

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vaccine development is a more time-consuming and resource-intensive process than traditional drug development and focuses on the prevention of disease through administration to healthy individuals. A vaccine for an infectious agent undergoes numerous tests with stringent regulatory requirements and can take up to 5–10 years to be approved and released to the market.1 Nevertheless, the coronavirus disease 2019 (COVID-19) forced the duration of vaccine development to a minimum as the number of infected individuals increased at an alarming rate after the World Health Organization announced the pandemic in January 2020.2 The first COVID-19 vaccine research started in March 2020, and on December 30, 2020, emergency authorization was granted in the UK vaccination program. The first vaccination outside of a trial was rolled out on January 4, 2021.3 This vaccine has since been approved by several medical institutions around the world along with several other types of COVID-19 vaccines. Until recently, about 72% of the world population have been vaccinated against COVID-19.4
COVID-19 vaccines were approved and used at an unprecedented level compared with previous experiences, which resulted in concerns about vaccination and raising questions about the safety of the vaccines.5 For this reason, in the early days after initiating COVID-19 vaccine programs, vaccine hesitance existed worldwide, which limited the vaccine acceptance rate.6 Patients with autoimmune disease and cancer patients showed significantly higher vaccine hesitancy than the healthy population. The main reason for this was safety concerns, as most patients with immunocompromising conditions and patients receiving immunosuppressive medications were excluded from the COVID-19 vaccine clinical trials.78 Over time, numerous studies have emphasized that the benefits of COVID-19 vaccination in autoimmune rheumatic disease (ARD) outweigh the risk of potential vaccine adverse events (AEs),91011 however, there are still reports of more vaccine AEs in patients with ARD than healthy individuals.12 In addition, a growing body of evidence has indicated that the COVID-19 vaccine may induce exacerbations or result in the onset of autoimmune diseases by triggering autoimmunity through mechanisms such as molecular mimicry and the production of specific autoantibodies.13
Evidence for a possible link between certain immunizations and the exacerbation or progression of autoimmune disease has increased over the past few decades.14 Even vaccines that are essential to prevent infection in patients with ARD, such as influenza, pneumococcal, human papillomavirus, and hepatitis B virus vaccines, have reported several cases of worsening underlying autoimmune disease after vaccination.1516 Therefore, we compared the occurrence of underlying disease flares after vaccination against COVID-19 and influenza among patients with ARD to determine whether vaccine-induced autoimmunity differs depending on the type of vaccine. Using a survey, this study also aimed to compare the incidence of AEs following COVID-19 and influenza vaccination and identify the factors associated with AEs and disease flares.
METHODS
Survey participants and data collection
A patient survey was conducted at the Department of Rheumatology, Ajou University Hospital, between November 2021 and March 2022. To participate, subjects were required to have been diagnosed with ARD by physicians and vaccinated against COVID-19 and influenza while receiving treatment for ARD. The study included patients aged 18 years and older and who could read and write Korean or English fluently. Participants without physician diagnosis of ARD and participants who were not able to read Korean/English were excluded. Medical and nursing staff selected eligible patients among those scheduled for outpatient visits, explained the purpose of the study, and provided questionnaires only to subjects who expressed a willingness to participate in the survey. All surveys were conducted face-to-face by nursing staff during the outpatient clinic visits, and the medical staff received the completed questionnaires directly. Medical history, including the year of diagnosis, demographic data, laboratory data, signs and symptoms of disease, and treatment, was collected by the medical staff through medical records.
Questionnaires
The development of this questionnaire was carried out systematically.17 Five individuals conducted a comprehensive literature review each, and discussed in two groups. After the discussion, 16 items were generated as a draft for the survey questionnaires. Before the main survey, the draft questionnaire was pre-tested with 20 participants of various ages, genders, and underlying ARDs. After completing the questionnaire, participants were required to provide opinions on the necessity, clarity, and relevance of each item. Based on this, three items were removed, and some were merged, resulting in a final survey with a total of 11 items.
The survey consisted of 11 questions (Supplementary Data 1). Question 1 required all participants to indicate a previous diagnosis of the following diseases: rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), ankylosing spondylitis (AS), adult-onset Still’s disease, primary Sjögren’s syndrome, vasculitis, polymyositis/dermatomyositis, and systemic sclerosis (SSc). Questions 2 and 3 related to the types of vaccines previously received (influenza; pneumococcal; zoster; pertussis; hepatitis; human papillomavirus; measles, mumps, and rubella; other vaccines) and reactions or discomfort after vaccination. Questions 4–6 related to COVID-19 vaccination, the patients’ vaccination status (incomplete vaccination/full vaccination/booster dose), and type of vaccine (AstraZeneca/Pfizer/Moderna/Johnson & Johnson/mixed schedule). To the participants who answered “Yes” to the question of “Did you have adverse reactions or a worsening of underlying ARD after COVID-19 vaccination?” we inquired about the following symptoms: localized reactions (redness, swelling, pain, or other), fever, myalgia, fatigue, nausea or vomiting, abdominal pain, generalized swelling, acute allergic reactions (itching, skin rash, swelling in the face or mouth, anaphylaxis), delayed allergic reactions, or any other side effects. We also queried the treatment of AEs and disease flares after vaccination. Questions 7–9 were the same as questions 4–6 but related to the influenza vaccine instead of the COVID-19 vaccine. Questions 10 and 11 were self-reported diagnoses of COVID-19 and influenza after vaccination as ”Yes/No” variables. This questionnaire took 10–15 minutes to complete.
Statistical analysis
All data are expressed as mean ± standard deviation. To determine the normality of distribution, the Shapiro-Wilk test was used. The χ2 test or Fisher’s exact test was used to compare the statistical significance of the differences in the incidence of AEs or underlying rheumatic disease flares following COVID-19 and influenza vaccination. The frequencies of AEs or underlying ARD flares after the mixed or matched vaccines were compared using the same statistical method. Univariate logistic regression was performed to investigate the factors associated with AEs or worsening of ARD after vaccination. After the univariate logistic regression analysis, only a few significant variables (P < 0.05) were used in the subsequent multivariate logistic analysis. The survey data were analyzed using R software (version 3.6.1; R Studio, Boston, MA, USA). A statistical significance level of P value < 0.05 was assumed in all analyses.
RESULTS
Survey participants characteristics
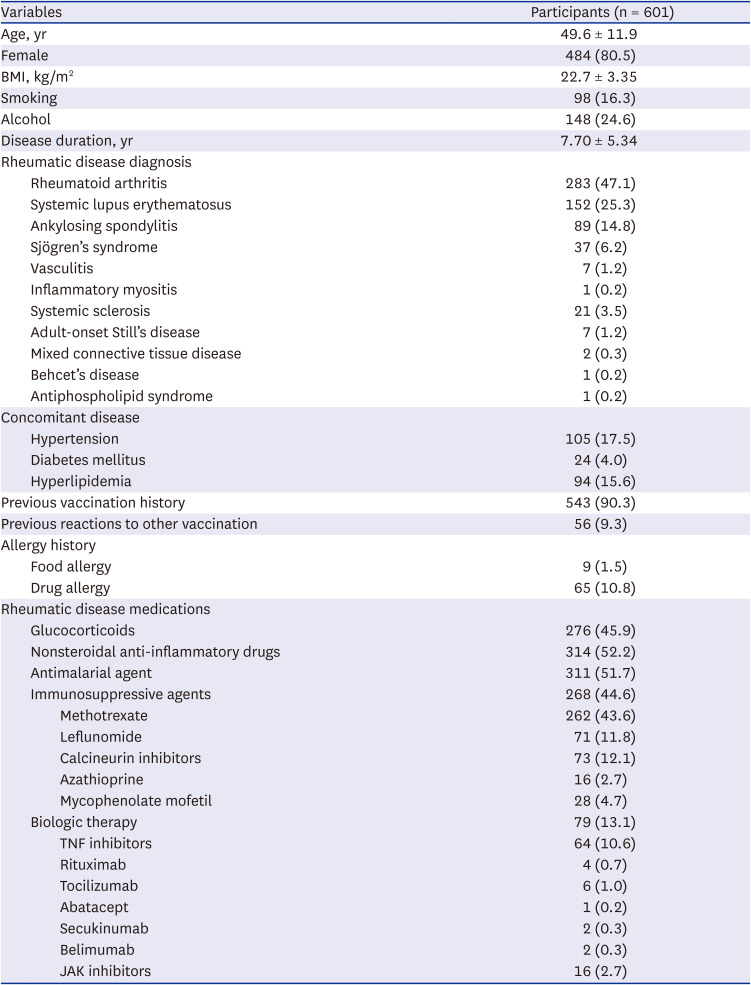
Between November 2021 and March 2022, we analyzed 601 patients with rheumatic diseases who received the COVID-19 vaccination (mean age 49.6 years, 80.5% female). Table 1 summarizes the demographic and clinical data of the participants. A total of 286 (47.1%) patients had RA, 152 (25.3%) had SLE, 89 (14.8%) had AS, 37 (6.2%) had Sjögren’s syndrome, 21 (3.5%) had SSc, and 19 (3.2%) had other rheumatic diseases. The mean disease duration was 7.7 ± 5.3 years. Of these, 543 (90.3%) patients had a history of receiving other vaccines prior to the COVID-19 vaccine and 56 (9.3%) reported experiencing adverse reactions (Supplementary Table 1). Sixty-five (10.8%) patients reported a history of drug allergies and 9 (1.5%) patients reported a history of food allergy. A total of 276 (45.9%) patients with ARD were receiving ongoing treatment with glucocorticoids and 268 (44.6%) were using more than one immunosuppressive agent. Among the patients treated with immunosuppressive drugs, 43.6% used methotrexate, 12.1% used calcineurin inhibitors, 11.8% used leflunomide, 4.7% used mycophenolate mofetil, and 2.7% used azathioprine. A total of 79 (13.1%) patients were treated with biologic therapies: 64 (10.6%) with a tumor necrosis factor inhibitor, 6 (1%) with tocilizumab, 4 (0.7%) with rituximab, 2 (0.3%) with belimumab, 2 (0.3%) with secukinumab, and 1 (0.2%) with abatacept. Sixteen patients (2.7%) were treated with Janus kinase inhibitors (JAKi).
Table 1
Demographic and clinical characteristics of the participants who responded to the survey
Vaccination status and dose
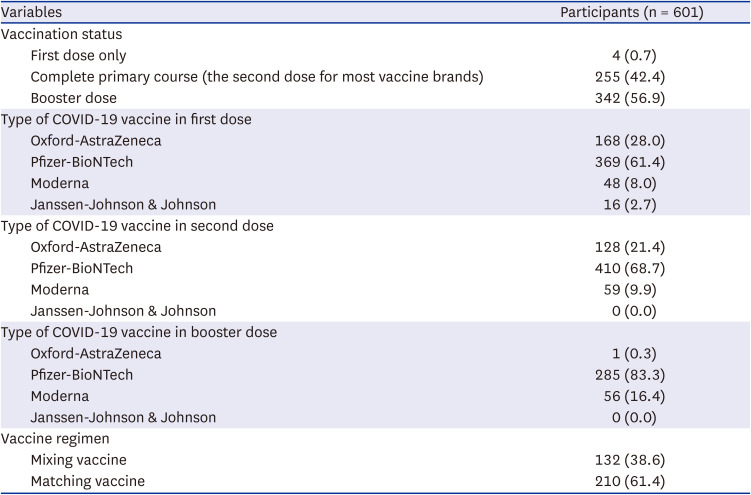
Table 2 lists the types and doses of vaccines administered to the survey participants. Of the 601 patients, 225 (42.4%) completed the primary course, 342 (56.9%) received booster doses, and 4 (0.7%) received only the first dose. The manufacturers of the first dose among the study participants included Pfizer-BioNTech (61.4%), Oxford-AstraZeneca (28.0%), Moderna (8%), and Janssen-Johnson & Johnson (2.7%), and the second dose included Pfizer-BioNTech (68.7%), Oxford-AstraZeneca (21.4%), and Moderna (9.9%). Of those who received a booster dose, 285 (83.3%) patients received Pfizer-BioNTech, 56 (16.4%) received Moderna, and 1 (0.3%) received Oxford-AstraZeneca. A total of 132 (38.6%) patients received mixed vaccines and 210 (61.4%) patients received matching vaccines.
Table 2
Types and frequency of administration of COVID-19 vaccination
Comparing AEs occurring after receiving COVID-19 vs. influenza vaccines
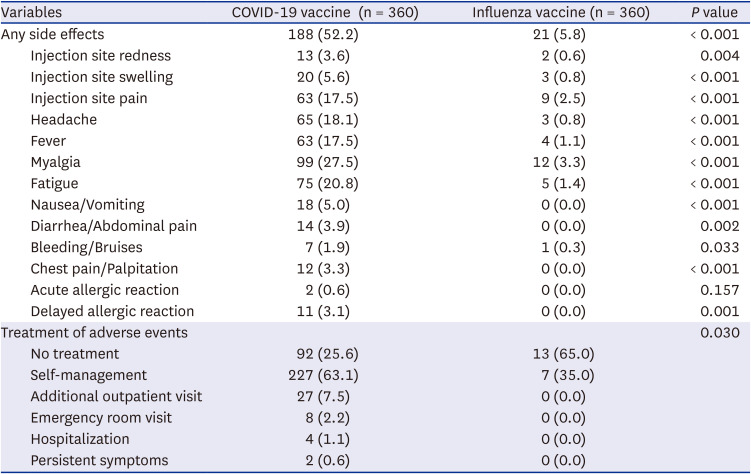
The adverse reactions reported after COVID-19 and influenza vaccinations are shown in Table 3. After vaccination, the AEs associated with the COVID-19 and influenza vaccines were 52.2% and 5.8%, respectively, with significant differences. No severe AEs related to either vaccine were reported. The most frequently reported AE in the COVID-19 and influenza vaccines was myalgia (27.5% vs. 3.3%, P < 0.001). Overall patient-reported AEs occurred more often in the COVID-19 vaccine than influenza vaccine, including injection site redness (3.6% vs. 0.6%, P = 0.004), injection side swelling (5.6% vs. 0.8%, P < 0.001), injection side pain (17.5% vs. 2.5%, P < 0.001), headache (18.1% vs. 0.8%, P < 0.001), fever (17.5% vs. 1.1%, P < 0.001), fatigue (20.8% vs. 1.4%, P < 0.001), nausea/vomiting (5.0% vs. 0.0%, P < 0.001), diarrhea/abdominal pain (3.9% vs. 0%, P = 0.002), bleeding/bruises (1.9% vs. 0.3%, P = 0.033), chest pain/palpitation (3.3% vs. 0.0%, P < 0.001), acute allergic reaction (0.6% vs. 0%, P = 0.157), and delayed allergic reaction (3.1% vs. 0%, P = 0.001). There was no significant difference in the frequency of AEs according to the vaccine manufacturer (P = 0.376, Supplementary Table 2). Comparing the pattern of treatment for vaccine AEs, most did not require treatment after the influenza vaccine (65%), whereas most COVID-19 vaccine-related AEs required self-management (63.1%). There were cases of additional outpatient visits (7.5%), emergency room visits (2.2%), and hospitalizations (1.1%) after receiving the COVID-19 vaccine; however, no patients required such treatment after receiving the influenza vaccine.
Table 3
Adverse events occurring after COVID-19 and influenza vaccination
Comparing underlying disease flares after receiving the COVID-19 vs. influenza vaccines
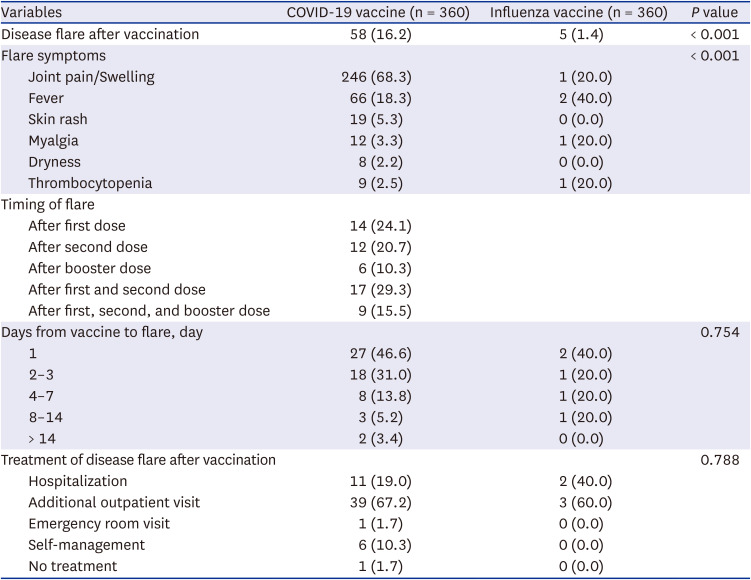
The incidence of ARD flares was higher after the COVID-19 vaccine than after the influenza vaccine (16.2% vs. 1.4%, P < 0.001) (Table 4). Joint pain or swelling (68.3%) was the most common symptom of ARD flares after COVID-19 vaccination. Fever (18.3%), skin rash (5.3%), myalgia (3.3%), thrombocytopenia (2.5%), and dryness (2.2%) were also included in the disease flare symptoms after COVID-19 vaccination. Nearly 80% of the patients developed symptoms of ARD flares within 3 days of COVID-19 vaccination. After influenza vaccination, patients experienced fever (40%), joint pain/swelling (20%), myalgia (20%), and thrombocytopenia (20%), due to ARD flares. Additional outpatient clinic visits were the most common treatment method for ARD flares after COVID-19 and influenza vaccination (67.2% vs. 60%), followed by hospitalization (19% vs. 40%).
Table 4
Flare of rheumatic diseases after COVID-19 and influenza vaccination
Factors associated with AEs and underlying rheumatic disease flares after COVID-19 vaccination
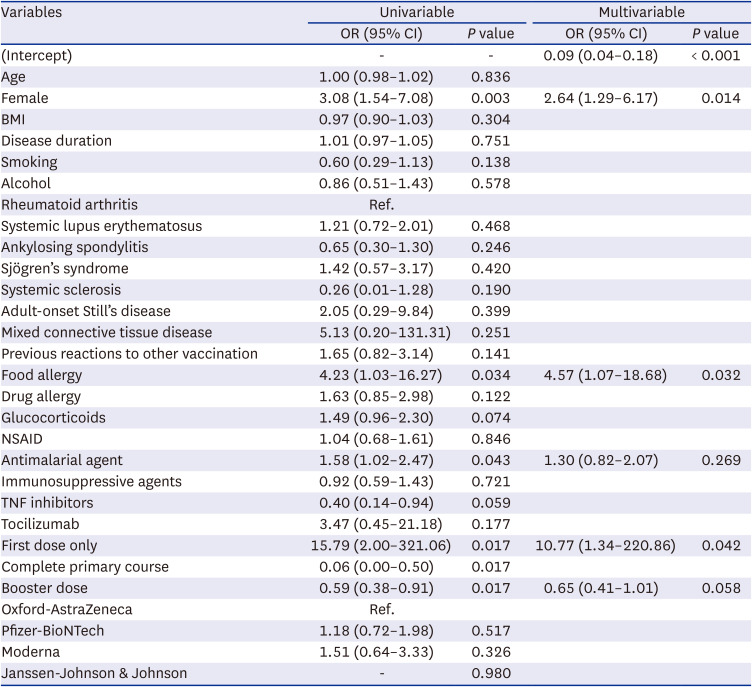
Table 5 shows the results of the analysis of the factors related to AEs after COVID-19 vaccination. AEs occurrence was significantly higher after COVID-19 vaccination in patients who had previously experienced other vaccine AEs (odds ratio [OR], 1.95; 95% confidence interval [CI], 1.07–3.7; P = 0.034), whereas the frequency of AEs decreased significantly in patients who received a booster dose (OR, 0.69; 95% CI, 0.49–0.98; P = 0.040). We also analyzed the risk factors associated with ARD flares after COVID-19 vaccination (Table 6). Multivariate logistic regression analysis revealed that the female sex (OR, 2.64; 95% CI, 1.29–6.17; P = 0.014), food allergy (OR, 4.57; 95% CI, 1.07–18.68; P = 0.031), and first dose only (OR, 10.7; 95% CI, 1.34–220.8; P = 0.041) were associated with ARD flares after COVID-19 vaccination.
Table 5
Multivariable analyses of risk factors for adverse events after coronavirus disease 2019 vaccination
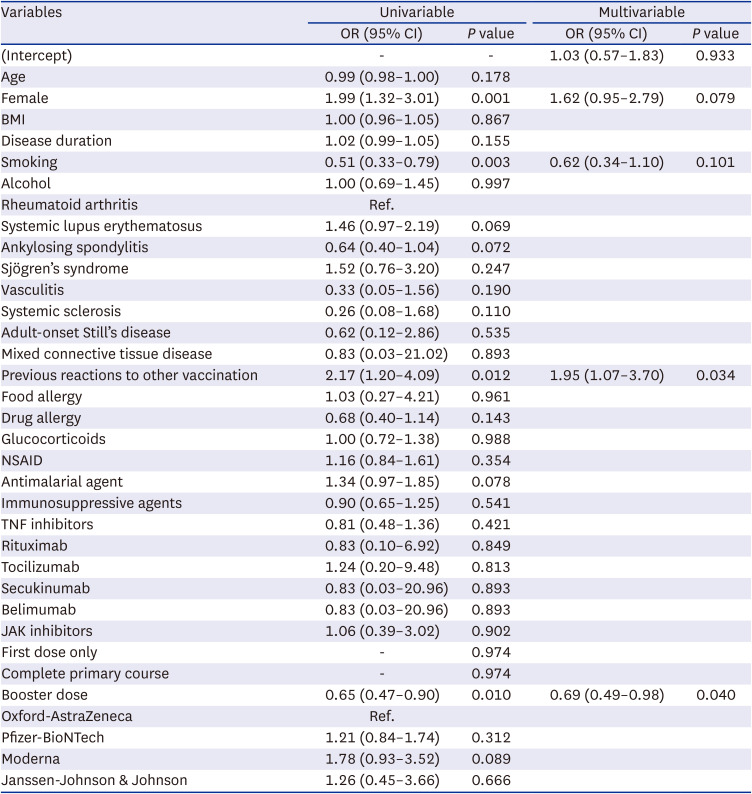
Table 6
Multivariable analyses of risk factors for rheumatic disease flares after coronavirus disease 2019 vaccination
Comparison of mixed and matched COVID-19 booster vaccines
No significant difference was found in the occurrence of reactions after COVID-19 vaccine according to mixed or matched (Supplementary Table 3). Mixed and matched COVID-19 booster vaccinations showed similar frequencies of AEs (48.5% vs. 51.4%, P = 0.596), ARD flares (12.9% vs. 13.3%, P = 0.89), and COVID-19 infections (14.4% vs. 15.2%, P = 0.831). COVID-19 and influenza infection after vaccination were shown in Supplementary Figure 1.
DISCUSSION
To reach the end of the COVID-19 pandemic, it is important to better understand vaccine safety profiles. This can be achieved through post-marketing safety studies by collecting data on the safety, efficacy, and potential risks. Therefore, we conducted a post-vaccination questionnaire survey of patients undergoing treatment for ARD. To the best of our knowledge, this is the first study to compare the incidence of AEs and underlying disease flares after COVID-19 and influenza vaccinations in patients with ARD. AEs after vaccination showed a significant difference of 52.2% for the COVID-19 vaccine and 5.8% for the influenza vaccine; fortunately, most AEs of the COVID-19 vaccine-related AEs could be improved with self-treatment. Participants widely reported common and mild AEs such as myalgia, fatigue, headache, fever, and injection site pain/swelling as post-vaccination reactions, and these findings were consistent with previous studies or manufacturer’s factsheets.1819 A comparative analysis of AEs after vaccination with the COVID-19 mRNA and influenza vaccines in the general population, with data reported on VigiBase, also suggested that mild systemic reactions are more prominent after receiving the COVID-19 vaccine.20 Whereas serious and rare AEs, including cardiovascular or neurologic complications, have been reported with different safety profiles for COVID-19 and influenza vaccines.1920 In this study, there were no severe AEs associated with the COVID-19 and influenza vaccines, such as myocarditis, deep vein thrombosis, or intracerebral hemorrhage, presumably because the survey participants were patients visiting outpatient clinics.
The rate of AEs after influenza vaccination in our study was similar to that of other studies.21
,
22 The proportion of ARD patients who experienced AEs from the COVID-19 vaccine has been reported in a wide range of 30% to 94% (including our results), with differences according to underlying disease, race, and vaccine manufacturer.101223242526 In other Asian countries, such as Japan, China, and Hong Kong, the incidence of AEs was around 70–80%, which is slightly higher than our results.2728 In addition, the frequency of AEs did not differ significantly by vaccine manufacturer in our study; however, when comparing symptoms, injection site redness, diarrhea or abdominal pain, general edema, and chest pain or palpitations were significantly higher in the Moderna vaccine. In the past three years, information on the AEs associated with the COVID-19 vaccine in patients with ARD has become abundant, and it has become difficult to obtain consistent results on the superiority of vaccines according to manufacturer.29303132 Based on the cumulative AE reports from patients with ARD, physicians can recommend a suitable vaccination approach for individual patients, which may help reduce hesitancy and the occurrence of COVID-19 vaccination-related AEs.33
Significant differences were also observed between COVID-19 and influenza vaccinations in terms of underlying disease flares, which is a major post-vaccination problem for patients with ARD. Approximately 11% of the participants reported flares of their underlying diseases after COVID-19 vaccination, consistent with previous findings.11
,
3435363738 Joint pain or swelling was the most common symptom of disease flare, which was expected due to vaccine reactogenicity, and there were no reports of severe disease flares in our study. In contrast, only 1.4% of patients with ARD experienced underlying disease flares after influenza vaccination, which supports the findings of previous studies that showed no correlation between influenza vaccine and rheumatic disease flares.35 The tendency for underlying disease flares to occur within 3 days of vaccination and the required treatment for symptoms did not differ between COVID-19 and influenza vaccines, which was also similar to the results published in several countries.34353639
COVID-19 vaccine development utilizes novel technologies, such as mRNA- and vector-associated vaccines, which differ from conventional influenza vaccines. These technologies result in a higher incidence of AEs and underlying rheumatic disease flares after COVID-19 vaccination than the continuously used influenza vaccines, mainly because of the activation of the immune response caused by COVID-19 vaccines. The mRNA and vector vaccines work by introducing small fragments of the virus’s genetic material into the body. Subsequently, the immune system recognizes this virus fragment and reacts to activate innate immunity, and these small pieces may lead to immune cross-reactivity through molecular mimicry with human proteins.40 Although the COVID-19 vaccine developers modified some structures to reduce these immune responses and safety was carefully evaluated through clinical trials, most of the clinical trials were limited to healthy populations, which would have resulted in different results than that of real-world data.
This mechanism has raised concerns that cross-vaccination with other types of COVID-19 vaccines may increase the frequency or intensity of AEs or cause acute flares of ARDs.41 In South Korea, the AstraZeneca vaccine was the first to be approved and was administered to the initial priority groups, which included immunocompromised patients, with nearly 30% of the AstraZeneca vaccinated patients in the primary course of our study. While booster vaccination in South Korea was mostly provided by Pfizer, and 40% of the patients included in our study received a mixed booster vaccination, there were no significant differences in the incidence of AEs and underlying disease flares. Some studies have reported that mixed vaccination had higher vaccine effectiveness than matched vaccination; however, in this study, there was no difference between mixed and matched in the rate of COVID-19 infection after vaccination.42
After evaluating the benefits and risks associated with COVID-19 vaccines, vaccination can be considered essential, and it is important to determine which features among patients with ARD are associated with AEs or ARD flares. Among the various factors, the only risk factor that increased AEs through multivariate analysis was a previous allergic reaction to other vaccinations. Similar to our findings, there have been several reports of many AEs of the COVID-19 vaccine in patients with a history of allergic reactions to other vaccinations.2343 mRNA vaccines are not an absolute contraindication, even if there is a past vaccine allergic reaction in which excipients such as polyethylene glycol contribute greatly. However, it is recommended that such patients be informed before vaccination that the possibility of minor allergic reactions to COVID-19 vaccines may increase. Other published analysis identified that female sex and an age below 50 were factors related to the risk of AEs.44 On the other hand, patients who received the booster vaccination had a lower frequency of AEs, which can be interpreted as the high rate of booster doses for patients who did not have AEs after the first and second COVID-19 vaccinations. In addition, no significant results were found in our attempt to find a possible correlation between occurrence of AEs and the drugs to treat several rheumatic diseases, especially biologic agents, which was estimated to be due to the insufficient number of patients for each biologic as the study included various ARDs. There have been reports of disease flare after COVID-19 vaccination in patients with RA treated with JAKi and interleukin (IL)-6 inhibitor, and in patients with psoriatic arthritis with IL-12/23 inhibitor.45
Our data also revealed that female sex, a single vaccine dose, and food allergies were factors associated with the occurrence of underlying rheumatic disease flares. This can be explained by the fact that no additional vaccination was received owing to disease flares after the first vaccine dose. The inclusion of female sex in the risk factors for underlying rheumatic disease flares is consistent with previous studies.46 As demonstrated by our results, most of the reports analyzed based on the survey showed that women tended to report more symptoms than men; thus, differences in gender sensitivity may also have contributed to these results.
A significant strength of our study is that, to the best of our knowledge, this is the first study to compare the incidence of AEs of COVID-19 and influenza vaccines in patients with ARD and their effects on underlying diseases. In addition, all surveys were conducted face-to-face, which ensures more information without missing items and a larger number of respondents. However, this study has some limitations. First, there was a lack of information regarding disease activity and the timing, dose, and discontinuation of immunosuppressive agents related to the time of vaccination. Second, although the potential risk of flares varies depending on the ARDs, a sub-analysis was not conducted according to each disease. For the RA, SLE, and AS groups, which include many participants, further research is needed to collect information on disease activities, immunosuppressive agent types, and doses to better understand the risk factors for reactions after vaccination. Finally, the subjective nature of the study design, which was based on self-reported patient data, may have led to an overestimation or underestimation of post-vaccination symptoms, and mild reactions, including myalgia, fever, and joint pain, may have been compounded by AEs or disease flares.
This study compared the incidence of self-reported AEs and underlying disease flares after COVID-19 and influenza vaccines through a survey of patients with ARD. We found that the incidence of AEs and ARD flares after the COVID-19 vaccine was higher than that after the influenza vaccine. We also identified several factors associated with potential disease flares and AEs following COVID-19 vaccination; an allergic reaction history of previous vaccination was found to be related to AEs after COVID-19 vaccination, and female sex was related to the flares of underlying rheumatic diseases.
 XML Download
XML Download