.3%; P = 0.161). These results suggest that patients with moderate to severely symptomatic congenital CMV disease could have similar long-term outcomes with mildly symptomatic infants by the proper anti-viral treatment.
Table 2
Clinical and laboratory findings of infants with congenital cytomegalovirus infection
Placental histologic findings
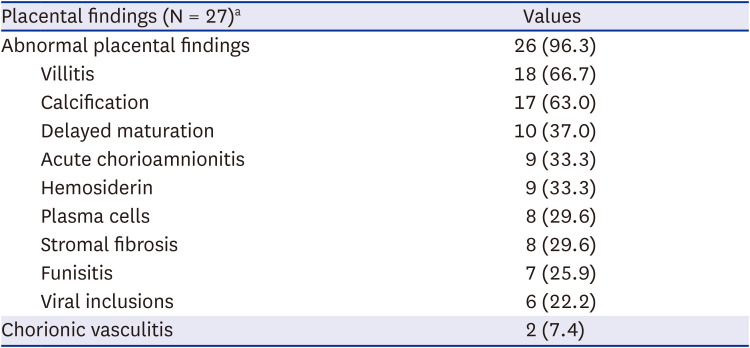
Table 3 summarizes detailed placental findings of congenital CMV infection. The most common histologic finding was chronic villitis (66.7%) followed by calcification (63.0%) and delayed maturation (37.0%). Of note, viral inclusions by CMV were identified in only six cases (22.2%).
Table 3
Placental findings of congenital CMV infection
Long-term neurologic outcomes and hearing loss with follow up
Table 4 summarizes long-term neurologic outcomes and hearing loss of infants with congenital CMV infection. Among cases with complete information available about hearing after 1 year of age, hearing loss was confirmed in 42.9% (9/21) during the follow-up period. Developmental delay was confirmed in 43.5% of infants (10/23), and among these 3 infants were less than 1 kg birth weight. At least 3 of the 6 cases in which viral inclusions were identified in the placenta were found to have developmental delays in long-term outcomes, however, only 7 of the 21 cases without viral inclusions were confirmed to have developmental delays (50.0% vs. 33.3%; P = 0.638). Regarding hearing loss, 1 of 6 cases in which viral inclusions were identified in the placenta were found to have hearing loss, however, 6 of 21 cases without viral inclusion were confirmed as hearing loss (16.7% vs. 28.6%; P = 1.000).
Table 4
Long term neurologic outcomes and hearing loss of infants with congenital cytomegalovirus infection
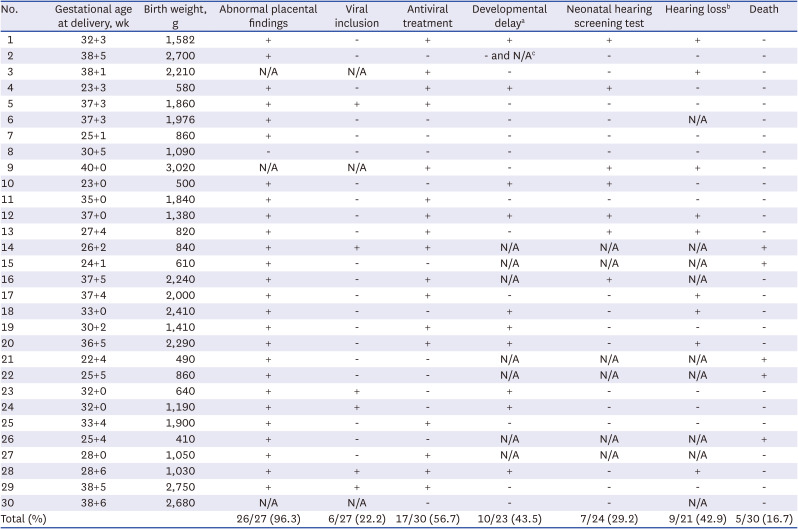
N/A = not applicable.
aClinically assessed by pediatricians or rehabilitation physicians at least 1 year of age and/or by Denver II or Bayley II/III tests within 3 years of age.
bAssessed after 1 year age.
cReached normal developmental milestones at 2 month of age when clinically assessed by pediatricians, but no further data were available due to follow up loss.
DISCUSSION
Our data showed that the birth prevalence of symptomatic congenital CMV infection was 0.15% in our institution, which was lower than the global congenital CMV prevalence at live birth of 0.7%.12 Each year, 0.5 to 1.0% of all newborns in the United States are born with congenital CMV infection,18 and about 0.37% in France.19 According to a recent Japanese cohort study that included universal neonatal screening, the incidence of congenital CMV at a university hospital (0.69%) was higher than in a primary maternity hospital (0.23%, P < 0.01).20 In contrast, our cases of congenital CMV were mostly derived from symptomatic CMV based on clinical suspicion of congenital CMV infection in either the prenatal or postnatal period rather than results of universal screening. In this point, we may underestimate the prevalence of congenital CMV. However, as this study was conducted at a single tertiary institution in Korea where high-risk pregnant women with symptomatic congenital CMV infection are more likely to be admitted, the incidence of congenital CMV infection may be overestimated in regard to the national prevalence.
In general, obstetric suspicion of fetal CMV infection generally occurs based on prenatal ultrasound findings suspicious of viral infection. In our cohort, the most common prenatal ultrasound finding was FGR (50%) followed by ventriculomegaly (17.9%) and abnormal placenta (17.9%). This is consistent with previous review studies, which described the prevalence of ultrasound findings for CMV infection including echogenic bowel (4.5–13%), ventriculomegaly (4.5–11.6%), cerebral calcification (0.6–17.4%), and FGR (1.9–13%).21 Ultrasound image abnormalities were identified in less than 50% of congenitally CMV infected fetuses.621 Similarly, in our study, one third of CMV cases had no abnormal prenatal sonographic findings. Collectively, these results suggest that normal prenatal ultrasounds cannot exclude congenital CMV infection.
At present, routine screening for CMV infection during pregnancy is not recommended, because a clear understanding of disease processes is lacking and early interventions that can change the course of the disease have not been validated.21 However, most healthy women who acquire CMV infections, especially non-primary type infections, during their pregnancy are asymptomatic or have only flu-like symptoms that are not specific to CMV.4 It is hard to suspect congenital CMV infection during pregnancy only with maternal symptoms or signs. Therefore, it is important not to miss any clues indicating congenital CMV, such as prenatal ultrasound findings and postnatal clinical and laboratory findings.
When congenital CMV infection is highly suspected, the best option for prenatal diagnosis is amniocentesis after 21 weeks of gestation and 6 weeks after maternal primary infection.21 However, in our cohort, there was no case in which congenital CMV infection was prenatally diagnosed through amniocentesis. In this study, only 8 women underwent maternal CMV serology tests for IgM with or without IgG tests during their pregnancy, who had abnormal prenatal ultrasound findings. Among them, there was only one case (12.5%) with positive IgM during pregnancy. Therefore, it can be inferred that the possibility of congenital CMV infection due to maternal primary infection was very low in our cohort. In addition, because we did not perform the immunoglobulin avidity test for one case of equivocal IgM, it was impossible to accurately determine the rate of primary CMV infection during current pregnancies in our cohort. We can only deduce that the majority of congenital CMV infections in our cohort originated from seropositive women, which is consistent with the results of previous studies in high seroprevalence countries such as Brazil.822 According to a recent population-based prediction model, about 57 to 96% of all congenital CMV infections occur in infants born to women with non-primary maternal infection during pregnancy in populations with population sero-positive prevalences of 30% to 95%.8 In Korea, seropositivity for CMV infection is very high among women of childbearing age. Therefore, more focus on congenital CMV infections after non-primary maternal infection is required in Korea. It was also indicated that maternal type of infection (primary vs. non-primary) itself was not associated with neonatal symptom and long-term neurologic outcomes.23
Meanwhile, 2–3 weeks after birth, it is very difficult to distinguish congenital CMV infection from postnatally acquired CMV infection by serological methods.1824 Therefore, it is important to detect and perform diagnostic tests for neonates at high risk for congenital CMV infection during the prenatal period or the first 2–3 weeks of life to establish future treatment directions and follow-up plans.18 Early suspicion and diagnosis of hearing loss allow for better outcomes in children with CMV-related SNHL.4
So far, there are no proven therapies to prevent vertical transmission of CMV during pregnancy or treat congenital CMV infected fetuses in utero.21 Some previous clinical trials showed effectiveness of antenatal treatment for congenital CMV infection to prevent maternofetal transmission or to reduce the viral burden in infected fetuses.252627 Ganciclovir and its oral prodrug valganciclovir are the most effective treatments for CMV infection currently available, but because of its extremely high in vitro genotoxicity, they have been labeled potentially teratogenic.22 Acyclovir and its prodrug valaciclovir are other well-known DNA-polymerase inhibitors. A previous clinical study has demonstrated the therapeutic efficacy of high dose valaciclovir in preventing CMV infection in transplant recipients.28 Compared to ganciclovir, valacyclovir is less effective for preventing viral reproduction in CMV infection, but are neither genotoxic nor carcinogenic in vitro or in animals.22 Also, a French study reported efficient placental transfer of valaciclovir, that it is concentrated in the amniotic fluid with no accumulation.26 Administration of valaciclovir 8g/day orally during pregnancy to mothers whose fetal infections were confirmed by amniocentesis resulted in larger proportions of asymptomatic newborns (82%; range 67–88) than in an untreated historical cohort (43%; range 29–57).252627 Therefore, in cases of confirmed congenital CMV infection amniocentesis, particularly in symptomatic cases, maternal therapy with valacyclovir during pregnancy can be recommended after parent counselling. Early treatment of pregnant women with primary infection may prevent termination of pregnancies or delivery of infants with congenital CMV infection, while additional evidence about secondary infection is required.2529
The placenta is the main route for vertical transmission of CMV during pregnancy.16 In our study, all placentas were reviewed and reassessed by a single pathologist (JSK) to evaluate placental histologic findings, which can be associated with congenital CMV infection. Chronic villitis (66.7%) was the most common finding, although it is not specific for congenital CMV infection. Among specific findings, viral inclusions by CMV were observed in only 6 cases (22.2%) in our study, which was much lower than in a previous Japanese study showing the presence of intranuclear viral inclusions in about half of congenital CMV infections.16
Of note, in our study, we also correlated placenta histology with long-term neurologic outcomes. Even though differences in long-term outcomes according to abnormal findings including viral inclusion were not found to be statistically significant, there was a tendency toward neurologic impairment in the viral inclusion-positive cases. In a previous study, the presence of intranuclear inclusions was not significantly different according to the presence of symptoms of congenital CMV infection or maternal infection type (primary or non-primary),16 and there was no association between viral inclusion in the placenta and neurologic impairment. Given that the prediction of long-term outcomes including SNHL is currently limited in clinical practice, further analysis of the relationships between detailed placental pathology in congenital CMV infections and neurologic outcomes, which include quantitative measurements of viral load using real time PCR in placental tissue, in a larger cohort is necessary.
In Korea, all neonates receive routine screening for hearing loss via automated OAE or AABR tests after birth303132 A Korean government-supported newborn hearing pilot project was started in 20079 and routine screening has been covered by national insurance since 2018.32 However, a normal newborn hearing screening test result is not sufficient to rule out hearing loss associated with congenital CMV infection, because 10-15% of children who are asymptomatic at birth will eventually develop hearing impairment.43334 For this reason, we evaluated hearing ability not only by automated OAE of AABR tests after birth but also hearing test results evaluated by an otolaryngologist after 1 year of birth. The prevalence of hearing loss in our cohort was 42.9% (9/21) during the follow-up period. In fact, congenital CMV infection is the most common non-genetic cause of congenital SNHL.35 Clinical spectra of hearing loss associated with CMV infection vary from mild to severe.36 Hearing loss may not be present at birth but later progression or fluctuation of hearing have been noted.3738 Recent study conducted in Korea proposed the clinical significance of CMV diagnostic test after 3 weeks from birth in children with SNHL.39 However, the clinical utility of diagnostic strategy is needed to be examined in further research. In order to evaluate developmental delay, the judgment of the rehabilitation physician and the results of Denver II or Bayley II/III tests were examined and developmental delay was confirmed in 43.5% of infants (10/23). In a 2013 study that explored long-term outcomes of congenital CMV infection at 5 years in Sweden and the United Kingdom, 18% of children with congenital CMV infection suffered developmental impairment. Symptomatic children exhibited noticeably greater neurological sequelae than asymptomatic children (42% vs. 14%, P = 0.006).40
The main strength of this study is that we analyzed the whole spectrum of disease at once through a multidisciplinary approach as a longitudinal study. However, in this retrospective study we included only data from a single center and did not compare congenital CMV infection cases with controls. To address these limitations, a prospective study recruiting mothers to prospectively assess the prevalence and risk factors of congenital CMV infection was started in 2020 and is currently underway at our institution.
Our results emphasize the importance of evaluating congenital CMV infection in Korea and of understanding the clinical manifestation by a multidisciplinary approach. Efforts are needed to reduce neurologic sequelae of congenital CMV infection through early intervention by diagnosing disease without missing single clues during the prenatal period and immediately after birth. Congenital CMV infections have various spectra of signs that include multiple organ systems. Therefore, a multidisciplinary approach, including obstetrics, pediatrics, pathology, otolaryngology, and rehabilitation medicine, is critical for detecting congenital CMV. Also, further studies are needed to establish the cost-effectiveness of universal screening of congenital CMV infection.
 XML Download
XML Download