

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gliomas, which constitute around 60% of all primary brain cancers, are tumors of glial cells that have differentiated from neuroectoderm. Gliomas are classified using the WHO classification of tumors of the central nervous system (CNS) and gades III and IV have been termed as high-grade gliomas (HGG) in previous editions [1]. Recently in 2021, the WHO has combined molecular diagnostics along with histopathology into the classification of brain tumors [2]. However, the historic clinicopathological grading system has been retained for prognostication but use of Roman numerals has been replaced with Arabic numerals for assigning tumor grades [2].
WHO grade 4 tumors are the most common type of HGGs and almost exclusively glioblastoma multiforme (GBM) by histopathology. HGGs are known to have poor prognosis due to significant invasive potential that hampers complete surgical excision [3]. Radiation with or without chemotherapy, in unresectable HGG cases, are less effective and thus achieving local control is challenging in such scenario [4]. The majority of patients succumb to local disease progression, local recurrences, or unmanageable intracranial hypertension [5]. Since most glioma recurrences occur within 2 cm of the original tumor site, quick and effective management depends on early and precise detection of a tumor recurrence and distinguishing recurrences from therapy-related alterations [67]. Currently, postoperative concurrent radio chemotherapy followed by adjuvant chemotherapy using temozolomide (TMZ) is the standard of care after maximal safe resection [8].
Neurocognitive impairment is another factor that needs to be weighed into clinical and therapeutic decisions for HGG patients. Neurocognitive functions (NCF) in these patients are affected by various factors, including the tumor itself, seizures related to the tumor, treatment therapies like surgery and radiotherapy, and patient parameters (e.g., age, psychological distress etc.) [9]. Decline in NCF eventually compromises patient’s independence, causing behavioral, emotional, and intellectual deficits, thereby hampering social and professional responsibilities. Preservation of NCF and providing better quality of life to glioma patients is becoming increasingly important as survival rates are improving with better therapies [1011].
Patients with HGG are found to have cognitive deficits more frequently than those with low-grade gliomas due to significant alterations in cognitive domains such as language, attention, memory, empathy and executive functions [12]. Most treatment naïve glioma patients also suffer from cognitive impairment, which suggests that neurocognitive dysfunction may correlate with the disease itself [13]. The Response Assessment in Neuro-Oncology (RANO) committee also advocates the assessment of neurological status for response to treatment therapies in glioma patients [14]. Various studies have used diverse methods and tools to evaluate neurocognition in glioma patients. One such method for evaluating HGG patients receiving radiotherapy is the Mini-Mental State Examination (MMSE) questionnaire [15]. It is a patient reported subjective assessment tool, widely implemented in various trials on glioma patients and also endorsed by the European Association of Neuro-Oncology (EANO) guidelines [1617]. Assessment of change in the pattern of NCF in HGG patients is essential in optimizing interventions like the use of neuroprotectors, in guiding future clinical trials on newer therapies and in determining the biological mechanisms associated with radiation induced neurocognitive impairment.
With this background, the current prospective study was conducted with the aim of assessing the change in NCF of HGG patients undergoing radiotherapy with concurrent chemotherapy and to identify risk factors for neurological deficits in them.
Go to : 
MATERIALS AND METHODS
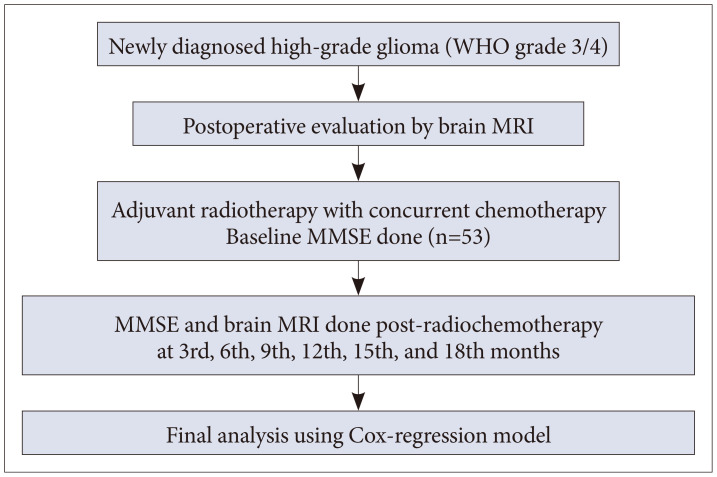
This prospective observational study was conducted in a tertiary cancer center of Northeast India after obtaining necessary approval of the Institutional Ethics Committee of Dr. B. Borooah Cancer Institute, Guwahati (Ref. No. BBCI-TMC/Misc-01/MEC/183/2020). All patients were required to provide written informed consent prior to study participation. The study complies with the principles enshrined in the Declaration of Helsinki. Fig. 1 depicts the workflow of our methodology in conducting this study.
Patient selection
Patients with diagnosis of glioma who visited our hospital for treatment were considered in this study. Patients were recruited between August 2020 to August 2021. Selection criteria included histopathologically proven newly diagnosed HGG (WHO grade 3 or 4) with age 18 years and above. Patients must have undergone maximal safe resection of their tumors by a neurosurgeon, which could be gross total resection (GTR), subtotal resection (STR), or biopsy only. Exclusion criteria included patients who were unable to write, speak, or answer the study questionnaire. Those with poor performance status (Karnofsky performance score less than 70), presence of any secondary CNS malignancy or other diseases causing cognitive impairment, history of previous brain radiotherapy, and severe medical comorbidities were also excluded from this study.
After accrual into the study, the postoperative specimen/blocks of the patients were subjected to immunohistochemistry for testing of molecular markers and appropriate grading. The tumor histology was defined based on presence/absence of isocitrate dehydrogenase (IDH) mutation and 1p/19q co-deletion as per the 2016 WHO classification of CNS tumors. Those who had H3K27 M-mutant were termed as diffuse midline glioma.
Various parameters related to demographic and disease characteristics of the enrolled patients were systematically recorded.
Treatment protocol
HGG patients enrolled in the study were treated with radiotherapy of the target volume using volumetric modulated arc therapy (VMAT) to a dose of 60 Gy in 30 fractions, along with concurrent TMZ at a dose of 75 mg/m2/day orally. After completion of radiotherapy, patients were prescribed adjuvant TMZ (150–200 mg/m2 for 5 days), given every 28 days for 6 cycles. Patients, who tolerated 6 cycles of TMZ without any grade 2 or above toxicities, were considered for 2 more cycles of adjuvant TMZ (up to 8 cycles) according to the institutional protocol.
Surgical or medicinal decompression therapy was used to relieve intracranial tension. Dexamethasone was used with a loading dosage of 0.5–1 mg/kg intravenously followed by a tapering dose (0.25 mg/kg/day) intravenously or per-orally in divided doses every 6–8 hours, combined with antacids for gastrointestinal protection.
Volume delineation and treatment planning
Preoperative and postoperative MRI scans of tumors of each patient were assessed and compared for treatment planning. The planning CT-simulation scans were co-registered with postoperative contrast-enhanced T1-weighted and T2/FLAIR sequences of MRI scans in the treatment planning system (TPS). Target volumes were delineated according to the European Organization for Research and Treatment of Cancer (EORTC) consensus recommendations [18]. Surgical cavity plus any residual enhancing tumor on postoperative T1-weighted MRI scans were delineated as gross tumor volume. An isotropic margin of 2 cm with inclusion of peritumoral edema formed the clinical target volume (CTV) after reductions respecting anatomical barriers of tumor spread. A 3 mm margin over CTV generated the planning target volume (PTV) to which the dose was prescribed. The treatment planning was performed using the Eclipse TPS using 6 MV photon beams with VMAT for treatment delivery in a Varian Trilogy linear accelerator equipped with Millennium 120 MLC (Varian Medical Systems, Inc., Palo Alto, CA, USA). Plan evaluation criteria required at least 97% of the PTV to be covered by the prescribed dose while restricting doses to surrounding critical normal structures. The plan with the most optimal outcome in both parameters would be approved for final treatment. Treatment was delivered daily for 5 days a week to a total dose of 60 Gy in 30 fractions at 200 cGy per fraction.
Neurological examination and follow-up
The MMSE questionnaire was used to measure cognitive impairment of each study patient by examining functions such as registration, attention, calculation, language, recall, orientation, and ability to follow simple commands. The maximum score is 30 points in one assessment. Cognitive impairment was defined as an MMSE score of less than 24 (mild with an MMSE score of 18–23 and severe with a score of 0–17). All the patients were subjected to the questionnaire before starting treatment (at baseline), at the completion of treatment, and at 3, 6, 9, 12, 15, and 18 months of follow-up. Brain MRI was also done at 3-month intervals to assess disease response according to RANO criteria [14]. Each study patient was kept on follow-up till disease progression or death.
Statistical analysis
The outcome of interest was the time to cognitive impairment in months among study patients. The potential risk factors of cognitive impairment considered in the analysis were age, sex, recursive partitioning analysis (RPA), tumor grade, type (histology), IDH type, alpha-thalassemia X-linked mental retardation (ATRX), site, lobe, and type of surgery. Categorical variables were presented as frequency and proportion. Continuous variables were presented as mean (±standard deviation, SD). First, univariate Cox regression was done to evaluate risk factors of cognitive impairment in patients with HGG. The variables found statistically significant in univariate Cox regression were taken in the final multivariable Cox regression model. The predictive accuracy of the multivariable model for cognitive impairment was assessed by receiver operating characteristic (ROC) curve. An independent t-test was used to compare the means (±SD) of continuous variables between the 2 groups. p value <0.05 was considered statistically significant. Data were analyzed by using coGuide software Version 1.03 [19].
Go to :
RESULTS
Fifty-three patients who fulfilled the study inclusion criteria were enrolled. The sociodemographic and clinical characteristics of the study population are depicted in Table 1. The majority were males aged less than 50 years. Grade 4 tumors consisted of nearly 70% of the cohort, of which 54.7% were glioblastoma histology. Mutation in IDH gene was seen in two-thirds of the cohort and majority underwent STR of their tumors on surgery (62.3%).
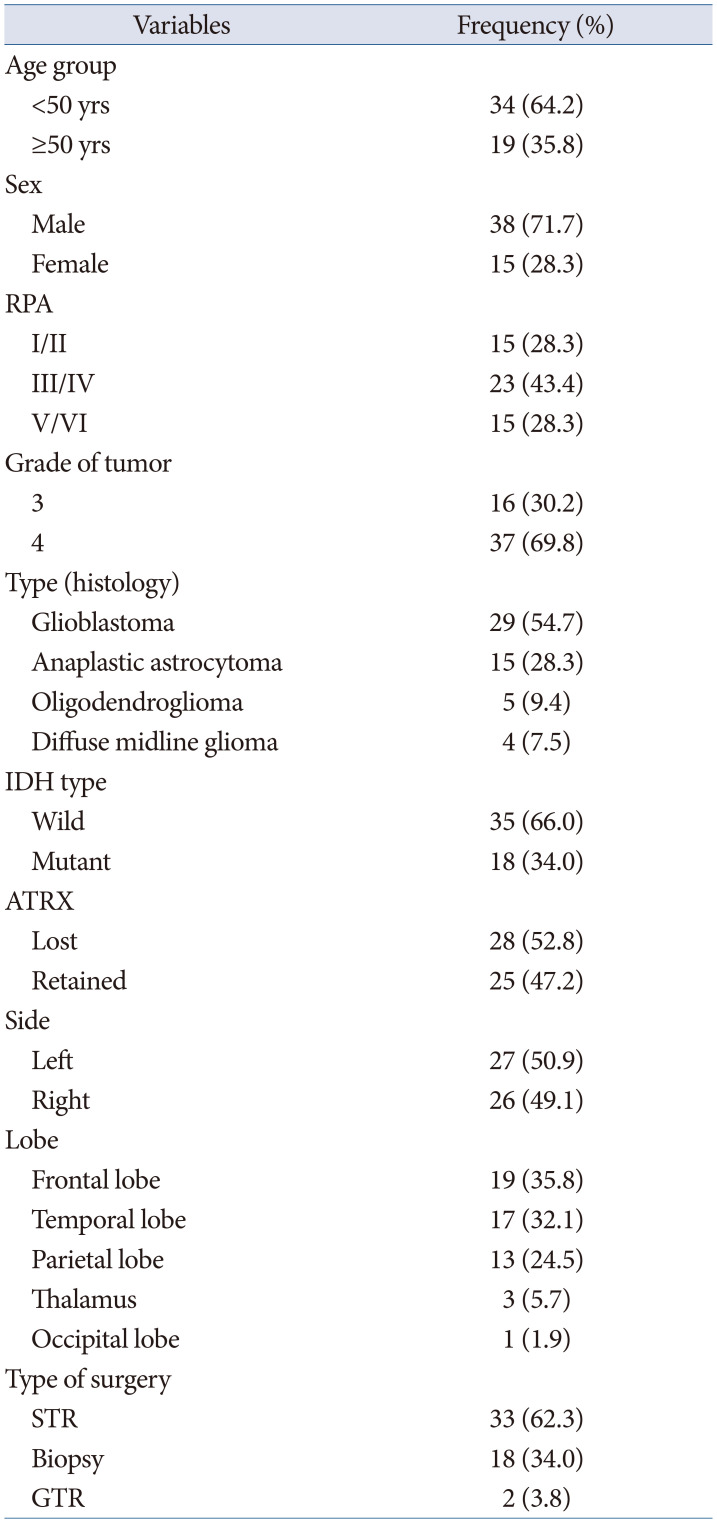
Table 1
Sociodemographic and clinical characteristics of the patients (n=53)
![]()
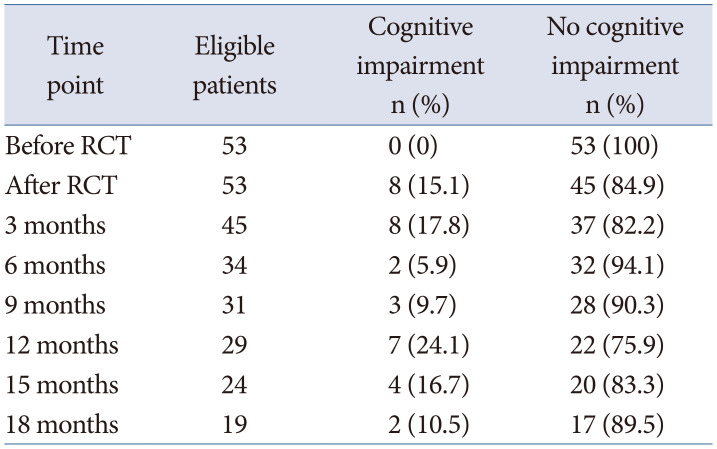
The number and percentage of patients with and without cognitive impairment at various time points of the study are shown in Table 2. All patients had normal cognitive function at baseline with MMSE scores between 26 to 30 and a mean (±SD) score of 28.92 (±1.67). The median follow-up duration with regards to assessment of cognitive function was 15 months (95% confidence interval [CI]: 6 to 18 months) in our study. At the end of last follow-up, the MMSE score in the remaining cohort of patients reduced to a mean (±SD) of 22.96 (±5.63). Considering the last follow-up of each study patient including those with disease progression and/or death, 30 (56.6%) had developed cognitive impairment while 23 patients (43.4%) did not. A total of 18 patients (34.0%) developed severe cognitive impairment (MMSE score 0–17) at various time points during the study. The probability of maintaining normal cognitive function at different time points from our study results is displayed in Fig. 2. Among patients surviving without disease progression on follow up, cognitive impairment was highest (31.8% of the cohort) at 12 months post-chemoradiation.
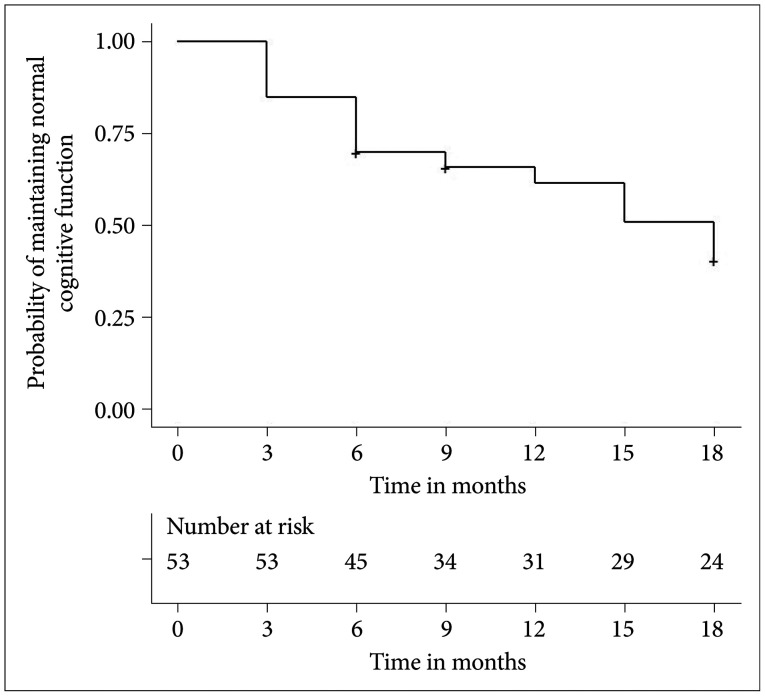 | Fig. 2Probability of maintaining normal cognitive function at different points in time for the study population.
|
Table 2
Characteristics of the study population
![]()
Table 3 shows the univariate and multivariable analysis in determining possible risk factors of cognitive impairment from our study results. On univariate analysis, RPA, grade of tumor, type (histology), IDH type, ATRX, and type of surgery were found to be significant predictors of cognitive impairment. The hazard of cognitive impairment increased by 3.77 times (95% CI: 1.36–10.45) in patients with RPA V/VI compared to patients with RPA I/II. The risk of cognitive impairment in patients with tumor grade 4 was 4.77 times (95% CI: 1.65–13.78) higher than in patients with grade 3 tumors. Glioblastoma and diffuse midline glioma histology patients were 8.20 times (95% CI: 2.40–27.99) and 5.85 times (95% CI: 1.29–26.48), respectively, more likely to develop cognitive impairment as compared to patients with anaplastic astrocytoma. The hazard of cognitive impairment increased by 4.70 times (95% CI: 1.77–12.48) in patients with IDH wild type compared to those with mutated IDH. The risk of cognitive impairment in patients with lost ATRX was 2.10 times (95% CI: 1.003–4.40) higher than those with retained ATRX. Patients who underwent biopsy only of their primary tumor were 2.73 times more likely to develop cognitive impairment, as opposed to the patients who underwent GTR and had a lower risk of such impairments. However, none of the variables were found to be significantly associated with NCF on multivariable analysis.
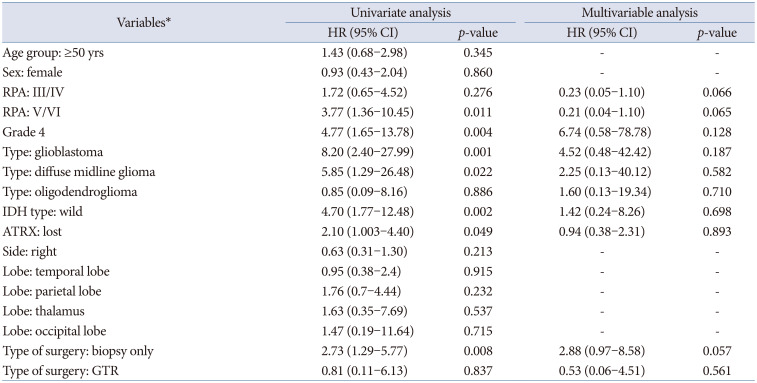
Table 3
Results of Cox univariate and multivariable regression analysis to determine factors for cognitive impairment in the study population
*Age <50 yrs, male sex, RPA I/II, grade 3, anaplastic astrocytoma, IDH mutant, ATRX retained, left-sided tumor, frontal lobe location, and STR were taken as the reference category for age group, sex, RPA, grade of tumor, type (histology), IDH type, ATRX, side, lobe, and type of surgery, respectively. HR, hazard ratio; CI, confidence interval; RPA, recursive partitioning analysis; IDH, isocitrate dehydrogenase; ATRX, alpha-thalassemia X-linked mental retardation; STR, subtotal resection; GTR, gross total resection
![]()
The PTV and corresponding hippocampus doses received by the study patients were analyzed and are depicted in Table 4. The mean PTV of patients having cognitive impairment was found to be significantly larger than those without cognitive impairment (p<0.05). Similarly, the mean of radiotherapy doses to ipsilateral (I/L) and contralateral (C/L) hippocampus, both minimum (Dmin) and maximum (Dmax) point doses, were found to be higher among patients with cognitive impairment compared to patients without cognitive impairment. However, the difference reached statistical significance correlating to cognitive impairment for the I/L hippocampus Dmin only (p<0.05).
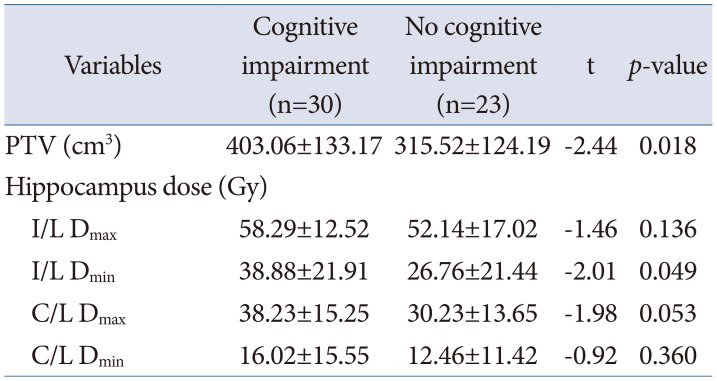
Table 4
Comparison of PTV and hippocampus doses between patients with and without cognitive impairment
![]()
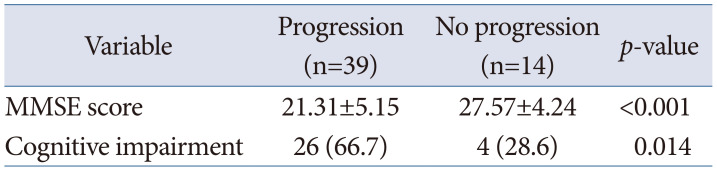
We also analyzed the correlation between treatment outcome and NCF in our cohort. Tumor progression status and its association with mean MMSE score and cognitive impairment was compared as depicted in Table 5. The mean (±SD) MMSE score was 21.31 (±5.15) among patients who had progression versus 27.57 (±4.24) among patients without progression (stable disease, partial or complete response). With regards to cognitive impairment, it was noticed in 66.7% patients with progression versus 28.6% patients without progression. Both variables demonstrated high statistical significance with tumor progression status (p<0.05).
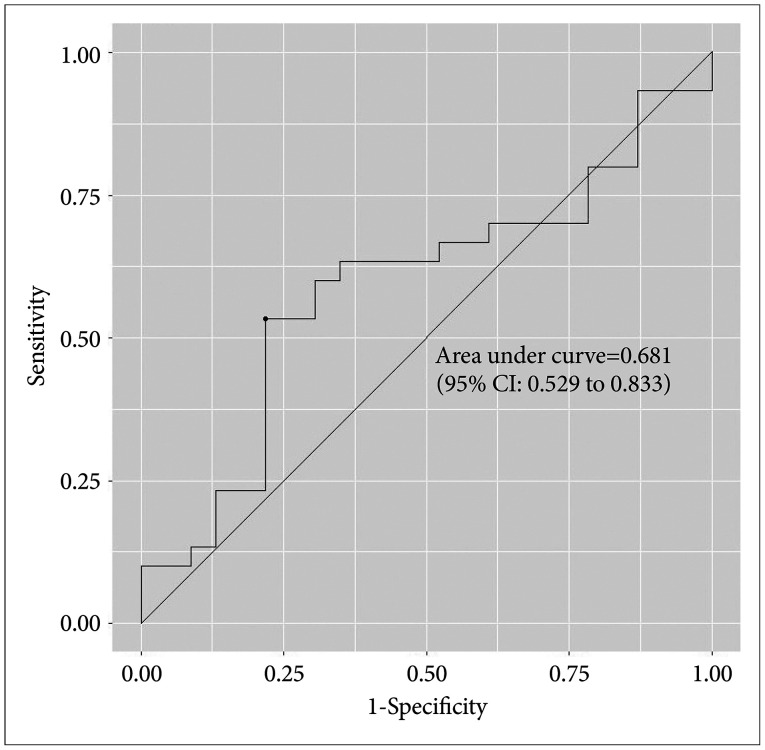
Finally, an ROC curve of the multivariable Cox regression model based on our study parameters for predictive accuracy of neurocognitive dysfunction was generated. The area under the curve was found to be 0.681 (95% CI 0.529–0.833), as shown in Fig. 3. Thus, prediction of NCFs in patients of HGG by a model based on our study results was found to be around 68.1% accurate.
Go to :
DISCUSSION
The current treatment approach for HGG patients is maximal safe resection of tumor followed by adjuvant chemoradiation (CRT) followed by maintenance chemotherapy [8]. CRT treatment is often believed to have a deleterious effect on the neurocognitive abilities of brain tumor patients. Radiation is associated with cerebral atrophy and alterations in white matter networks in patients who survive over a period of time [12]. A Cochrane Database systematic review on long-term neurocognitive side effects of radiation with or without chemotherapy in glioma patients, however, states that the magnitude of risk association is uncertain due to lack of definitive data [20]. They suggest that neurocognitive assessment should be an integral part of trials evaluating effect of treatment on glioma to improve the level of evidence. Most of the studies in this review included only patients of low-grade gliomas and only 2 studies were on grade 3 glioma patients with anaplastic oligodendroglioma and oligoastrocytoma histologies [2122]. Thus our study is one of the few to prospectively report the effects of radiation and chemotherapy treatment on the NCF of HGG patients, with nearly 70% of the cohort having grade 4 tumors.
Two randomized controlled studies have reported long-term outcomes of NCFs and quality of life in grade 3 glioma patients treated with CRT. Both these studies included patients treated in the European Organization for Research and Treatment of Cancer (EORTC)-26951 study and Radiation Therapy Oncology Group (RTOG)-9402 study [2122]. The EORTC analysis by Habets et al. [21] assessed cognition using neuropsychological tests for 6 domains in 37 long-term survivors of anaplastic oligodendroglioma and reported 30% incidence of severe cognitive impairment in the cohort. At a median survival of 147 months when reporting, no significant difference was noted in cognitive impairment of patients who received CRT versus RT alone. The RTOG study analyzed cognition using the MMSE scale and also found no difference in the cognitive decline between the treatment arms among anaplastic oligodendroglioma patients [22]. Younger, fitter patients had better MMSE scores which predicted for superior survival outcomes in this study.
Research has shown that there is considerable variation in levels of cognitive impairment experienced by patients of high-grade glioma vis-à-vis low-grade gliomas, which are attributable to the tumor grade itself. Miotto et al. [23] carried out a comparative analysis where glioma patients were accrued before surgery and their neurocognitive status evaluated. They found that 88% HGG patients showed reduced speed of information processing, executive functions, verbal and visual memory independently of the lesion location which was much higher than the low-grade glioma cohort. Thus, HGGs are inherently more susceptible to cause impaired NCF which may be further aggravated with CRT. Our results support these findings as GBM and diffuse glioma patients had inferior NCF compared to other histologies, on univariate analysis (Table 3). Wang et al. [24] analyzed effects of adjuvant CRT upon cognition in a prospective study of HGG patients with 43% of the cohort having GBM histology. Their results did not show any significant decline of NCF status assessed by MMSE during the treatment as well as follow-up period. Hilverda et al. [25] also showed that GBM patients who were progression free after postoperative CRT treatment did not show decline in NCF. Contrastingly, cognitive impairment occurred in 56.6% of our study participants following CRT during the follow-up period of 18 months. One reason for our results could be that, unlike Hilverda et al. [25], we did not include only the complete responders in the final analysis but also those with partial or no response to CRT. Hence their decline in NCF may have been attributable also to the disease pathology rather than only the CRT treatment. Also, our study has a comparatively longer follow-up (18 months) of patients when compared to these two studies (12 months and 6 months, respectively).
Meyers and Wefel [26] opined that MMSE as a screening technique of NCF might fail to detect modest cognitive alterations because it lacks the sensitivity to identify frontal-subcortical network disruption, which is frequently associated with radiation therapy in the brain. The Montreal Cognitive Assessment is advocated to be a tool with higher sensitivity and greater comprehensive coverage for detecting even mild decline in NCF and has been used in studies of HGG patients [2728]. However, it is dependent on the education levels of patients as it takes into account the years of education received and requires corrections to be made accordingly to eliminate bias. As illiteracy rates are very high among patients in our part of the world, we decided to implement the MMSE tool for our study, which is also a widely implemented NCF assessment tool [2224].
Although decline in NCF in glioma patients is multifactorial, the pathogenesis of radiotherapy-induced neurocognitive dysfunction is largely attributed to the vulnerability of proliferating neuronal progenitor cells in the subgranular zone of the hippocampi to radiation injury [2930]. Radiation exposure to hippocampus causes a long-term decrease in neurogenesis in the subgranular zone of adult rats and has also been linked to deficits in learning and memory in humans [3031]. We used VMAT technique for irradiating all our study patients and found a significant correlation of minimum dose received (Dmin) by ipsilateral hippocampus with development of neurocognitive impairment in the cohort. The threshold dose for hippocampi that can be safely delivered in glioma patients still remains unclear, but modern conformal radiotherapy techniques enable us to spare the hippocampi from high radiotherapy doses which holds promise for improving NCF. Rydelius et al. [32] have found that arc-based intensity modulated radiotherapy has less negative impact on cognitive function of malignant glioma patients.
With the trend of incorporating molecular and genetic markers into the classification and management of gliomas, newer risk factors have emerged which impact the NCF in these patients. In a large prospective analysis of 229 HGG patients receiving adjuvant CRT from China, Wang et al. [28] found that apart from known prognostic factors like GBM histology and residual tumor volume, unmethylated O6-methylguanine-DNA methyltransferase (MGMT) promoter status also negatively impacted NCF in an independent manner. MGMT is a DNA repair protein and its unmethylated status in the tumor cells is known to cause resistance to TMZ chemotherapy with poorer survival [33]. Similarly, IDH gene status in glioma patients is another prognostic factor. IDH wild-type (IDH-WT) gliomas have been associated with worse prognosis and shorter survival than IDH mutant (IDH-mut) [34]. A systematic review by Bunevicius et al. [35] now shows that IDH-WT gliomas are also associated with greater cognitive burden than IDH-mut tumors. Our study also found a significant positive association between declining NCF and IDH-WT tumors (HR: 4.70, 95% CI:1.77–12.48). However, we did not assess MGMT methylation status in our cohort due to logistic issues. With advancement of knowledge, more such molecular prognosticators may be revealed in upcoming days, that impact neurocognition in glioma patients.
Our study does not evaluate other parameters like anxiety, depression, and overall quality of life that may be impacted from CRT treatment in HGG patients. Also, it is limited by its short follow-up period. A longer follow-up of patients surviving without residual or recurrence will be required to eliminate the confounding factors of neurocognitive decline apart from CRT in our study cohort.
In conclusion, tumor histology (GBM and diffuse glioma), WHO grade 4, IDH wild type status, RPA class IV/V, unresectable tumors, radiotherapy PTV, and dose received by ipsilateral hippocampus have been found to be independent risk factors for cognitive impairment in HGG patients. Tumor progression, during or after CRT also adversely affects NCFs. Future large prospective studies on HGG must incorporate evaluation and reporting of NCFs of participating patients using standardized tools in a systematic manner. Genetic and molecular markers need to be explored for developing predictive risk models of neurocognitive decline in HGG patients treated with chemoradiation.
Go to :
 XML Download
XML Download