

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is defined as a preventable and treatable airway disease characterized by airflow obstruction due to an enhanced chronic inflammatory response within the airways.1 COPD causes substantial morbidity and mortality, and due to the aging of the population, the economic burden of COPD is continuously increasing.23 Smoking is a known major cause of COPD, and, like noxious particles or gases, causes an inflammatory response in the lungs that leads to airway damage and destruction of the lung parenchyma. This inflammatory response involves not only the airways, but also other chronic diseases such as cardiovascular, metabolic, and other inflammatory comorbidities.4567
Poor oral health (e.g., periodontal disease, dental caries) is a common comorbidity in individuals with COPD.89 For example, poor dental and periodontal health was shown to increase the risk of developing COPD.10 Periodontal diseases can also increase the risk of acute COPD exacerbations by increasing the risk of lower respiratory tract infections.11 Furthermore, edentulous individuals with COPD were shown to be at an increased risk of hospitalization and mortality.12 However, most previous studies have evaluated the association between a specific condition of poor oral health (e.g., periodontitis) and COPD, and few studies have comprehensively evaluated the association between general oral health (including periodontitis, dental caries, denture wearing, number of existing permanent teeth, and tooth brushing habits) and COPD.111314 Furthermore, the association between oral health and the severity of COPD has not been well elucidated.12 Therefore, this study aimed to evaluate the association between poor oral health and airflow limitation (AFL), particularly in terms of the severity of AFL.
METHODS
Study population
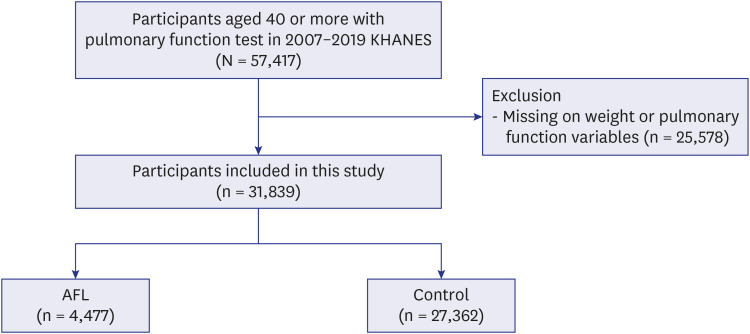
The Korea National Health and Nutritional Survey (KNHANES) is a population-based nationwide survey to assess the health and nutritional status of the noninstitutionalized population of Korea conducted by the Korea Centers for Disease Control and Prevention (KCDC). We used data from the KNHANES IV (2007–2009), V (2010–2012), VI (2013–2015), VII (2016–2018), and VIII (2019). The KNHANES analyses are periodically conducted to assess Korea’s health and nutritional status. Thus, the KNHANES is a nationally representative cross-sectional study conducted by KCDC. The study population was investigated based on a stratified multi-stage sampling method. During the 12 years, 57,417 participants aged 40 years or older underwent pulmonary function tests. Of these, participants with missing weighted variables or pulmonary function variables (n = 25,578) were excluded, and 31,839 individuals were included in the analysis. Of the eligible individuals, we allocated participants to one of two groups according to the presence or absence of AFL (pre-bronchodilator forced expiratory volume in 1 second [FEV1]/forced vital capacity [FVC] < 0.7) (Fig. 1).15 Since post-bronchodilator spirometry was not performed in KHANES, AFL was defined using pre-bronchodilator spirometry. The spirometry equation used in the KHANES data is a Korean spirometry standard equation that meets the requirements recommended by the American Thoracic Society.1617
Classification of severity of AFL
The exposure was AFL, and the severity of AFL was classified as mild (FEV1 ≥ 80% predicted), moderate (50% ≤ FEV1 < 80% predicted), or severe to very severe (FEV1 < 50% predicted).18
The measurement of oral health
Oral health conditions were evaluated using the number of remaining teeth, presence of periodontitis, Decayed, Missing, and Filled Teeth (DMFT) index, and denture use.
The number of existing natural teeth was investigated by a dentist trained in the examination criteria of the National Oral Health Survey. Of the 28 teeth excluding the third molars, the number of existing natural teeth was calculated by excluding teeth that had been lost due to caries, those lost for reasons unrelated to caries, and those with unerupted surfaces. Since previous studies suggested that people cannot chew foods when they have more than 20 teeth missing, which is known as functional dentition,1920 the number of existing natural teeth was categorized into one of three groups as follows: 0–19, 20–27, and 28.921
The World Health Organization (WHO) community periodontal index (CPI) was used to evaluate periodontitis.22 Based on the periodontal pocket measurements, the periodontal status was classified as Code 0 (normal), Code 1 (bleeding periodontal tissue), Code 2 (presence of calculus), Code 3 (shallow periodontal pocket [> 3.5 mm]), or Code 4 (deep periodontal pocket [> 5.5 mm]). The index tooth numbers were 11, 16, 17, 26, 27, 31, 36, 37, 46, and 47 according to the World Dental Federation (FDI) system.23 The CPI probe was used according to the WHO guideline.22 Codes 1 and 2 were classified as normal, and Codes 3 and 4 were classified as periodontitis.
The DMFT index is the sum of an individual’s decayed, missing, and filled permanent teeth.24 The DMFT index has been used since the 1930s as a method for evaluating caries and is one of the simplest and most commonly used indicators in epidemiological investigations.25 The DMFT index was allocated into tertiles designated as 0–4, 5–9, and 10 or more. Denture use was classified into the group without dentures, the group with partial dentures, and the group with full dentures. Regarding habits related to periodontal diseases and oral health, the frequency of daily tooth brushing (categorized as ≤ 2 times/day or ≥ 3 times/day) and the history of dental clinic visits in the last year were evaluated.
Other measurements
Body mass index (BMI), calculated as weight in kilograms divided by height in meters squared, was categorized according to Asian-specific criteria: underweight (< 18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23–24.9 kg/m2), and obese (25.0–29.9 kg/m2).26 Individuals who consumed more than 30 g/day of alcohol were considered heavy drinkers.
Occupation type was categorized into one of five groups according to the 6th Korean Standard Classification of Occupation: manager, professional, office worker; service or sales worker; agriculture or fishery worker; skilled labor or machine operator; and manual laborer.27
Comorbidities (pulmonary tuberculosis, asthma, cardiovascular disease including myocardial infarction or angina, osteoporosis, arthritis, and depression) were defined based on self-reported physician diagnosis.4142829 Diabetes mellitus (DM) was defined as a fasting blood glucose concentration ≥ 7 mmol/L, the current use of anti-diabetic medications, or a self-reported physician diagnosis of DM.30 Hypertension was defined as a self-reported physician diagnosis, the use of antihypertensive medication, a systolic blood pressure ≥ 140 mmHg, or a diastolic blood pressure ≥ 90 mmHg.31 Dyslipidemia was defined as a serum total cholesterol concentration ≥ 6.22 mmol/L, a fasting triglyceride concentration ≥ 2.26 mmol/L, use of lipid-lowering medications, or a self-reported physician diagnosis of dyslipidemia.32
Statistical analysis
All analyses were performed using survey commands in STATA version 15.1 (StataCorp LP, College Station, TX, USA) to account for the complex sampling design and survey weights. All data are presented as weighted percentages with standard errors for categorical variables. Data were compared using Student’s t-test for continuous variables and Pearson’s χ2 test for categorical variables. To evaluate the association between oral health and AFL, multivariable logistic regression analyses were performed. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were estimated after adjusting for potential confounding factors. All analyses were adjusted for age, sex, BMI group (underweight, normal, overweight, or obese), smoking status (never, current, or ex), and comorbidities (pulmonary tuberculosis, asthma, DM, hypertension, dyslipidemia, cardiovascular disease, osteoporosis, osteoarthritis or rheumatoid arthritis, depression). All tests were two-sided, with P values < 0.05 considered to be statistically significant.4
RESULTS
Study population
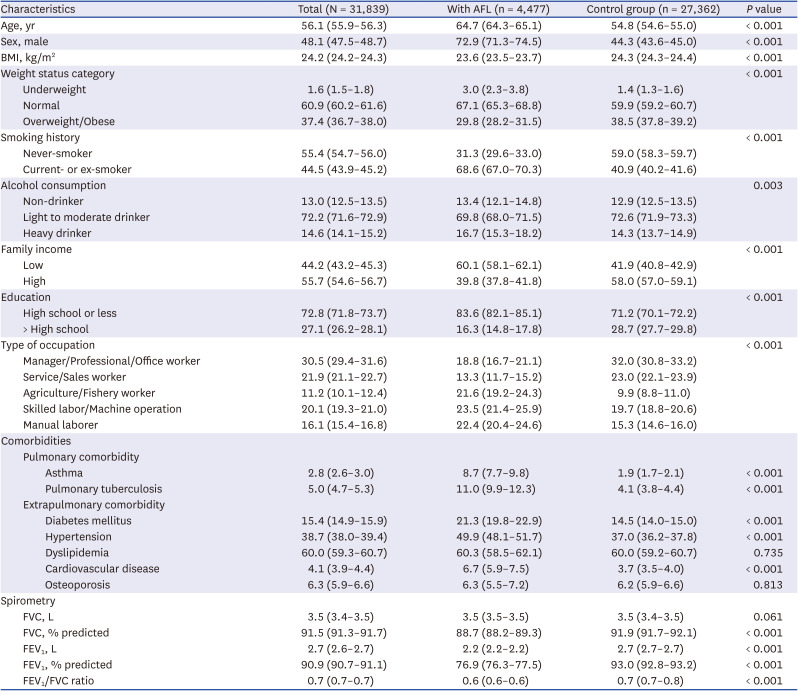
The characteristics of the study population were summarized in Table 1. Of the 31,839 participants, approximately 14% (n = 4,477) had AFL (AFL group), while 86% (n = 27,362) did not (control group). Compared with the control group, the AFL group had a higher mean age (64.7 years vs. 54.8 years), a higher proportion of male participants (72.9% vs. 44.3%), a lower BMI (23.6 kg/m2 vs. 24.3 kg/m2), a higher proportion of smokers (68.6% vs. 40.9%), and a higher proportion of heavy drinkers (16.7% vs. 14.3%; P < 0.05 for all variables). Regarding socioeconomic characteristics, the AFL group had lower family income and a lower level of education than the control group (P < 0.001 for all variables). In addition, the proportion of participants working as service/sales workers was lower in the AFL group, while the proportion of participants working as skilled labor/machine operators was higher (P < 0.001). Regarding comorbidities, the AFL group had a higher proportion of asthma (8.7% vs. 1.9%), pulmonary tuberculosis (11.0% vs. 4.1%), DM (21.3% vs. 14.5%), hypertension (49.9% vs. 37.0%), and cardiovascular disease (6.7% vs. 3.7%) than the control group (P < 0.05).
Table 1
Characteristics of the study population
Comparison of oral health between the AFL and control groups
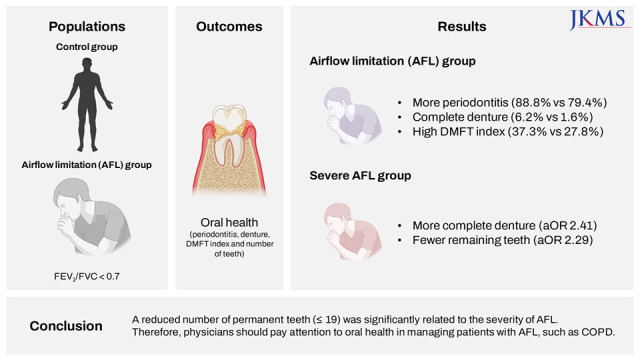
The comparison of oral health between the AFL and control groups is summarized in Table 2. Compared with the control group, the AFL group had a lower frequency of tooth brushing (62.4% vs. 52.9%, ≤ 2 times per day) but a higher proportion of periodontitis (88.8% vs. 79.4%), complete dentures (6.2% vs. 1.6%), and high DMFT index (37.3% vs. 27.8%; P < 0.001 for all variables). The number of permanent teeth was significantly lower in the AFL group than in the control group (15.2% vs. 35.5% in 28 permanent teeth; P < 0.001). However, the frequency of dental visits in the previous year did not differ between the two groups.
Table 2
Comparison of oral health between the AFL and control groups
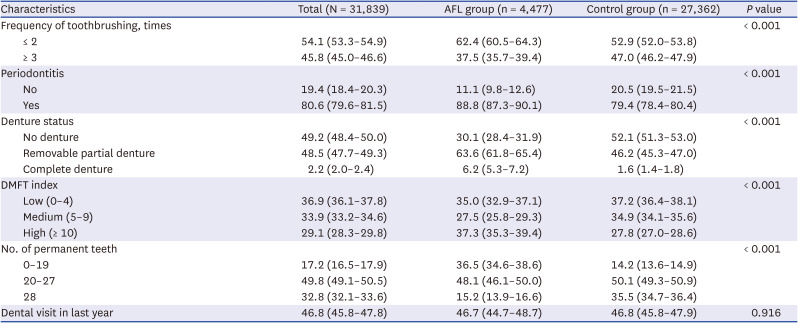
Data are presented as weighted mean (95% confidence interval) or weighted percentage (95% confidence interval). AFL was defined as pre-bronchodilator forced expiratory volume in 1 second/forced vital capacity < 0.7. Periodontitis: the World Health Organization CPI was used to assess periodontitis and when CPI code ≥ 3.
AFL = airflow limitation, DMFT = decayed, missing, and filled teeth, CPI = community periodontal index.
Association of oral health status with AFL severity
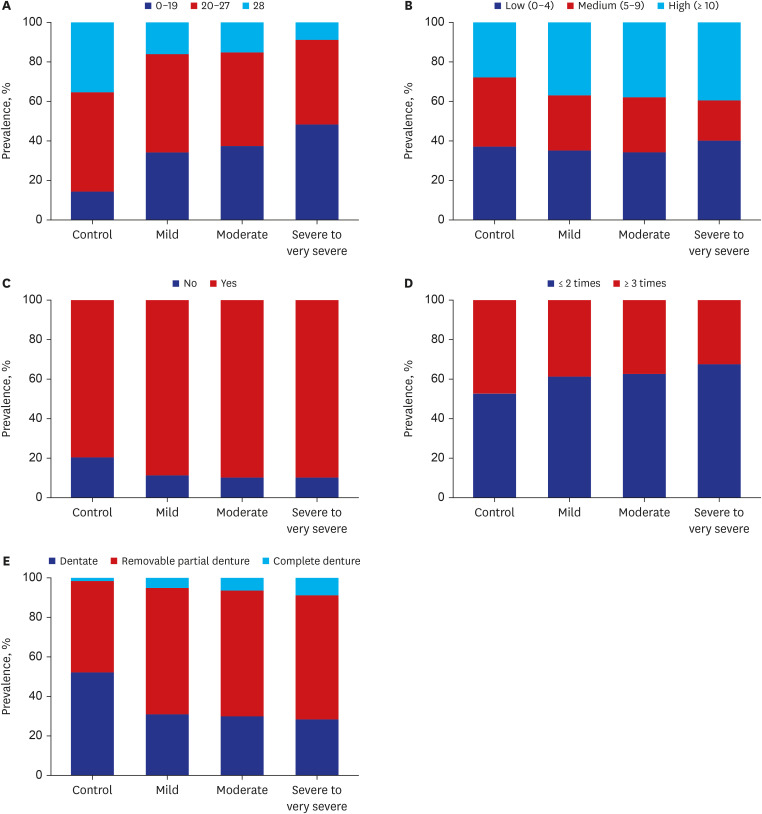
The distribution of oral health according to the severity of AFL is shown in Fig. 2. As the severity of AFL increased, the number of permanent teeth decreased (P for trend < 0.001), whereas the proportions of high DMFT index and complete dentures increased (P for trend < 0.001). In contrast, there was no significant difference in the frequency of tooth brushing, or the prevalence of periodontitis based on the severity of AFL.
Fig. 2
Distribution of dental status in subjects with AFL according to the severity. (A) Natural teeth. (B) DMFT index. (C) Periodontitis. (D) Frequency of toothbrushing. (E) Denture Status. AFL was defined as pre-bronchodilator forced expiratory volume in 1 second/forced vital capacity < 0.7. Periodontitis: the World Health Organization CPI was used to assess periodontitis and when CPI code ≥ 3.
AFL = airflow limitation, DMFT = decayed, missing, and filled teeth, CPI = community periodontal index.
In multivariable analyses, denture status: removable partial denture (aOR, 1.12; 95% CI, 1.04–1.20), complete denture (aOR, 1.52; 95% CI, 1.01–2.05), high DMFT index (aOR, 1.13; 95% CI, 1.02–1.24), and lower number of existing permanent teeth (0–19; aOR, 1.32; 95% CI, 1.12–1.52) were factors significantly associated with AFL.
Compared to the control group, the severe to very severe AFL group had a significantly higher proportion of complete dentures (aOR, 2.41; 95% CI, 1.11–3.71) and a lower number of permanent teeth (0–19; aOR, 2.29; 95% CI, 1.57–3.01). The moderate AFL group was more likely to have periodontitis (aOR, 1.03; 95% CI, 1.01–1.06), complete dentures (aOR, 1.81; 95% CI, 1.30–2.31), high DMFT index (≥ 10; aOR, 1.20; 95% CI, 1.10–1.30), and a lower number of permanent teeth (0–19; aOR, 1.54; 95% CI, 1.35–1.73) compared to the control group (Table 3).
Table 3
Adjusted odds ratios and 95% confidence intervals for oral health status by the severity of AFL
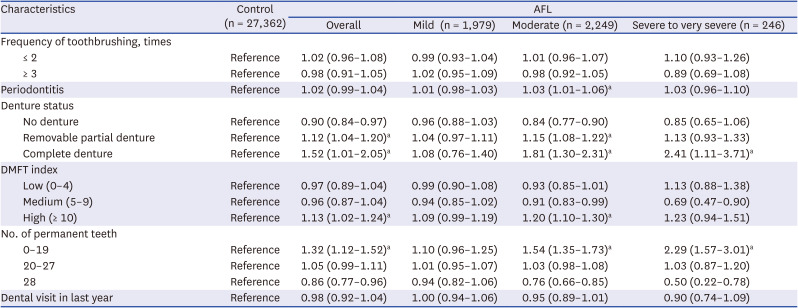
Adjusted for age, sex, body mass index group (underweight, normal, overweight or obese), smoking status (never, current or ex), and comorbidities (asthma, pulmonary tuberculosis, diabetes mellitus, hypertension, dyslipidemia, cardiovascular disease, osteoporosis, osteoarthritis or rheumatoid arthritis, depression). AFL was defined as pre-bronchodilator forced expiratory volume in 1 second/forced vital capacity < 0.7. The forced expiratory volume in 1 second (% predicted) value of 3 participants was missing. Periodontitis: the World Health Organization CPI was used to assess periodontitis and when CPI code ≥ 3.
AFL = airflow limitation, DMFT = decayed, missing, and filled teeth, CPI = community periodontal index.
aStatistically significant values are indicated.
Association of oral health status with respiratory symptoms in the AFL group
Table 4 shows the association between oral health and respiratory symptoms in the AFL group. The AFL group with high DMFT index (≥ 10) were significantly associated with physical activity limitation (aOR, 1.42; 95% CI, 1.15–1.69), and those with fewer permanent teeth (0–19) were associated with dyspnea (aOR, 1.59; 95% CI, 1.05–2.14) and physical activity limitation (aOR, 1.27; 95% CI, 1.03–1.51).
Table 4
Adjusted odds ratios and 95% confidence intervals for oral health status by respiratory symptoms in participants with AFL
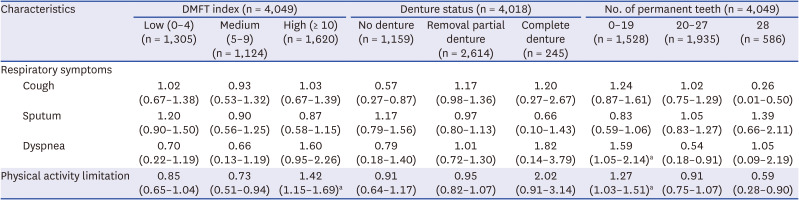
Adjusted for age, sex, body mass index group (underweight, normal, overweight or obese), smoking status (never, current or ex), and comorbidities (asthma, pulmonary tuberculosis, diabetes mellitus, hypertension, dyslipidemia, cardiovascular disease, osteoporosis, osteoarthritis or rheumatoid arthritis, depression). AFL was defined as pre-bronchodilator forced expiratory volume in 1 second/forced vital capacity < 0.7.
AFL = airflow limitation, DMFT = decayed, missing, and filled teeth.
aStatistically significant values are indicated.
DISCUSSION
Using nationally representative data in Korea, the present study showed the association between oral health and AFL. Our study showed that denture status, high DMFT index, and decreased number of permanent teeth were factors significantly associated with AFL. Furthermore, high DMFT index and decreased number of permanent teeth (0–19) were significantly associated with the severity of AFL.
The association between oral health and COPD has been investigated in recent decades. Most previous studies have focused on one or two indicators, such as periodontitis or the number of permanent teeth.911213334 Additionally, Gaeckle and colleagues35 recently showed that compared with healthy controls, participants with COPD had fewer teeth, a trend of a higher plaque index, and worse oral health-related quality of life. However, the study was limited by its small sample size. In contrast, using a nationwide survey, oral health was comprehensively evaluated using various indicators such as periodontitis, denture wearing, DMFT index, and number of permanent teeth. In addition, independent factors associated with AFL were investigated by adjusting for several factors. As a result, denture status, high DMFT index, and decreased number of permanent teeth were factors associated with AFL.
Our study shows that the AFL group had a higher proportion of complete dentures, a higher DMFT index, and a decreased number of existing permanent teeth (0–19) than the control group. A prospective observational study also reported that the COPD group had poor oral hygiene and fewer teeth than the healthy control participants.35 Changes in oral health status due to dental caries and periodontitis lead to a decreased number of existing permanent teeth.9 The decreased number of existing permanent teeth as a result of dental caries and periodontal disease is a representative indicator of oral health and has significant clinical implications. In general, it is assumed that people wear dentures because of a small number of existing permanent teeth. The biofilm formed on the denture can provide shelter for bacteria, yeast, and mold. It is said to have a structure similar to that of natural teeth, and the type and number of microorganisms it contains are complex.36 Therefore, it was thought that the risk of COPD may increase in people who have lost more teeth due to denture-related accumulation of biofilm.
Interestingly, our study showed that a high DMFT index and a decreased number of permanent teeth (0–19) were significantly associated with the severity of AFL. To our knowledge, this is the first study to show an oral health factor associated with AFL severity. The reason may be that the more advanced the AFL, the more severe the breathing difficulties and fatigue, making it difficult to perform daily activities.37 This is thought to deteriorate the ability to perform oral hygiene, resulting in the loss of permanent teeth and exacerbation of dental and periodontal diseases. In addition, participants with AFL who had a high DMFT index were associated with physical activity limitation, and those with decreased teeth (0–19) were associated with physical activity limitation as well as dyspnea. Although this phenomenon is not fully explainable, subjects with poor oral health may have poor oral intake, which can lead to poor nutrition and increased fatigue.38 Thus, these nutritional changes and increased fatigue might be a plausible explanation for physical activity limitation and dyspnea symptom in subjects with AFL who have poor oral health.
The present study results have several important clinical implications. First, the AFL group showed a higher DMFT index, more extensive denture use, and a decreased number of permanent teeth than the control group. Dental caries is one of the main causes of tooth loss. As tooth loss progresses, the use of dentures increases. Aerobic and anaerobic microorganisms have been identified in the dentures. These pathogenic microorganisms are thought to affect dental health and cause greater tooth loss.14 In addition, aspiration of these microorganisms is believed to contribute to respiratory infection and COPD exacerbation. Therefore, clinicians must regularly assess the oral health of patients with COPD. Another important finding was that a decreased number of permanent teeth (0–19) was significantly associated with the severity of AFL. This is because the greater the number of teeth lost, the more difficult mastication becomes, which can lead to malnutrition. In addition, the more advanced the AFL, the more severe the breathing difficulties and fatigue, making it difficult to perform daily activities.37 This effect is believed to deteriorate the ability to perform oral hygiene, resulting in the loss of permanent teeth and exacerbation of dental and periodontal diseases. Thus, for COPD patients, the number of permanent teeth should be assessed, and the clinician should ensure that adequate nutrition is provided.
Despite these clinical implications, our study has several limitations. First, it was performed using a representative sample from Korea. Therefore, our data may not be generalizable to other ethnic groups or populations. Second, the AFL group was defined based on pre-bronchodilator spirometric results, not by post-bronchodilator spirometry. Thus, the proportion of COPD in our study population could not be well evaluated. Although the KNHANES have a questionnaire about the presence of physician-diagnosed COPD, the physician-diagnosed COPD is known to be very low in Korea.39 Thus, previous studies evaluated the prevalence of COPD using pre-bronchodilator AFL.43940 The actual prevalence of COPD seems to be between those two values; however, it is thought to be closer to the prevalence of AFL. Third, although we calculated the odds of AFL and AFL severity according to dental health status, a cause–effect relationship could not be determined due to the limitation of our cross-sectional study design. Thus, future studies are needed for this issue. Finally, this study included healthy participants with mild airflow obstruction rather than those with severe airflow obstruction. KNHANES data were obtained from participants in a nationwide survey; individuals admitted to hospitals or nursing homes were not included. Within these limitations, the KNHANES data represent the public health of the total population of Korea and are of considerable value in many respects.41
In conclusion, our study showed that denture status, high DMFT index, and decreased number of permanent teeth were factors significantly associated with AFL. Furthermore, a reduced number of permanent teeth (0–19) was significantly related to the severity of AFL. Therefore, physicians should pay attention to oral health in managing patients with AFL, such as COPD.
 XML Download
XML Download