

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Diffuse intrinsic pontine glioma (DIPG) is the most aggressive primary central nervous system malignancy in children, accounting for 10%–20% of all childhood brain tumors [12]. It originates in the pons and commonly infiltrates other regions of the brain stem, further invading into the cerebellum and thalamus via the white matter tracts, and are occasionally accompanied by leptomeningeal dissemination. Together with recent advances in molecular profiling, DIPG has been classified as a new pathologic entity called “diffuse midline glioma, H3K27M-altered” by the World Health Organization [34].
Due to the anatomical complexity and high risk of complications following biopsy, DIPG is usually diagnosed based on characteristic radiographic findings and clinical signs and symptoms. Surgical resection is hindered by its location and infiltrative nature of the tumor. Without any treatment, the prognosis is very dismal with a median survival of approximately 4 months [56]. Radiotherapy is effective as a palliative treatment, providing transient symptomatic improvement, and improves the overall survival (OS) duration by several months [67]. To date, radiotherapy has been considered as the mainstay of treatment for DIPG. Clinical trials of combined chemotherapy provided to improve the prognosis of DIPG have failed to demonstrate a meaningful survival benefit.
Although symptomatic and radiologic responses are achieved with radiotherapy, subsequent tumor progression is almost universal, with a median survival period of 8–11 months in patients with DIPG [18]. To further improve clinical outcomes, the role of alternative radiotherapy fractionation regimens has been investigated. In this review, we summarize the role of radiotherapy and various radiotherapy approaches in the treatment of DIPG.
Go to : 
RADIOTHERAPY AS A DEFINITIVE TREATMENT
The current standard of treatment for DIPG consists of external beam radiotherapy at a dose of 54–60 Gy with conventional fractionation (1.8–2.0 Gy daily, 5 days/week) [1]. This approach has not changed over the decades. Similar to the current recommendation, the Children’s Cancer Study Group study performed in 1977 recommended radiotherapy to be administered 5 times a week at 8–9 Gy/week up to 50–60 Gy [9]. A Korean Radiation Oncology Group (KROG) study reported that the radiotherapy dose did not change over the last 20 years in clinical practice in Korea, and most patients received 54 Gy of radiation with conventional fractionation [10].
Upfront radiotherapy results in a worthwhile, albeit temporary, improvement in neurologic function, although the overall prognosis remains dismal [111213]. The median OS is approximately 12 months after 54 Gy of conventional fractionation radiation. A systematic review of 61 studies involving 1,620 patients treated with upfront conventional radiotherapy with or without systemic therapy showed a median OS of 11.4 months [14]. Similarly, a multicenter study involving 162 patients treated with radiotherapy in Korea for 20 years showed a median OS of 13.1 months and a 2-year OS rate of 19% [10]. OS improved significantly over time, even after adjusting for other prognostic factors, to median OS of 11.4, 13.5, and 17.6 months for patients treated before 2010, during 2010–2015, and after 2015, respectively. The reason may be the improvement in socioeconomic conditions and medical insurance reimbursement because clinical practice of radiotherapy did not change during the period. Age ≤3 or >10 years and longer symptom duration at presentation are prognostic factors associated with a favorable survival outcome [815]. A Korean study [10] also confirmed these significant prognostic factors.
After an upfront radiotherapy, 70%–80% of patients respond to radiotherapy with transient improvement in neurological symptoms, which leads to improvement of quality-of-life. However, this is not sustainable in most of the patients and worsen again with progression of tumor after approximately 6 months [216]. A longitudinal study prospectively evaluating neuropsychological assessments and daily functioning of children with DIPG before and after radiotherapy showed that they exhibited short-term improvements immediately post-radiotherapy in performance-based attention tests and parent-reported behavior, including attention, hyperactivity, behavioral regulation, and executive function. However, these improvements did not persist and significant decline was documented by 6 months [17].
In planning radiotherapy, radiation oncologists determine the optimal target volume and protect the normal organs close to the tumor. However, the optimal margin for the target volume is undefined yet. Most clinical trials recommended a 1–2-cm margin in addition to the gross tumor volume (GTV) for the clinical target volume (CTV) [18192021]. GTV includes contrast-enhanced lesions on magnetic resonance imaging and hyperintense lesions on T2-weighted and fluid-attenuated inversion recovery images. An additional margin of 3–5 mm is added to obtain the planning target volume (PTV). Tinkle et al. [22] evaluated failure patterns of patients with DIPG treated with standard (1 cm) or extended (2–3 cm) margins. Among 93 patients who underwent radiographic evaluation for progression, 87% showed local progression. Central failure (Vprogression95% ≥95%) accounted for 99% of all failures. The failure patterns, progression-free survival (PFS), or OS did not differ significantly with the CTV margin. These findings suggested that an extended margin over 1 cm is not recommended, considering no apparent benefit in tumor control and the high risk of organ damage from the large target volume. Similarly, a multicenter KROG study showed that the infield failure rate was comparable among different CTV margin groups, since most failures represented infield progression (78.6% for no margin, 75.9% for <1 cm of margin, and 86% for 1–2 cm of margin; p=0.160) [10].
Go to :
RADIOTHERAPY APPROACH
Hyperfractionated radiotherapy
Over the decades, numerous trials of the alternative fractionation approach have been performed to overcome the poor prognosis of DIPG (Table 1). The principal focus of these trials has been the use of hyperfractionated radiotherapy, considering the predominantly local pattern of failure and the dose–response relationship in malignant gliomas [23]. The late-responding tissues, such as the normal brain tissues, may be spared from the effects of radiation relative to the tumor with a decreasing dose per fraction [24], which has been the theoretical basis of studies on hyperfractionated radiotherapy.
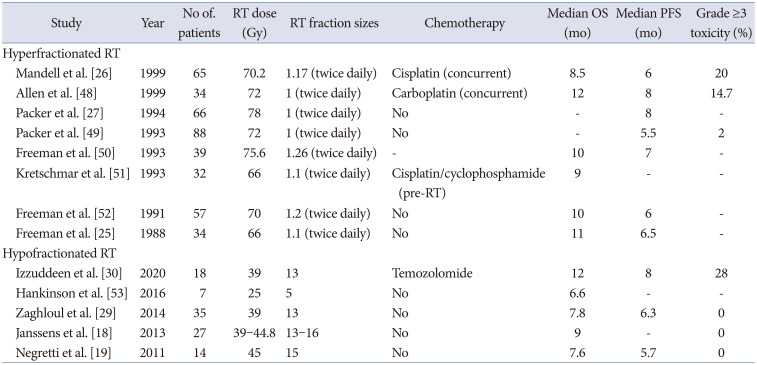
Table 1
Clinical features of studies with hyperfractionated or hypofractionated RT in diffuse intrinsic pontine glioma
| Study | Year | No of. patients | RT dose (Gy) | RT fraction sizes | Chemotherapy | Median OS (mo) | Median PFS (mo) | Grade ≥3 toxicity (%) | |
|---|---|---|---|---|---|---|---|---|---|
| Hyperfractionated RT | |||||||||
| Mandell et al. [26] | 1999 | 65 | 70.2 | 1.17 (twice daily) | Cisplatin (concurrent) | 8.5 | 6 | 20 | |
| Allen et al. [48] | 1999 | 34 | 72 | 1 (twice daily) | Carboplatin (concurrent) | 12 | 8 | 14.7 | |
| Packer et al. [27] | 1994 | 66 | 78 | 1 (twice daily) | No | - | 8 | - | |
| Packer et al. [49] | 1993 | 88 | 72 | 1 (twice daily) | No | - | 5.5 | 2 | |
| Freeman et al. [50] | 1993 | 39 | 75.6 | 1.26 (twice daily) | - | 10 | 7 | - | |
| Kretschmar et al. [51] | 1993 | 32 | 66 | 1.1 (twice daily) | Cisplatin/cyclophosphamide (pre-RT) | 9 | - | - | |
| Freeman et al. [52] | 1991 | 57 | 70 | 1.2 (twice daily) | No | 10 | 6 | - | |
| Freeman et al. [25] | 1988 | 34 | 66 | 1.1 (twice daily) | No | 11 | 6.5 | - | |
| Hypofractionated RT | |||||||||
| Izzuddeen et al. [30] | 2020 | 18 | 39 | 13 | Temozolomide | 12 | 8 | 28 | |
| Hankinson et al. [53] | 2016 | 7 | 25 | 5 | No | 6.6 | - | - | |
| Zaghloul et al. [29] | 2014 | 35 | 39 | 13 | No | 7.8 | 6.3 | 0 | |
| Janssens et al. [18] | 2013 | 27 | 39–44.8 | 13–16 | No | 9 | - | 0 | |
| Negretti et al. [19] | 2011 | 14 | 45 | 15 | No | 7.6 | 5.7 | 0 | |
![]()
In the 1980s, the Pediatric Oncology Group (POG) performed a phase I/II trial of the efficacy and toxicity of hyperfractionated radiotherapy administered twice daily in children with brainstem glioma. Survival tended to increase with an increase in the radiation dose from 66 Gy to 72 Gy but did not change with an increase in the radiation dose from 72 Gy to 75.6 Gy [25]. To further address this issue, the POG 92-39, a phase III prospective randomized controlled trial, comparing hyperfractionated (1.17 Gy/fraction twice daily up to 70.2 Gy) and conventional (1.8 Gy/fraction once daily up to 54 Gy) radiotherapy with cisplatin showed no improvement with either approach in progression or survival [26]. A Children’s Cancer Group (CCG) phase I/II trial of the safety and efficacy of hyperfractionated radiotherapy with a dose of 78 Gy also showed no improvement in objective responses with hyperfractionated radiotherapy compared to conventional fractionation and accompanying possible radiation-associated normal tissue damage with a higher dose of radiation [27].
Gallitto et al. [14] performed a systematic review to identify all available studies until 2018 involving patients with DIPG treated with radiotherapy. Of all eligible studies, 49 (1,286 patients) used conventional fractionated radiotherapy and 8 (348 patients) used hyperfractionated radiotherapy. The median OS was 12.0 and 10.2 months in patients who received conventional and hyperfractionated radiotherapy, respectively. In the Cochrane Database of Systematic Review, a review compared hyperfractionated and conventional radiotherapy in 2016 and revealed no clear evidence of the effect on OS or event-free survival (EFS) on patients receiving hyperfractionated radiotherapy compared to conventional radiotherapy (OS: hazard ratio [HR]=1.07, 95% confidence interval [CI]: 0.75 to 1.53; EFS: HR=1.26, 95% CI: 0.83 to 1.90) [28].
Considering the paucity of data in favor of hyperfractionation radiotherapy, hyperfractionation radiotherapy is not promising in clinical practice and undesirable because of the discomfort of two sessions per day and possible damage to the healthy organs caused by higher doses.
Hypofractionated radiotherapy
Considering that the median survival of patients with DPIG is approximately 12 months, hypofractionated radiotherapy has been evaluated to shorten the treatment period and reduce hospital visits. Negretti et al. [19] reported a single institution’s experience with 22 patients treated with hypofractionated radiotherapy with 3 Gy/fraction up to 45 Gy over 3 weeks (Table 1). The median OS was 7.6 months, similar to that in other previous studies using conventional fractionation. However, the daily fraction was modified to 2 Gy because of intolerance in 5 cases, and one patient died from serious intracranial hypertension. A matched cohort analysis by Janssens et al. [18] compared outcomes of hypofractionated (44.8 Gy in 16 fractions or 39 Gy in 13 fractions) and conventional fractionated radiotherapy, which revealed that hypofractionated radiotherapy provided equivalent survival outcomes with shortening of the overall treatment time. Zaghloul et al. [29] performed the first related prospective randomized controlled trial involving 35 patients receiving hypofractionated radiotherapy (3 Gy/fraction up to 39 Gy) and 36 patients receiving conventional fractionation (1.8 Gy/fraction up to 54 Gy). The non-inferiority trial revealed median OS of 7.8 and 9.5 months in the hypofractionated and conventional groups, respectively, showing no significant differences, thereby failing to fulfill the non-inferiority assumption.
Another phase II randomized controlled trial from India aimed to determine whether or not hypofractionated radiotherapy (39 Gy in 13 fractions) with 75 mg/m2 body surface area of concurrent temozolomide followed by adjuvant temozolomide for 6 cycles improved the prognosis better than conventional fractionated radiotherapy (60 Gy in 30 fractions) [30]. Hypofractionated radiotherapy with temozolomide did not improve survival outcomes and accompanied higher hematologic toxicity compared to conventional fractionated radiotherapy. A recently published meta-analysis performed to overcome the small sample size of previous studies included 4 articles, involving 88 patients undergoing hypofractionated radiotherapy and 96 patients undergoing conventional fractionation radiotherapy [31]. It revealed that hypofractionated and conventional fractionation radiotherapy provided comparable OS (HR=1.07, 95% CI: 0.77–1.47) and PFS (HR= 1.04, 95% CI: 0.75–1.45) and had similar toxicity profiles. However, this result cannot change the current mainstay of conventional radiotherapy in patients with DIPG because of the small number of patients and retrospective design of some included studies. To overcome this limitation, a phase III non-inferiority randomized trial comparing hypofractionated (39 Gy in 13 fractions and 45 Gy in 15 fractions) and conventional fractionated (54 Gy in 30 fractions) radiotherapy was performed and recently published [32]. They randomized 253 patients into 3 arms of radiation regimens. The results revealed median OS of 9.6, 8.2, and 8.7 months in the 39 Gy in 13 fractions, 45 Gy in 15 fractions, and conventional groups, respectively, fulfilling their non-inferiority assumption (noninferiority margin of 15%) at 18 months OS. Younger patients (2–5 years of age) had better OS, excepting for those in 45 Gy in 15 fractions group, which may seem that the higher radiation dose with higher biologically effective dose deprived the younger patients of their inherited superior survivals.
Based on the results so far, hypofractionation radiotherapy can be performed with a dose of 39 Gy in 13 fractions in patients with DIPG according to the clinician’s discretion considering the patient’s condition and tumor location.
Go to :
PROTON THERAPY
In all aforementioned studies, radiation was delivered as photon beams, which is the basis of external beam radiation and the treatment adopted worldwide. Proton therapy is a type of particle radiotherapy with relatively constant energy deposition up to the Bragg peak and a subsequent drop because of the depth–dose distribution of particles. It has the advantage of protecting the surrounding healthy organs by reducing the radiation dose behind the Bragg peak. Although proton therapy is theoretically useful in reducing the radiation dose to healthy brain tissue, studies investigating proton therapy in patients with DIPG scarce.
A small retrospective study from Japan reported clinical outcomes of 12 children who received proton therapy for DIPG at the University of Tsukuba Hospital [33]. The target volume was defined as similar typical radiotherapy volumes: CTV as the GTV plus a 5–10-mm margin and PTV as the CTV plus 2–3-mm margin. A total dose of 54 Gy (relative biological effectiveness [RBE]) in 30 fractions was delivered to the PTV during proton therapy.
Median PFS and OS were 5 and 9 months, respectively, showing no significant difference from the conventional photon radiotherapy group in which the median PFS and OS were 5 and 11 months, respectively. Proton therapy was well tolerated and caused a grade 3 low neutrophil count in only one patient; however, the proton therapy was not safer or more effective treatment compared to conventional photon radiotherapy.
Although proton therapy is a priority in pediatric low-grade glioma [34], it may be contraindicated in high-grade gliomas, including DIPG, because of poor outcomes and a short survival prognosis which render patients unable to benefit from the advantages of proton therapy. In addition, uncommon but serious morbidities, including symptomatic brainstem injury after proton beam radiation, have been reported [353637]. Unlike photons, protons differ in linear energy transfer (LET) and RBE, which are increased within the distal segments of the spread-out Bragg peak (SOBP). This can lead to unexpected brainstem injury. Caution should be exercised to limit brainstem exposure to the distal or lateral aspects of SOBP. Further, brainstem tolerance doses should be reduced, and RBE and LET should be accounted for [38].
Go to :
RE-IRRADIATION AS SALVAGE TREATMENT
Re-irradiation for patients with DIPG is an emerging salvage treatment as it can alleviate the symptoms and improve the prognosis. Fractionated re-irradiation may be considered at the time of progression, although it may increase the risk of toxicity. A few studies have been reported to date; however, a conclusive implication of re-irradiation is difficult to draw because of the small number of patients included in each study (Table 2) [39404142434445]. The first and only prospective study was a phase I/II trial conducted to determine the optimal dose of reirradiation for patients with DIPG. Three dose levels (24 Gy in 12 fractions, 26.4 Gy in 12 fractions, and 30.8 Gy in 14 fractions) were evaluated in 12 patients, and the regimen of 24 Gy in 12 fractions was preferred, considering its safety profiles and efficacy in clinical outcomes. Clinical improvement was observed in all but one patient, and quality of life was improved in almost two-thirds of the patients with a median OS of 19.5 months and median PFS of 4.5 months from the start of reirradiation. Other retrospective studies published before this study usually used a regimen of 18–20 Gy in 10 fractions and reported a median OS of 3–7 months after re-irradiation with an acceptable tolerability [3940414344]. The largest retrospective study was a matched cohort analysis performed by the European Society for Paediatric Oncology (SIOPE) high-grade glioma (HGG)/DIPG working group. It involved 31 children who underwent re-irradiation for DIPG and 39 children as the matched cohort [39]. It showed a survival benefit with re-irradiation (median OS: 13.7 months for re-irradiation vs. 10.3 months for control; p=0.04). The survival benefit was prominent with a longer interval between end-of-radiotherapy and first progression, and clinical improvement was observed in 77% of patients. Lassaletta et al. [43] published a Canadian multicenter series of 16 patients treated with re-irradiation at a dose of 21.6–36 Gy (median: 30.6 Gy) for recurrent DIPG. The median survival from progression to death was 92 days in patients without re-irradiation and 218 days in patients with re-irradiation (p=0.0001). Although the results are not conclusive, we could consider re-irradiation with a dose of 30.6–36.0 Gy in 17–20 fractions as a salvage treatment, particularly when the interval from upfront radiotherapy is long. Recently, Krishnatry and Manjali [46] reported the largest single institution series from Tata Memorial Center involving 20 patients treated with higher dose of re-irradiation (median 41.4 Gy, range 33.8–43.2 Gy) according to a response-based dose escalation approach. Clinical outcomes for all patients were comparable to previously reported studies with a median OS of 5.5 months after re-irradiation and 16.6 months from initial diagnosis, respectively. Notably, they evaluated the median OS according to the radiation dose groups (5.8 months for 39.6–41.4 Gy, 7 months for 43.2 Gy, and 5.3 months for 45 Gy group), and suggested there may be a dose-response benefit although statistical analysis was not performed due to the small sample size.
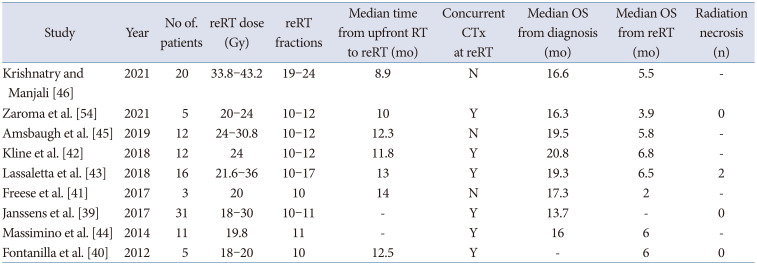
Table 2
Clinical features of studies with re-irradiation in diffuse intrinsic pontine glioma
| Study | Year | No of. patients | reRT dose (Gy) | reRT fractions | Median time from upfront RT to reRT (mo) | Concurrent CTx at reRT | Median OS from diagnosis (mo) | Median OS from reRT (mo) | Radiation necrosis (n) |
|---|---|---|---|---|---|---|---|---|---|
| Krishnatry and Manjali [46] | 2021 | 20 | 33.8–43.2 | 19–24 | 8.9 | N | 16.6 | 5.5 | - |
| Zaroma et al. [54] | 2021 | 5 | 20–24 | 10–12 | 10 | Y | 16.3 | 3.9 | 0 |
| Amsbaugh et al. [45] | 2019 | 12 | 24–30.8 | 10–12 | 12.3 | N | 19.5 | 5.8 | - |
| Kline et al. [42] | 2018 | 12 | 24 | 10–12 | 11.8 | Y | 20.8 | 6.8 | - |
| Lassaletta et al. [43] | 2018 | 16 | 21.6–36 | 10–17 | 13 | Y | 19.3 | 6.5 | 2 |
| Freese et al. [41] | 2017 | 3 | 20 | 10 | 14 | N | 17.3 | 2 | - |
| Janssens et al. [39] | 2017 | 31 | 18–30 | 10–11 | - | Y | 13.7 | - | 0 |
| Massimino et al. [44] | 2014 | 11 | 19.8 | 11 | - | Y | 16 | 6 | - |
| Fontanilla et al. [40] | 2012 | 5 | 18–20 | 10 | 12.5 | Y | - | 6 | 0 |
![]()
All studies reported to date have included only a small number of patients, except for the study from the SIOPE HGG/DIPG working group. To offset the limitation driven from the small cohort of each study, a systematic review and meta-analysis of seven studies involving 90 patients was recently reported by Lu et al. [47]. In this review, the pooled incidences of clinical improvement and acute serious toxicity following reirradiation were 87% and 0%, respectively. Pooled PFS and OS from the time of re-irradiation were 4.2 and 6.2 months, respectively. The pooled median OS in the re-radiation group was 18.0 months, implicating that re-irradiation may be an effective therapeutic intervention in select patients with DIPG. A non-randomized phase II trial of the efficacy of conventional fractionation re-irradiation with a dose of 30.6 Gy or 36 Gy in recurrent or progressive DIPG is underway (NCT03126266) [17].
Go to :
CONCLUSIONS
Despite recent advances in medical technology, including molecular, imaging, and therapeutic aspects, pediatric DIPG remains an unsolved problem. To date, numerous clinical trials have explored potential therapeutic challenges in DIPG and showed no improvement in survival. Conventional radiotherapy with a dose of 54 Gy remains the only proven therapeutic option. Recent advances in molecular profiling has ushered in a new era of DIPG, leading to the development of new targeted approaches to treat DIPG. While clinical studies are required before application in clinical practice, the results of these studies may serve as a basis to discover more effective treatment options for DIPG.
Go to :
 XML Download
XML Download