

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Prolactinoma, a prolactin-secreting adenoma arising from the lactotroph cells of the pituitary gland, accounts for approximately 40% of all pituitary adenomas and mostly occurs in women aged 20–40 years [1]. The clinical presentations of prolactinoma originate from its hormonal and mass effects. Hyperprolactinemia causes galactorrhea via its direct effect on breast epithelial cells, which leads to hypogonadism via regulation of gonadotropin-releasing hormone. Thus, women typically present with amenorrhea, oligomenorrhea, dyspareunia, or even infertility as well as osteoporosis. The mass effect of the tumor causes visual dysfunction, and 50% of patients present with headaches, which reduces their quality of life [23].
The goal of prolactinoma treatment is to relieve symptoms and preserve the gonadal status by normalizing prolactin levels and decreasing the tumor size. The remission rate of disease following treatment with dopamine agonists (DAs) is 91% in microprolactinoma and 77% in macroprolactinoma [4].
However, surgical treatment is inevitable given the side effects of long-term drug use, such as nausea, vomiting, headache, dizziness, and apoplexy. Recent advances in surgical techniques have made radical resection of prolactinoma feasible, especially for microadenomas or small noninvasive macroadenomas, with minimal surgical complications [45]. Moreover, an increasing number of studies have reported excellent outcomes for patients who are surgically treated without DA medication trials. As the role of surgical resection has become more important in the treatment of prolactinomas, several studies have attempted to predict hormonal remission after surgical treatment of prolactinoma. Some studies have reported that tumor size and extent and prolactin levels are related to outcomes, and most recent studies have identified a clear correlation between preoperative and postoperative factors [67]. However, no study has highlighted the importance of postoperative prolactin level measurement or suggested a clear threshold value that differentiates surgical remission and non-remission [8].
In this study, we performed a retrospective analysis of postoperative prolactin levels in patients with surgically treated prolactinomas in order to evaluate their predictive power relationship with time-dependent remission and their feasibility in predicting long-term outcomes.
Go to : 
MATERIALS AND METHODS
Patient selection and study design
We searched the electronic medical record for patients with histologically confirmed prolactinomas who underwent surgery at our institution between December 2010 and April 2018; 108 patients were recruited. To refine our patient population for reliable statistical modeling, we set the following strict criteria: 1) We only included patients who underwent complete tumor removal, as confirmed by postoperative MRI. 2) We excluded men because of insufficient patient numbers and differences in the standard of remission criteria. 3) We excluded any patient with previous surgery or radiation history. 4) We only included patients who were followed up for more than 12 months. Consequently, one patient with incomplete medical records was excluded and two male patients were excluded. Finally, 105 patients were enrolled in this study. This study was conducted in accordance with the Declaration of Helsinki and was approved by the local Institutional Review Board (4-2022-1018).
Preoperative assessment
All patients underwent tumor resection based on either a direct microscopic or an endoscopic endonasal transsphenoidal approach. The choice of surgical approach was based on the surgeon’s preference. In most cases, surgical removal was performed as the second-line treatment after DA therapy failure, and in a few cases, surgical treatment was adopted because of the patient’s personal preference. DA therapy failure was defined as a decrease of <50% in the tumor size after bromocriptine or cabergoline administration or the failure of normalization of prolactin level or DA cessation owing to their side effects [910].
A preoperative workup, including physical examination, endocrine laboratory testing with a pituitary function test, and MRI, was performed for all patients. Basal hormone tests for anterior pituitary hormones including adrenocorticotropic hormone, growth hormone, prolactin, thyroid stimulating hormone, follicle-stimulating hormone and the free α-small unit of luteinizing hormone and its target hormones including insulin-like growth factor-I, free T4, free T3 and estradiol measurements were performed before and after surgery. Tumor size was defined as the longest diameter of the tumor in the T1 contrast coronal view on MRI using a 1.5-T system (Signa; General Electric, Minneapolis, MN, USA) or a 3-T system (Achieva; Philips, Best, The Netherlands). All prolactinomas were classified according to a modified Hardy radiological classification scheme: type I was confined entirely within the sella turcica and was <1 cm, whereas type II extended into the suprasellar space <1 cm above the line of the diaphragm. Preoperative DAs were used in 90 patients; bromocriptine was used in 8 patients, cabergoline in 49 patients, and both in 33 patients.
Postoperative evaluation and management
Postoperative MRI was performed within 48 h after surgery to assess the extent of resection. In addition, patients were followed up with MRI annually for the first 2 years and then every 2 years thereafter. Only patients with no residual tumor on intraoperative inspection by the surgeon and postoperative MRI evaluation were included in the study. During the immediate postoperative period, prolactin levels were serially measured at 2, 6, 12, 18, 24, 48, and 72 h after surgery.
Normal serum prolactin level was defined as <25 ng/dL in female patients. The patients were followed up for 12–102 months after surgery, and the prolactin levels and associated symptoms before surgery, such as galactorrhea or amenorrhea, were evaluated during follow-up. Surgical remission was defined when patients showed normal prolactin levels and no associated symptoms without postoperative DA therapy. A basal hormone test including prolactin was performed at 1, 3, 6, 12, 18, and 24 months after surgery and every 6–12 months thereafter.
Of the 105 patients, 95 had remission, and the remaining 10 needed continuous postoperative DA therapy. One patient in the non-remission group was confirmed to have delayed remission after 7 years of postoperative DA therapy. No patient underwent radiosurgery or conventional radiotherapy.
Statistical analysis
Descriptive statistics were used to summarize the patient characteristics. Continuous variables were examined using the Shapiro–Wilk test to determine the normality of the distribution and then expressed as mean and standard deviation. Student’s t-test was performed depending on the normality of the distributions of the variables, as appropriate. Categorical variables are described as numbers with percentages and were compared using the chi-square and Fisher’s exact tests, as appropriate.
The area under the receiver operating characteristic (ROC) curve (AUC) was used to describe and compare the overall performance at each time point. Predictive power was compared based on the AUC. All data processing and statistical analyses were performed using the R software, version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). A two-tailed p-value of <0.05 was considered statistically significant for all analyses.
Go to :
RESULTS
Demographic and clinical characteristics
We analyzed the relationship between long-term patient outcome and its associated operative factors; preoperative prolactin level, tumor size, and DA use. The mean age was 30.45 years in the remission group and 29.20 years in the non-remission group. The mean follow-up duration was 38 months (range: 12–102 months). Based on the modified Hardy classification scheme [1112], microadenomas (Hardy type I) represented the largest proportion (80.9%), followed by Hardy type II (19.1%) (Table 1). A total of 95 (90.5%) patients achieved remission, whereas 10 (9.5%) did not.
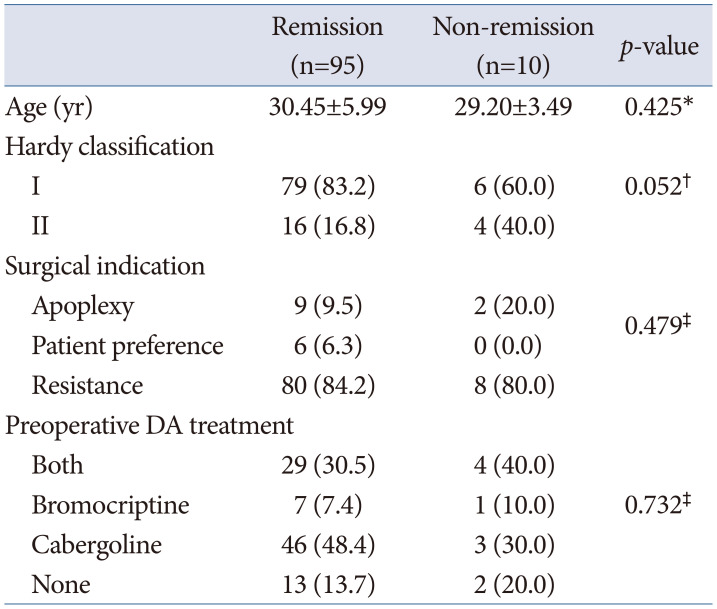
Table 1
Demographics and clinical characteristics of patients with prolactinoma
![]()
Among the 105 patients who underwent surgical treatment for prolactinoma, the difference between the initial prolactin level at diagnosis and the prolactin level the day before surgery was not significant. Tumor size and tumor extent based on the modified Hardy classification affected tumor resectability. However, only the tumor size affected the remission rate (Table 2).
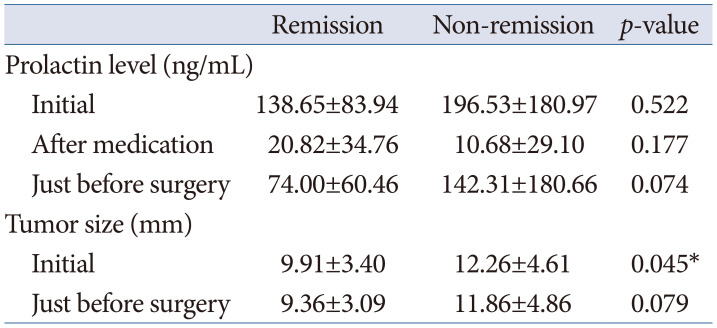
Table 2
Preoperative clinical characteristics in patients with prolactinoma in the comparison between remission and non-remission groups
![]()
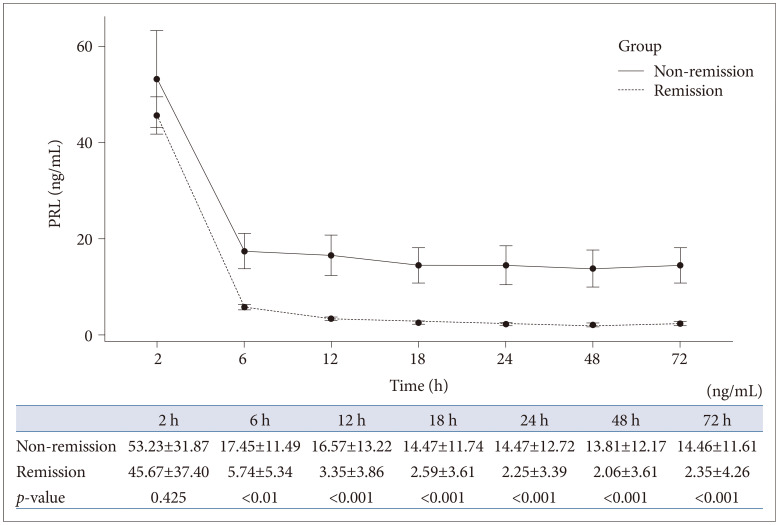
Immediate postoperative prolactin level measurement
Prolactin levels were measured at serial intervals from 2 to 72 h postoperatively. There was a significant difference in the prolactin levels from the time point of postoperative 6 h until 72 h after surgery between the remission and non-remission groups (Fig. 1).
ROC analysis was used to assess the predictive power of postoperative prolactin levels on long-term outcomes. We discovered that the AUC value could predict long-term outcomes from 6 h after surgery, with a range of 0.817 to 0.897. Furthermore, the AUC continued to increase and peaked 72 h after surgery (Table 3). At each postoperative time point, we determined a cut-off value that showed a significant relationship with disease remission. The likelihood of remission increased when the prolactin level was below 10.30 ng/mL at 6 h postoperatively, below 7.15 ng/mL at 12 h, below 6.45 ng/mL at 18 h, below 5.85 ng/mL at 24 h, below 6.00 ng/mL at 48 h, and below 6.40 ng/mL at 72 h.
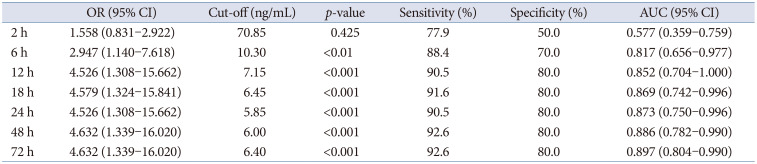
Table 3
Immediate postoperative prolactin levels
![]()
Further treatments for non-remission patients
DA therapy was initiated if hyperprolactinemia and its associated symptoms persisted even after the complete tumor resection. Of the 105 patients, 10 (9.5%) stayed in non-remission condition. One of the 10 patients with non-remission attained delayed remission after 7 years of DA therapy. A recurrent tumor was observed in another patient with hyperprolactinemia during postoperative DA therapy, and the patient underwent a second surgery. For the remaining eight patients, we continued DA treatment and regular follow-up via image evaluation and hormone level assessment at the outpatient clinic.
Go to :
DISCUSSION
Prolactinomas are typically treated with DAs; however, surgical treatment also plays a major role, particularly in cases where DAs are contraindicated, poorly tolerated, or ineffective [41314]. Recently, many studies have reported excellent outcomes of surgical treatment for prolactinomas and suggested that surgical treatment may play a primary role in prolactinoma treatment [1516].
Radical surgery, in which the tumor is removed along with the pseudocapsule, is important because the pseudocapsule may contain tumor cells that hinder complete resection, thus increasing the risk of recurrence [17]. However, complete resection, determined by surgeon’s impression and postoperative radiological evaluation, does not always lead to endocrinological remission [1819]. Therefore, the development of reliable predictors is extremely helpful for predicting postoperative outcomes and guiding treatment decisions.
Previous studies have suggested many potential predictors, with the main focus on preoperative factors such as tumor size, invasiveness, prolactin level, and MRI characteristics; however, these predictors have shown inconsistent results [2021]. Our study focused on the predictive value of serial postoperative prolactin levels rather than preoperative predictors. Since normal lactotrophs are suppressed by prolonged negative feedback, prolactin levels should decrease to a subnormal level in cases of radical tumor removal [22]. We previously demonstrated that immediate postoperative measurement of hypersecreting hormones reliably predicts long-term remission in acromegaly and thyroid-stimulating hormone-secreting pituitary adenoma models [2324]. We hypothesized that this predictive modeling system may also be useful for patients with surgically treated prolactinoma. We demonstrated that the prolactin level became reliable after 6 h postoperatively in differentiating between remission and non-remission patients and, thereafter, remained a good predictor. In addition to being a reliable predictor throughout the entire time point after 6 h postoperatively, it became the most predictive at 72 h after surgery.
In accordance with our findings, several studies have also suggested the importance of measuring postoperative prolactin levels as a reliable predictor. Amar et al. [25] also reported that the prolactin level on the first postoperative day is a significant predictor of long-term outcomes. They simply grouped their patients according to their prolactin levels, which demonstrated intergroup differences in the chance of remission. Penn et al. [8] reported that a prolactin level higher than 7.6 ng/mL measured on the first postoperative day acts as an important predictor of surgical failure. No studies have described time-dependent postoperative changes in prolactin levels during the immediate postoperative period. We successfully demonstrated the difference in prolactin levels between remission and non-remission groups. In addition, optimal cut-off values were suggested at each specific time point. We believe that our predictive modeling system contributes to early identification of patients who require adjuvant treatment after surgery.
This study has several limitations. First, this was a single-center retrospective study with a relatively small sample size. Multicenter study based on larger number of patients will be required for scalability and generalizability in future. Second, only patients who underwent complete surgical resection were included based on the belief that incomplete surgical resection does not result in endocrinological remission. As the judgement made by a surgeon and a radiologist is often inaccurate, our mathematical modeling system should be applied cautiously when extent of resection is uncertain. Third, applying overly stringent criteria to test the hypotheses can be disadvantageous in terms of diversity. As male patients were excluded from our study, other mathematical modeling is necessary to test immediate postoperative prolactin level as a predictor. In addition, the use of preoperative DA hugely affects the prolactin level measured just before surgery, which necessitates a different mathematical modeling for the patients without preoperative DA trial. Lastly, with longer follow-up, more recurrent cases may possibly change the optimal cut-off in the prediction of remission.
In conclusion, this study demonstrates that serial postoperative prolactin levels are powerful and reliable predictors of long-term endocrinological remission. We observed that the postoperative prolactin level stayed reliable at 6 h after surgery and thereafter and reached the most predictive point at 72 h after surgery. We believe that serial postoperative prolactin monitoring is a useful predictive tool, which contributes to early identification of patients who require adjuvant treatment after surgery.
Go to :
 XML Download
XML Download