

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Renal infarction (RI), caused by the main renal artery or segmental branch occlusion, can lead to hypertension (HTN) and permanent kidney dysfunction if proper management is not conducted in an instant.123 However, nonspecific symptoms of RI can result in delayed diagnosis and treatment,4 and it is practically common to detect RI incidentally while evaluating patients who were suspected to have other diseases. RI usually develops when patients have underlying diseases that increase thromboembolic risk or renovascular disease. Especially, with the rapid aging of the population, the number of Korean adults with circulatory diseases and risk factors such as HTN, diabetes mellitus (DM), and dyslipidemia is continuing to increase in Korea.56 Since the first case study published in 1978 reported 17 RI patients based on clinical diagnosis and autopsies for 14 years,4 there have been occasional case studies from various nations and races.278910 Because of its rare incidence, most studies about RI are retrospective case studies with small sample size. Therefore, the incidence and prevalence of RI are not clearly identified, and the comorbidity characteristics cannot be recognized. Identifying the epidemiologic trend can help determine which patient to suspect and prevent misses or delays in diagnosis. Also, the absence of definite guidelines about RI treatment is a significant reason for large-scale studies. The result of the treatment trend research may serve as a basis for comparative studies on outcomes according to therapeutic strategies. In this background, we aimed to investigate the epidemiologic trend and characteristics of RI on a nationwide scale using the National Health Insurance Service (NHIS) claims database in South Korea.
METHODS
Data source and study population
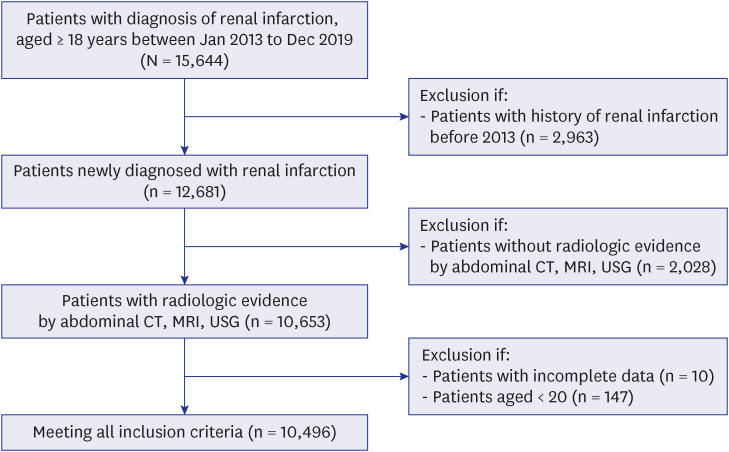
This nationwide population-based retrospective cohort study obtained health-related information about demographics, diagnosis, and prescription from the NHIS claims database, which covers the entire Korean population.11 Study population was selected among Koreans aged 18 years old and above from January 1, 2013 to 31, 2019. Individuals with incomplete data and age under 20 years were excluded. RI patients were defined as individuals with the International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) code corresponding to RI (N28.0), regardless of whether they are the primary or secondary diagnosis. Afterwards, we selected only patients who had records of radiological examination including abdominopelvic computer tomography, magnetic resonance imaging, or ultrasonography (Fig. 1).
Assessment of comorbidity
Comorbidities were defined as a confirmed primary or secondary diagnosis at the time of hospitalization or at least two outpatient clinic visits, within 1 year preceding the RI diagnosis.
We analyzed traditional risk factors for cardiovascular disease and thromboembolism related diseases which included HTN, dyslipidemia, DM, myocardial infarction (MI), ischemic heart disease (IHD), atrial fibrillation (AF), ischemic stroke, transient ischemic attack, arterial thromboembolism, peripheral arterial disease (PAD), heart failure, deep vein thrombosis and pulmonary embolism.
Subsequently, we assessed the risk factor distribution by grouping comorbidities according to etiologic mechanism. Based on several previous retrospective case studies that attempted to analyze the etiology of RI,121314 we categorized the mechanism of RI as embolism, renovascular disease, hypercoagulable state. The number of patients with at least one disease belonging to the group was counted and overlapping cases were excluded. Diseases included as risk factors for each mechanism are indicated below. The ICD-10-CM codes for the diseases were attached in the Supplementary Table 1.
I. High embolic risk group: AF, patent foramen ovale, status post (s/p) radio frequency ablation, s/p prosthetic valve implantation, previous embolic event (cerebral infarction due to embolism,15 arterial thromboembolism, mesenteric occlusion).
II. Renovascular disease group: renal artery atherosclerosis, fibromuscular dysplasia, renal artery aneurysm, aortic dissection, renal artery dissection, trauma, atherosclerotic disease (MI, IHD, PAD, cerebral infarction due to thrombosis, stenosis or occlusion,15 carotid atherosclerosis, general atherosclerosis, s/p percutaneous coronary intervention, s/p coronary artery bypass graft).
Assessment of medication
To sort the antithrombotic agent, we used the main ingredient codes of medicine. We investigated the prescription history of oral antiplatelet and anticoagulation agents, which was reported before and after the index time of RI diagnosis. Medication taken before the diagnosis of RI was defined as two or more prescriptions within the 6 months preceding the diagnosis, while medication prescribed after the diagnosis of RI was defined as one or more instances within the 3 months following the diagnosis. Included drugs were aspirin, clopidogrel, warfarin, and non-vitamin K antagonist oral anticoagulant (NOAC). Aspirin and clopidogrel were grouped as antiplatelet agents, and warfarin and NOAC were combined as anticoagulation agents.
Statistical analyses
Continuous variables were presented as means with standard deviation or as median-valued with interquartile range. Categorical variables were expressed as percentages. To compare the trend of demographic characteristics, we conducted an independent t-test for continuous variables and a χ2 test for categorical variables. The incidence and prevalence of RI was estimated annually. The incidence was calculated as the number of patients newly diagnosed with RI divided by the total person-years (PY) at risk of individuals who had not previously been diagnosed with RI, for each year. Incidence was presented as per 100,000 PY. The annual prevalence was calculated as the number of patients with RI divided by the total population of each year. Prevalence was presented as a percentage. In-hospital mortality was defined as death that occurred during the hospitalization period that included the index diagnosis of RI. Analytic programs used in this study were SPSS 25, R (version 3.6.0; IBM Corp., Armonk, NY, USA), and SAS 9.4 (SAS Institute, Cary, NC, USA).
Ethics statement
The study was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital (SCHBC 2021-02-019) and was conformed to the ethical guidelines of the Declaration of Helsinki. No informed consent was required from patients due to the nature of public data from NHIS.
RESULTS
The incidence and prevalence, in-hospital mortality of RI
During the 7-year period, 10,496 patients were newly diagnosed with RI (overall incidence, 2.91 per 100,000 PY). Table 1 indicates the demographic characteristics of the RI incidence cohort. From year 2013 to 2019, the incidence of RI per 100,000 PY increased from 2.68 to 3.06 (P < 0.001). The annual RI incidences gradually increased in both genders (Fig. 2). The proportion of male patients was greater for the whole study period, and the incidence rate was generally 1.41 times higher than that of females. The median age of overall RI patients increased from 60 to 62. Divided by the patients’ gender, the median age of male patients increased from 55 to 57, while the median age of female patients increased from 68 to 70.
Table 1
Demographic characteristics of the renal infarction patients
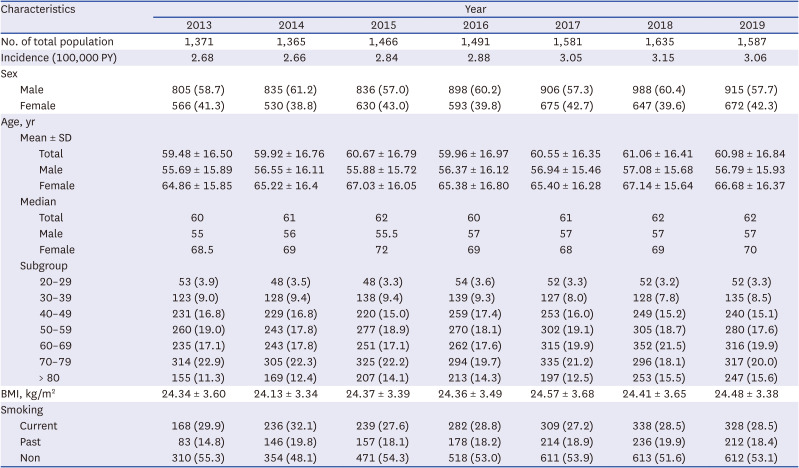
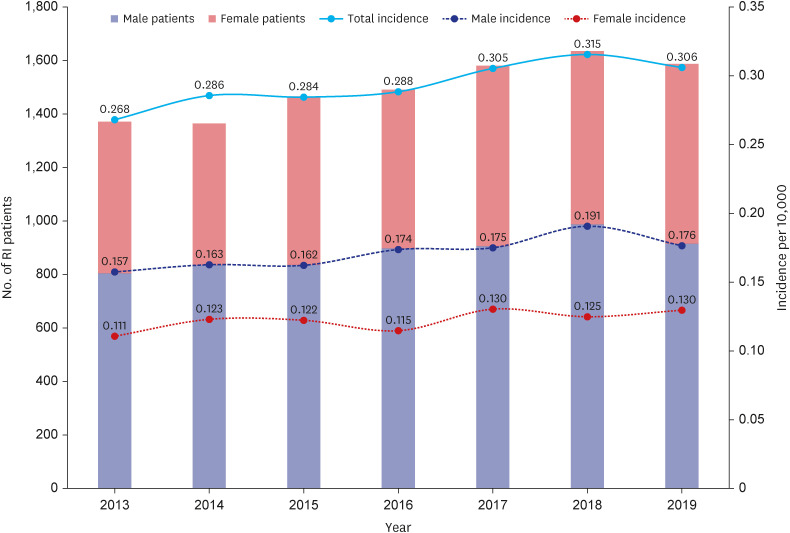
Fig. 3 shows the trend of RI incidence according to the age group. The incidence rate of RI increased with patient’s advancing age and peaked in the 70s. Although the proportion of patients aged in the 80s was not prominent in the initial study phase, a noticeable increase in the incidence rate was observed during the study period from 11.3% to 15.6% (n = 92, P < 0.001). The incidence rate of young patients under 40 hardly changed.
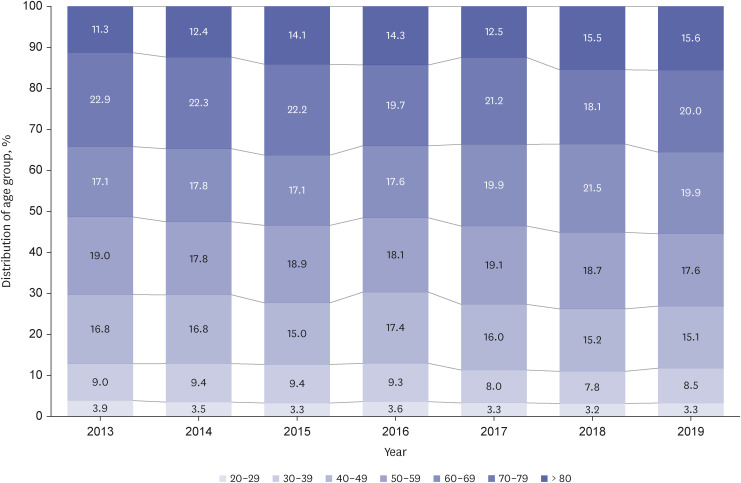
In the aspect of prevalence, RI increased by 1.7-fold from 0.007% to 0.012% (P < 0.001) (Supplementary Table 2). Likewise in the incidence graph, the prevalence of RI linearly increased in both genders during the study period with male predominance. Patients between 50 to 70 had the highest prevalence accounting for more than 60% of all the patients. An obvious increasing trend was observed in those aged > 80 (1.45-fold, P < 0.001) and 60–69 (1.17-fold, P < 0.001).
The in-hospital mortality of patients with RI ranged from 5.4% to 7.3%, and the average during the study period was 6.0% (Supplementary Table 3).
Comorbidities in RI patients
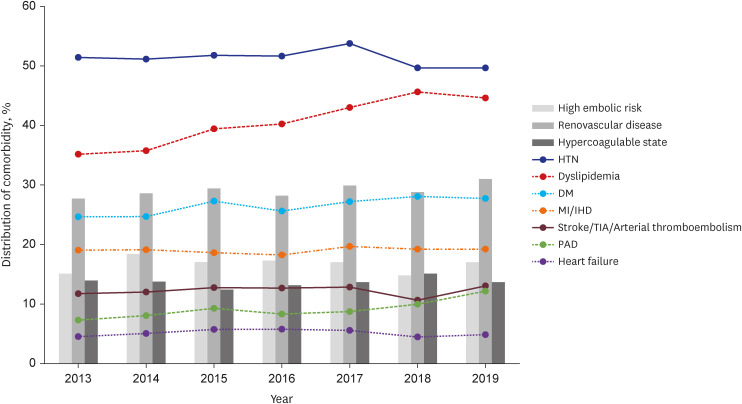
The most common comorbidity of patients with newly diagnosed RI during the study period was HTN (51.3%), followed by dyslipidemia (40.8%) and DM (26.6%) (Table 2, Fig. 4). Dyslipidemia steeply increased between study periods from 35.2% (n = 482) in 2013 to 44.6% (n = 708) in 2019. AF and PAD also showed a slight increase. Regarding etiologic mechanisms, the high embolic risk group, renovascular disease group, and hypercoagulable state group, accounted for 16.6%, 29.1%, and 13.7% on average respectively. When we analyzed for each subgroup, AF was the most frequent single disease (89.6%) in the high embolic risk group, while atherosclerotic disease accounted for the majority (95.0%) of the renovascular disease group. In the hypercoagulable state group, cancer was the most common factor (73.9%).
Table 2
Prevalence of comorbidities in the renal infarction patients
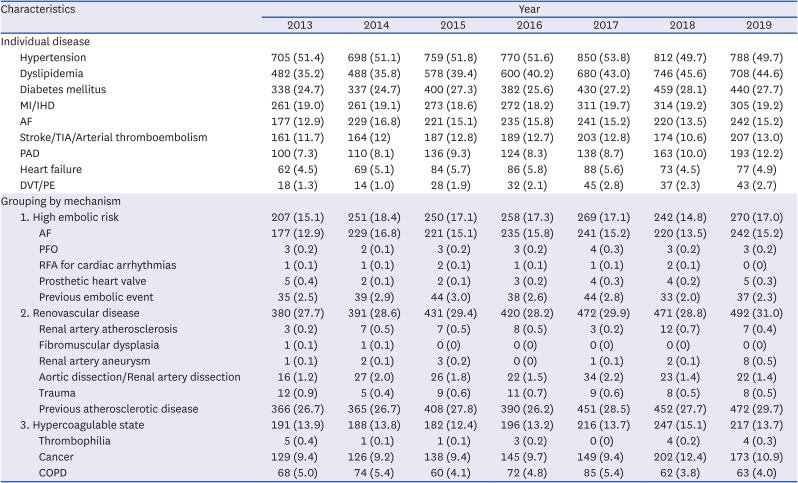
Values are presented as number (%).
AF = atrial fibrillation, COPD = chronic obstructive pulmonary disease, DVT = deep vein thrombosis, IHD = ischemic heart disease, MI = myocardial infarction, PAD = peripheral arterial disease, PE = pulmonary embolism, PFO = patent foramen ovale, RFA = radiofrequency ablation, TIA = transient ischemic attack.
Fig. 4
Distribution of comorbidity and etiology of renal infarction.
HTN = hypertension, DM = diabetes mellitus, MI = myocardial infarction, IHD = ischemic heart disease, TIA = transient ischemic attack, PAD = peripheral arterial disease.
In addition, we evaluated the in-hospital mortality rate according to the etiologic risk subgroup. The subgroup with the highest in-hospital mortality was the hypercoagulable state group (12.8%) followed by the high embolic risk group (8.4%) and renovascular disease group (8.0%) (Supplementary Table 3).
Antiplatelet and anticoagulation agents in RI patients
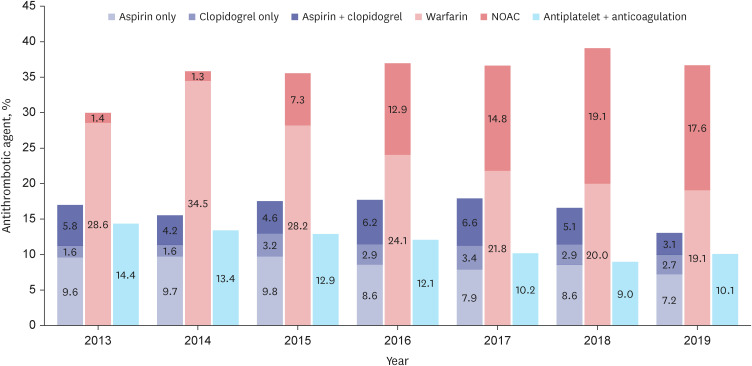
In terms of antithrombotic therapy, the prescription rate of antiplatelet agents showed a continuous decrease from 17.0% in 2013 to 13.0% in 2019. Among the group, aspirin monotherapy was the most common at an average of 53.0%, while clopidogrel monotherapy and aspirin plus clopidogrel combination therapy were 16.0% and 30.9%, respectively. The prescription rate of anticoagulation agents remained around 35% annually, and while warfarin prescription decreased from 34.5% in 2014 to 19.1% in 2019, NOAC prescription increased from 1.3% to 17.6% during the same period. The proportion of patients receiving both antiplatelet and anticoagulation agents decreased from 14.4% in 2013 to 10.1% (Fig. 5, Supplementary Table 4).
Fig. 5
Temporal trend of oral antithrombotic therapy of renal infarction.
NOAC = non-vitamin K antagonist oral anticoagulant.
When we investigated RI patients without any history of antithrombotic therapy, the proportion of patients who were prescribed antiplatelet and anticoagulation agents as their first medication for RI was about 8.4% and 25.4% on average, retrospectively. The 5.9% of the patient population received both antiplatelet and anticoagulation agent.
Among the patients who had been taking oral antiplatelet agent before the diagnosis of RI, 36.2% kept only antiplatelet agent after the diagnosis of RI and the number of adding or changing anticoagulation agents accounted for 39.7% on average. However, in the anticoagulation agent taking group, 55.7% were held on the existing medication, and the proportions of patients who were changed to antiplatelet agents or received extra antiplatelet agents were both less than 10%.
Also, the distribution of medical treatment showed differences according to the etiologic risk subgroup. In the high embolic risk group, the proportion of patients who received only anticoagulation agent prescriptions was significantly higher at an average of 52.5% compared to those who received only antiplatelet agent prescriptions (17.2%) and those who received both antiplatelet and anticoagulation agent prescriptions (20.7%). Meanwhile, in the renovascular disease group, the proportion of patients who received only antiplatelet agent prescriptions was higher at an average of 24.5% compared to the other two subgroups. In the hypercoagulable state group, a higher proportion of patients (28.3%) received only anticoagulation agent prescriptions compared to those who received only antiplatelet agent prescriptions (16.8%).
DISCUSSION
There has been a limited number of large scaled real-world studies reporting on the incidence and prevalence of RI. This study is the first research about the epidemiologic trend of RI on a nationwide scale based on the NHIS claims database.
The incidence rate of RI in Korean population showed an increasing trend from 2.68 to 3.06 per 100,000 PY with 1.41 of male-to-female ratio. Earlier studies from Taiwan and Austria, which were conducted on patients who visited the emergency department, reported a slightly higher incidence rate of RI as 4.15 to 6.83 per 100,000 PY.2021 The male-to-female ratio of RI patients differed from the earlier review studies. Antopolsky et al.7 reported that females comprised 55% of the entire group, and Weber et al.22 identified that only 24% were male in a total of 34 patients. However, we observed that the incidence of RI was higher in male patients, with a male-to-female ratio of about 6:4. Also, the mean age of male patients was approximately ten years younger than that of female patients at the time of RI diagnosis. According to the age subgroup, the largest proportion was in their 70s and a gradually increasing trend was observed in patients whose ages are in their 80s. As the aging of the patients progresses, it seems that more elderly patients would be diagnosed with RI.
The average in-hospital mortality of RI patients in this study was 6.0%, which is slightly higher than a previous study that reported an in-hospital mortality of 5.0%.14 Various factors including severity of the blockage, underlying cause of the condition and general status of patients may contribute to the mortality of RI patients, but further research is needed to understand factors more thoroughly.
The most common comorbidity of RI patients was HTN, followed by dyslipidemia and DM. Considering that these three diseases are the representative risk factors of atherosclerosis, which appeared to be an important etiologic mechanism of RI according to the current study, it implies the importance of suspecting the disease in the patients with these clinical histories. On the other hand, we found a relatively low prevalence of AF (14.9%) compared with the previous reports.2021 Many case studies report AF as the most common comorbidity of RI patients, although the figure can be various.27810 It may suggest the necessity of meticulous evaluation to reveal hidden AF.
When we assessed etiologic risk subgroup analysis, not only diseases that could cause RI, but also diseases that share similar mechanisms were included in each subgroup. For example, even if atherosclerosis was confirmed in areas other than the renal artery, the cases were included in renovascular group considering that atherosclerosis affects blood vessels throughout the body and eventually can cause stenosis of the renal artery. As a result, among the renovascular disease group, patients with atherosclerotic disease mainly contributed the majority of the subgroup’s proportion (95.0%). In the high embolic risk group, AF, which is considered one of the main causes of RI, accounted for the highest proportion (89.6%). The proportion of the hypercoagulable state group were mainly attributable to the cancer (73.9%) and COPD (33.7%) patients. They also may have contributed to the high mortality rate in this group (12.8%).
Regarding the treatment of RI, we could identify that the number of patients who received antiplatelet agents gradually decreased whereas the prescription of anticoagulation agents has maintained a similar trend. In the anticoagulation therapy group, the use of NOAC has increased following its approval instead of warfarin. For the medical treatment of RI patients who are considered unlikely to benefit from surgical or interventional revascularization, antithrombotic therapy is conducted. The antithrombotic treatment option of RI is determined according to the grade of infarction, suspected occurrence time, and prognosis.232425 If a patient is suspected to have suffered from remote RI based on clinical and radiologic findings such as atrophic kidney, and if no indication of anticoagulation is found after systemic evaluation, antiplatelet agents could be prescribed. In contrast, anticoagulation therapy should be started when acute or subacute infarctions are suspected based on systemic evaluation or when patients have underlying diseases that raise the embolic risk.1226 We were able to confirm such a trend in this study as well, where it was found that in the high embolic risk group, 73.2% of patients were prescribed anticoagulation agents either alone or in combination with antiplatelet agents. However, since there are no specific criteria to determine treatment methods, it would be helpful to treat RI patients if therapeutic guidelines were established through follow-up studies on outcomes.
On the other hand, patients without any documented oral antiplatelet and anticoagulation agent are considered to have had a high risk of bleeding and were therefore unable to receive antithrombotic therapy. Furthermore, some might have received only intravenous heparin or other treatment including surgery and intervention.
There were several limitations on the current study. First, the fact that the current study is based on the NHIS claims database might lead to an underestimation of the results. While NHIS claims databases rely on precise coding of diagnoses and procedures, there may be inaccuracies in coding that can lead to underestimation of the actual prevalence. Regarding medication prescriptions, cases of uninsured medical benefits which are not reported in the NHIS claims database system were not available for analysis. Second, the statistical method of this study based on diagnostic code could only identify comorbidities in individuals and could not determine the specific cause of RI for individual patients. Therefore, we aimed to examine the distribution of the risk factors correlated with each etiologic mechanism in RI patients. Also, there may be selection bias in the process of assessing the distribution of etiologic risk subgroups. Finally, investigation about the treatment of RI was limited to oral antithrombotic agents only, because it was not possible to collect data on surgical or interventional treatment, as well as the use of intravenous heparin or thrombolytic agents.
In this study, we could provide a comprehensive epidemiologic description of RI in Korea. Considering the progressively increasing incidence of RI and high prevalence of coexisting risk factors, constant efforts are necessary to raise awareness of the disease while avoiding misdiagnosis. This nationwide scale investigation of epidemiologic trend regarding RI would be the stepping-stone to establishing future studies about clinical outcomes and consequential optimal treatment strategies.
 XML Download
XML Download