

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lung cancer is a major cause of psychological distress among patients with cancer. Higher psychological distress is associated with psychosocial problems, physical symptoms, and emotional difficulties.1 The overall prevalence of distress in patients with lung cancer exceeded that of other types of cancer, ranging from 43.4% to up to 58%.23 This relatively higher rate results from a poorer prognosis and greater burden of the disease itself,24 and the distress was associated with a poorer quality of life,5 which implies relevant clinical attention is required. Furthermore, among patients with the most prevalent cancers in South Korea, those with lung cancer showed a significantly higher probability of experiencing symptoms of psychological distress such as depression6 and insomnia7 compared with patients with other types of cancer. These findings are similar to prior results suggesting that depression was most frequently observed in patients with lung cancer, although a lack of appropriate treatment was reported.8 Similarly, sleep disturbance was most commonly found in those who visited a lung cancer clinic.9
Fear of progression (FoP) is one of the most common psychological symptoms in cancer patients. Its prevalence was reported to be approximately 50% in several samples of patients with cancer.101112 For patients with physical illness, fears related to their disease are considered normal psychological reactions; these fears are referred to as FoP.13 Unlike other psychiatric symptoms, FoP is reactive and appropriate, especially in the context of cancer. Nevertheless, exaggerated FoP can cause distress in cancer patients and is often associated with psychiatric disorders and poor quality of life.10
Previous research has suggested that several demographic and clinical factors are associated with FoP. For example, younger age, more physical symptoms, and chemotherapy were related to a higher level of FoP.1014 However, besides these variables, other demographic, clinical, and psychological variables indicate mixed results regarding the association with FoP.15 Although there is a lack of evidence that cancer type is significantly associated with FoP, patients with lung cancer are known to have a relatively higher level of FoP, considering the high prevalence of psychological distress and the poor prognosis of the disease itself. Indeed, fear of cancer progression was the most significant psychological distress among patients with non-small cell lung cancer (NSCLC) who had undergone surgically resection and their caregivers.16 In addition, considering that more than one-third of patients who undergo curative resection for early-stage NSCLC eventually develop recurrence and die,17 It is very important to evaluate FoP and psychological distress in these populations.
Insomnia occurs in about 30–50% of patients with cancer18 but is especially prevalent among patients with lung cancer.19 One systemic review of cancer-related sleep disorders showed that the prevalence of sleep disorders reached up to 95% in patients with lung cancer.20 Although insomnia has a negative impact on both physical and psychological function, only a few studies have investigated the link between insomnia and cancer. However, insomnia plays an important role in sustaining patients’ well-being.21 A Mendelian randomization study suggested that insomnia itself could be a risk factor for lung cancer in some ways,22 but it is not yet clear which precedes the other.
Patients with cancer who complain of insomnia show different characteristics compared to individuals experiencing insomnia in the general population. Cancer patients generally feel more nervous, anxious, and helpless, and they feel that they cannot control their cancer, which leads to anxiety.18 Various studies have shown that the worse anxiety is, the worse insomnia symptoms are in different cancer-diagnosed patients.23 Insomnia in cancer patients appears to have a stronger connection with anxious feelings, and anxiety leads to cognitive distortion24 that insomnia could result in immune dysfunction and cancer recurrence. In this context, cancer-related dysfunctional beliefs about sleep (C-DBS) develop, which can be used to predict insomnia severity with a high correlation.25 Intervention to correct these dysfunctional beliefs about sleep is as important as pharmacologic treatment of insomnia. Development and maintenance of insomnia are supported by dysfunctional cognitions, which is one of the key components of cognitive therapy of insomnia.26 Case-control and meta-analysis studies suggested that cognitive behavioral therapy for insomnia (CBT-I) is significantly effective.27 A previous study also showed that patients with lung cancer reported more dysfunctional beliefs about sleep and attitudes about beliefs.28 Determining how dysfunctional beliefs mediate and worsen insomnia in patients with lung cancer could be another key to their treatment.
This study aimed to determine whether insomnia or depression were significant predictors of FoP in patients with stage I or II NSCLC. Furthermore, we tested whether C-DBS may mediate the influence of depression or insomnia on their FoP. We hypothesized that (a) insomnia will be positively related to FoP, (b) depression will be positively related to FoP, and (c) dysfunctional beliefs related to cancer about sleep will mediate the relationship between insomnia or depression with FoP among patients with lung cancer.
METHODS
Participants and procedure
This study was a part of a single-center randomized controlled study evaluating the efficacy of digital healthcare applications for patients with surgically resected NSCLC.29 In the main study, 320 patients consented to participate and were enrolled between November 2020 and January 2022. Prior to discharge, 3 days after surgery for their lung cancer, patients were informed of the study and were enrolled. After baseline assessment in the wards, their physical or psychological symptoms and digital application usage were evaluated at outpatient clinics at 3, 6, and 12 months after baseline assessment. Each assessment was completed by a face-to-face interview and using paper-and-pencil self-rating scales. The inclusion criteria were as follows: 1) age 20 to 80 years; 2) with a pathological diagnosis of stage 0, I, and II primary NSCLC; 3) scheduled for curative resection, including wedge resection, segmentectomy, lobectomy, and bilobectomy; 4) no evidence of lymphatic or distant metastasis; and 5) provision of written informed consent. Patients who 1) had any evidence of metastasis; 2) had a previous history of segmentectomy or wedge resection for lung cancer; 3) were scheduled for pneumonectomy; 4) were scheduled for neoadjuvant or adjuvant chemotherapy or radiotherapy around the time of surgery; 5) were pregnant or breast-feeding; 6) had a history of diagnosis of other malignancies within 5 years; or 7) had a disability that would make exercise difficult were excluded.
In the current study, we extracted baseline assessment data of all 320 patients from the main study in April 2022 and analyzed it to explore the expected psychological variables of FoP. At baseline, the following patient information was collected: age, sex, smoking history, European Cooperative Oncology Group (ECOG) performance status, underlying disease, and results of pulmonary function test. In addition, information related to lung cancer, including pathological diagnosis and clinical and pathological stage, was collected. Finally, the responses to psychological symptom rating scales of patients were also gathered.
Measures
Short form of the Fear of Progression Questionnaire (FoP-Q-SF)
FoP-Q-SF is a shortened version of the original FoP-Q that was developed to measure FoP among chronically ill patients.30 The FoP-Q has previously been used in cancer31 and multiple sclerosis32. The shortened version (FoP-Q-SF) included 12 items33 of 43 items of the original scale and has been validated among patients with breast cancer with adequate reliability (Cronbach’s α = 0.87). In this study, we used the Korean version of the FoP-Q-SF,31 and the Cronbach’s alpha in this sample was 0.891.
Patient Health Questionnaire-9 items (PHQ-9)
The PHQ-9 is a self-reported rating scale widely used to assess the severity of depression.34 Nine elements of the PHQ-9 scale can be rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day), for a total score ranging from 0 to 27. A high score indicates a severe degree of depressive symptoms. In this study, we applied the Korean version of PHQ-9,35 and Cronbach’s alpha was 0.796 in this sample.
Insomnia Severity Scale (ISI)
The ISI is a self-report rating scale developed to assess insomnia severity.36 Seven items of the ISI scale can be rated on a 0–4 Likert scale, for a total score ranging from 0 to 28. A high total score indicates a high level of severity of insomnia. In this study, we applied the Korean version of the ISI37, and the Cronbach’s alpha was 0.874 in this sample.
C-DBS scale
C-DBS scale is a 2-item self-report rating scale developed to assess C-DBS.25 It includes two items: immune dysfunction (My immune system will have serious problems if I don’t go to sleep at a certain time) and cancer recurrence (If I don’t sleep well at night, my cancer may recur or metastasize). Each element is rated on a scale of 0–10, and a higher total score indicates that patients may have a high level of dysfunctional beliefs about sleep. In this study, we applied the original Korean version of the C-DBS, and the split-half coefficient was 0.807 in this sample.
Statistical analysis
The participant’s demographic characteristics and rating scale scores are summarized as mean ± standard deviation. Pearson’s correlation coefficients were examined to explore whether FoP of patients with lung cancer was significantly correlated with insomnia, depression, or C-DBS. A linear regression analysis with enter methods was conducted to explore which variables, among insomnia, depression, or C-DBS could predict the level of FoP among subjects. We included in the regression model clinical variables that patients directly know and may affect their FoP, such as gender (male vs. female) and smoking history (yes vs. no), as dummy variables. However, cancer stages or surgical procedures, which patients were not aware of exactly, were not included in the final model. Finally, the bootstrap method with 2000 resamples was implemented to explore whether dysfunctional beliefs related to cancer about sleep may mediate the influence of insomnia or depression on FoP. The level of statistical significance was defined as two-tailed at values of P < 0.05. SPSS version 21.0, AMOS version 27 for Windows (IBM Corp., Armonk, NY, USA) and Jamovi version 1.6.18.0 were used to perform the statistical analysis.
RESULTS
A total of 320 enrolled subjects who completed all psychological symptom rating scales were included for the statistical analysis. The mean age of the patients was 60.9 (SD = 8.6) years; 51.3% (n = 164) were women. Two hundred patients (86.6%) had more than one underlying medical comorbidity. Adenocarcinoma (290/320, 90.6%) was the most common type of NSCLC, and 90.6% of patients were in stage I. Among 320 patients, 241 (75.3%) underwent lobectomy or bilobectomy, while 79 (24.7%) received sublobar resection. The mean scores of the self-report questionnaires were as follows: FoP-Q-SF (36.5 ± 12.2), C-DBS (11.7 ± 6.0), ISI (15.5 ± 6.9), and PHQ-9 (11.4 ± 6.6) (Table 1).
Table 1
Demographic and clinical characteristics of the study participants (N = 320)
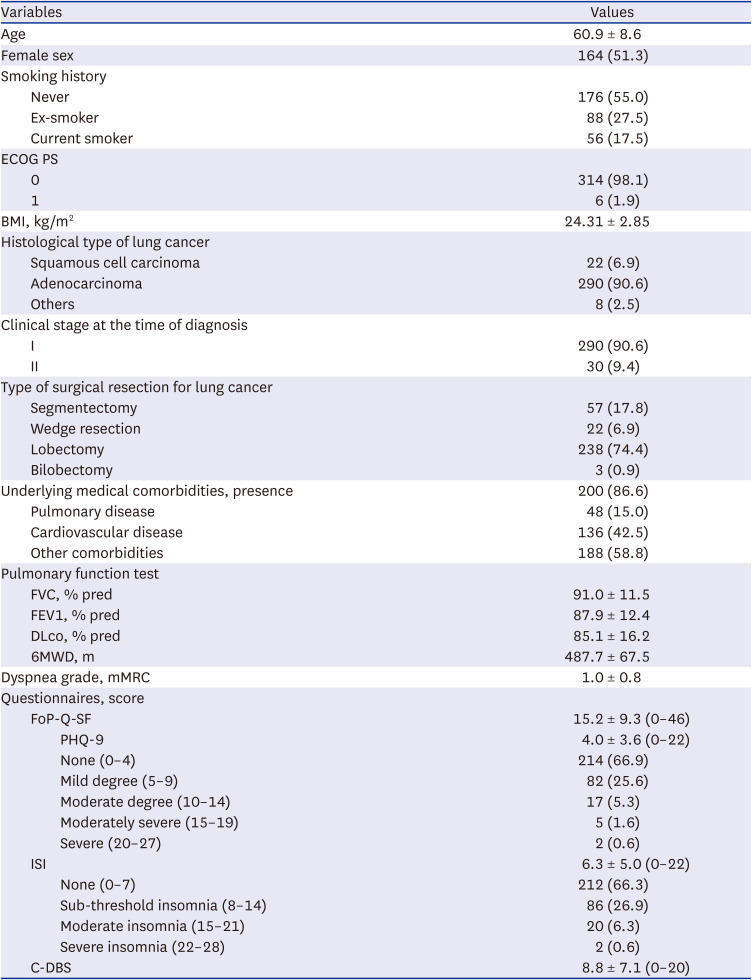
Values are presented as number (%) or mean ± standard deviation.
ECOG PS = eastern cooperative oncology group performance status, BMI = body mass index, FVC = forced vital capacity, FEV1 = forced expiratory volume in 1 second, Dlco = diffusion capacity, 6MWD = 6 minute walk distance, FoP-Q-SF = Fear of Progression Questionnaire-Short Form, PHQ-9 = Patient Health Questionnaire-9 items, ISI = insomnia severity index, C-DBS = cancer-related dysfunctional beliefs about sleep.
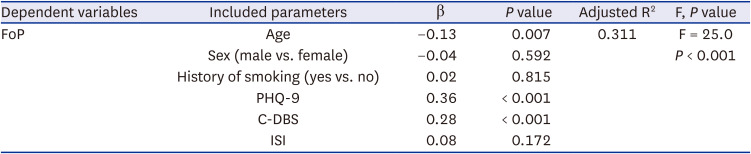
Table 2 shows that the age of the patients was significantly correlated with the FoP-Q-SF score (r = −0.15, P < 0.001), and the FoP-Q-SF score was significantly correlated with PHQ-9 (r = 0.47, P < 0.001), ISI (r = 0.54, P < 0.001), and the C-DBS score (r = 0.22, P < 0.001). We conducted a linear regression analysis with enter methods to explore which variables could predict FoP. We found that the FoP-Q-SF score was predicted by age (β = −0.13, P = 0.007), PHQ-9 (β = 0.35, P < 0.001), and C-DBS (β = 0.28, P < 0.001) (adjusted R2 = 0.32, F = 38.7, P < 0.001) (Table 3).
Table 2
Pearson’s correlation coefficients of each variable in all participants (N = 320)

| Variables | Age | FoP-Q-SF | PHQ-9 | ISI | C-DBS |
|---|---|---|---|---|---|
| Age | 1.000 | - | - | - | - |
| FoP-Q-SF | −0.15* | 1.000 | - | - | - |
| PHQ-9 | −0.04 | 0.47* | 1.000 | - | - |
| ISI | 0.01 | 0.35* | 0.54* | 1.000 | - |
| C-DBS | −0.05 | 0.39* | 0.22* | 0.31* | 1.000 |
Table 3
Linear regression analysis exploring predicting symptoms for fear of disease progression in patients with lung cancer (N = 320)
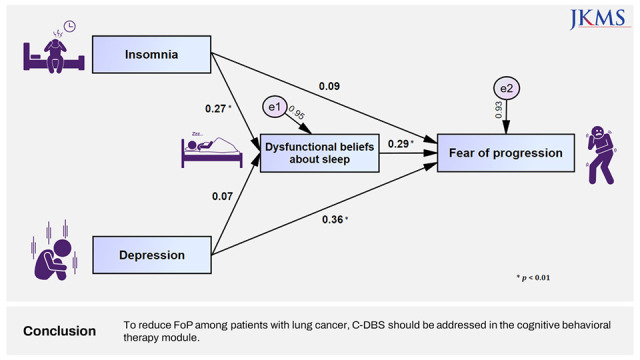
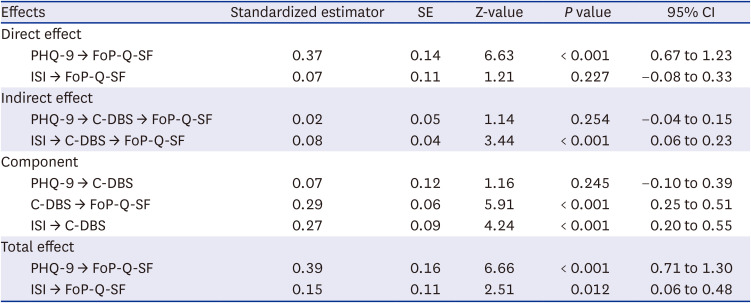
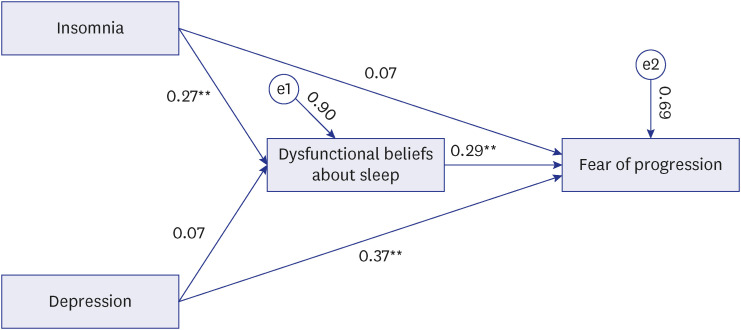
A mediation analysis showed that insomnia did not directly influence FoP, and C-DBS completely mediated this association. Conversely, depression was observed as it directly influenced the FoP in patients with lung cancer, but dysfunctional beliefs related to cancer did not mediate this association (Table 4, Fig. 1).
Table 4
Results of direct, indirect, and total effects on mediation analysis
DISCUSSION
In this study, we found that FoP in patients with surgically resected NSCLC was significantly related to insomnia severity and depression; however, only depression was found to be a significant predictor of FoP based on the linear regression model. Furthermore, according to the mediation model, the influence of insomnia severity on FoP was completely mediated by C-DBS, but the influence of depression on FoP was not mediated by C-DBS, despite the direct influence of depression on FoP in patients with lung cancer.
A positive correlation was found between ISI scores and FoP, indicating the association between insomnia and fear of cancer progression in patients with lung cancer. This finding is consistent with previous results, including from our previous studies, which suggest that FoP was significantly related to a higher risk of poor sleep quality in cancer patients.383940 Conversely, a pilot study reported that insomnia was related to intrusive thoughts rather than FoP in cancer survivors.41 This discrepancy may have occurred due to the difference in measurement scales and heterogeneity of clinical samples. However, the correlation coefficient was higher in our results (Pearson’s correlation coefficient = 0.54), suggesting that the association could be more prominent in patients with lung cancer. Furthermore, even in patients with early-stage lung cancer, more anxiety was found in those with comorbid insomnia than in those without sleep problems.28
Similarly, the PHQ-9 score was positively correlated with FoP, similar to our previous findings.3940 The association between depression and FoP remained after adjusting for all other variables in linear regression. This finding was consistent among patients with other types of cancer, including malignant melanoma,42 cervical cancer,43 and breast cancer.44
The 5-year survival rate of stage I NSCLC is 73–90%, even in patients who undergo surgical resection, and it decreases further to 56–65% at stage II.17 Considering the high recurrence rate and relatively low survival rate of early-stage NSCLC, FoP is prevalent even in early-stage cancer; this is unfortunately often neglected by their physicians. Clinicians should pay close attention to the importance of their patient’s distress during cancer treatment.
In the correlation analysis, we observed that the FoP of patients with lung cancer was associated with C-DBS. Previously, we reported that cancer patients experiencing sleep disturbances might have dysfunctional beliefs and that their sleep disturbance might impair their immune function or influence cancer recurrence. Based on medical knowledge, these dysfunctional beliefs about sleep are based on the belief that sleep disturbances can influence immune dysfunction, in which melatonin plays an important role. Furthermore, previous studies have shown that sleep deprivation disrupts the immune system and promotes cancer progression.4546 However, taking into account this medical knowledge, patients are concerned that sleep problems may be related to the progression of their disease. Thus, these beliefs are “dysfunctional” as they cause anxiety in cancer patients and, consequently, cause sleep problems.
According to our mediation analysis, the severity of insomnia did not directly influence FoP for lung cancer. However, dysfunctional beliefs about sleep mediated an association. This suggests that insomnia might not influence the FoP but that dysfunctional beliefs that insomnia could affect immune dysfunction or cancer progression will lead to fear in patients. On the contrary, we previously showed that, in patients with cancer, FoP affects the severity of insomnia by mediating dysfunctional beliefs about sleep related to cancer.40 As a result of these relationships, insomnia, FoP, and C-DBS can develop into a vicious cycle. Patients with cancer may experience sleep disturbances, dysfunctional beliefs, and FoP. Furthermore, this FoP may aggravate sleep disturbance by increasing dysfunctional beliefs about sleep.
In particular, sleep problems are one of the most distressing symptoms in patients with lung cancer.7 However, no study has explored the relationship between insomnia, C-DBS, and FoP in patients with lung cancer. From the result of this study, we observed that the FoP of patients with lung cancer could be influenced by their sleep and by dysfunctional beliefs about sleep. Therefore, in the concept of CBT-I, physicians must explore dysfunctional worries of cancer patients about their sleep disturbance or cancer progression to improve their quality of life as sleep problems are modifiable factors. This might effectively address dysfunctional beliefs about sleep while performing CBT-I for patients with lung cancer.
In this study, depression directly affected FoP, but dysfunctional beliefs about sleep did not mediate this association. We observed in our previous study that cancer patients’ depression may influence insomnia through cancer-related dysfunctional beliefs.47 In another study, FoP was significantly related to C-DBS.40 In the current study, we observed depression was significantly correlated with dysfunctional beliefs about sleep. Therefore, we expected that dysfunctional beliefs about sleep could mediate the association between depression and FoP, but we could not observe the mediation effect. Additional studies are needed to explore the mediation effect of dysfunctional beliefs about sleep on the association between depression and FoP.
Several limitations should be considered. First, we included patients who volunteered to participate in a study investigating digital applications for cancer patients. We extracted the baseline data of patients from this prior prospective long-term follow-up study, and this might have influenced the results. Second, our participants were all recruited from a single hospital, and the subsequent selection bias may have limited the generalizability of our results. However, more homogeneous participants could be included. Third, rather than conducting interviews with well-trained psychiatrists, the psychiatric symptoms of these patients were assessed using a self-assessed rating scale. Forth, the lack of anxiety assessment scale in this study may also be a limitation since anxiety symptoms need to be considered when assessing psychological distress in patients with cancer. However, FoP innately encompasses worry, illness anxiety, or death anxiety48; thus, we did not include anxiety assessment scales. Furthermore, we were unable to adjust for the relationship between sleep and FoP for physical symptoms of cancer patients such as pain or fatigue, even though these symptoms might influence FoP.43 Further study is needed to explore whether physical symptoms of cancer patients mediate the influence of sleep on their FoP. Among patients with surgically resected lung cancer, dysfunctional beliefs about sleep influenced insomnia severity on their FoP. Depression also directly influenced FoP, but this relationship was not mediated by dysfunctional beliefs. To reduce the fear of cancer recurrence among patients with lung cancer, dysfunctional beliefs about sleep should be addressed during CBT-I.
 XML Download
XML Download