

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Glioblastoma (GBM) is the most common and malignant type of gliomas, characterized by a dismal prognosis. The primary treatment for GBM involves surgical resection followed by chemoradiation with temozolomide. However, despite these standard treatments, median survival remains at approximately 15–18 months [1]. When gross total resection (GTR) is achieved, patient survival may extend to 20–25 months [2].
For glioma resection, including GBM, the goal is to achieve complete removal of the tumor on T1-contrast enhanced (T1CE) MRI [34]. However, complete resection is challenging because gliomas deeply infiltrate the surrounding brain tissue. Additionally, cancer cells should have a density above a certain threshold to become visible on MRI, meaning that areas with lower cell densities may appear normal on MRI scans [56]. Autopsies of GBM have revealed cancer cells even in seemingly normal brain tissue on the opposite side [7]. Due to these invisible tumors on MRI, even after the removal of all visible lesions, residual tumors may still be present, necessitating chemotherapy and radiotherapy [18].
It may be expected that removing additional surrounding tissue would increase the removal of invisible lesions, but the brain hosts critical functions, and damaging these areas can significantly reduce the patient’s quality of life. Therefore, complete removal of the brain infiltrated by the tumor is not always a solution. Consequently, the surgical principle for brain gliomas is referred to as “maximal safe resection.” This principle aims to remove as much of the tumor as possible without worsening the patient’s symptoms, although there is no objective standard for determining the extent of maximal safe resection, leading to various interpretations depending on the surgeon.
The tumor regions that show enhancement on T1CE are typically the most malignant and densely populated with tumor cells [5]. These core tumor areas undergo angiogenesis, and the blood-brain barrier is destroyed, leading to contrast leakage and enhancement on MRI. High-grade gliomas, including GBM, often display enhancement in large portions of the tumor. In contrast, low-grade gliomas may show weak or no enhancement on T1CE and can be distinguished by high signal intensity on T2-weighted fluid-attenuated inversion recovery (T2-FLAIR) images.
While the extent of resection in GBM was evaluated based on T1CE, it was not applicable for low-grade gliomas, which often relied on T2 FLAIR lesions. However, the traditional concepts of low-grade and high-grade gliomas are being redefined depending on molecular alterations. In cases where cell density is low, there is no T1CE on imaging, and the pathology appears to be a low-grade glioma, molecular features of GBM may still be present, resulting in a poor prognosis. In such cases, T1CE tumors cannot serve as a standard for evaluating the extent of tumor resection. The criteria for determining the resection range of GBMs have become increasingly ambiguous, necessitating redefinition based on advances in molecular biology.
On the other hand, Yordanova et al. [9] suggested that removing a more extensive range of lesions visible on MRI in low-grade gliomas could result in improved prognosis and coined the term “supratotal resection” to contrast it with GTR (Duffau’s principle). However, this study was conducted before molecular classification and mostly included patients with a favorable prognosis, such as oligodendroglioma, limiting the evidence for survival improvement due to supratotal resection.
Duffau’s principle of supratotal resection states that resection should be “pursued beyond MR imaging abnormalities until corticosubcortical eloquent structures are encountered.” Applied literally, this would mean removing tissue up to the point where eloquent structures appear, even if they seem normal. However, it is unclear whether this principle is applicable to low-grade gliomas, and it has not yet been established whether it can be applied to GBMs.
Since Yordanova et al. [9] described “supratotal” resection, similar concepts have also been referred to as “supracomplete” [10], “supramaximal” [11121314], and “supramarginal” [15161718] resection. On the other hand, the term “supratotal” has also been used with a slightly different meaning. Esquenazi et al. [19] introduced a method of subpial resection of lesions visible on T1CE, which they referred to as supratotal resection. However, the extent of removal on T2-FLAIR and its impact on survival were not assessed in this study.
The term “supratotal” means being above the total. However, complete resection or microscopic total resection is nearly impossible in GBMs due to the lack of margin. Given this, the phrase “supramaximal” resection, which adheres to the maximization of safe resection, appears suitable. We will use this term in this paper, as the Response Assessment in Neuro-Oncology (RANO) group did [20]. Recently, there has been growing evidence suggesting that it is beneficial to remove lesions observed on T2-FLAIR in GBM as much as possible, and efforts have been made to classify this based on more objective criteria. In this review, we will examine the emerging consensus and newly defined criteria for the concept of “supramaximal resection” in GBMs concerning the extent of resection.
Go to : 
DANDY’S HEMISPHERECTOMY FOR GLIOMAS
Walter Dandy, a distinguished neurosurgeon who made significant contributions to pediatric neurosurgery, sought to treat gliomas through surgical intervention. With expertise in epilepsy surgery, which involved performing hemispherectomies to control seizures, particularly in pediatric patients, Dandy [21] applied this technique to patients with right hemispheric gliomas. This represented the first documented instance of supramaximal resection for gliomas.
During this period, neither MRI nor CT scans were available, making it difficult to precisely identify the tumors that were candidates for hemispherectomy. It is possible that the resected tumors may not meet the current diagnostic criteria for GBM. Among the five patients who underwent surgery, two died postoperatively, and another within three months. However, the remaining two patients reportedly survived for over 3.5 years. As no postoperative MRI was conducted at the time, the exact extent of the resection remains uncertain. Based on the data recovered by Dandy’s successors, the right frontal, temporal, and parietal lobes were resected, and the anterior cerebral arteries and middle cerebral arteries were ligated with clips. The right hemisphere’s basal ganglia and thalamus were preserved. All patients experienced left hemiplegia following the surgery [22].
Dandy’s attempt demonstrated that for gliomas located in the right hemisphere, extensive resection could be performed within the limits of maintaining a certain level of consciousness, albeit with some sacrifice of neurological function. At the same time, it implied that gliomas are diseases that cannot be cured by surgery alone.
Go to :
ASSOCIATION BETWEEN T2-BASED EXTENT OF RESECTION AND SURVIVAL IN LOW-GRADE GLIOMAS
For low-grade gliomas where the extent of resection cannot be determined based on T1CE, the extent of resection has traditionally been determined using T2-FLAIR as the reference [2324]. In 2018, a study involving 228 adult participants who underwent surgical treatment for supratentorial low-grade gliomas was published [23]. Pre- and postoperative tumor volumes were assessed using semiautomatic software on T2-weighted images, and targeted next-generation sequencing was employed to classify samples according to the 2016 World Health Organization (WHO) classification. The results indicated that postoperative volume was associated with overall survival (OS), with a hazard ratio of 1.01 per cm3 increase in volume. This association was especially pronounced in patients with isocitrate dehydrogenase (IDH) mutated astrocytoma, where even small postoperative volumes (0.1–5.0 cm3) negatively impacted OS. The study concluded that maximal resection should be the primary treatment for molecularly defined low-grade gliomas, and in IDH mutated astrocytoma, a second-look operation should be considered to remove minor residues if safely achievable to enhance OS.
In a separate study published in 2020, which focused on WHO grade 2 gliomas based on the 2016 criteria, it was demonstrated that cases with more than 99% removal based on T2-FLAIR had longer survival periods compared to those with less resection [25]. The benefit of the extent of resection in increasing survival was also reported for 1p/19q-codeleted oligodendrogliomas, which are based on molecular markers [25].
These studies were retrospective in nature, potentially introducing bias, and did not reflect the recently discovered molecular markers. Therefore, it is necessary to re-examine these findings according to the newly published 2021 WHO classification. Many tumors that were classified as low-grade in the WHO 2016 classification are now classified as molecular GBMs in the 2021 WHO Central Nervous System (CNS) 5 classification [14]. It is essential to re-establish the significance of the extent of resection for grade 2 gliomas based on the 2021 WHO CNS 5 criteria.
Go to :
ASSOCIATION BETWEEN EXTENT OF RESECTION AND SURVIVAL IN WHO GRADE 3 GLIOMAS
Grade 3 gliomas include tumors that exhibit enhancement and those that do not. In most studies, enhancing tumors were assessed based on T1CE, while non-enhancing tumors were evaluated using T2-FLAIR for determining the extent of resection [2627]. When examining the extent of resection for grade 3 gliomas based on the WHO CNS 4 criteria, an increase in extent of resection was found to be associated with increased survival [27]. For grade 3 gliomas according to the 2016 WHO classification, a larger survival difference was observed when assessing the extent of resection using T2-FLAIR compared to T1CE [28].
Go to :
ASSOCIATION BETWEEN EXTENT OF RESECTION AND SURVIVAL IN GBM PATIENTS
Extent of resection on T1CE MRI in GBMs
Studies investigating the survival benefit of the extent of resection in GBMs have primarily focused on T1CE [34]. When defining GTR as cases, where the tumor is not visible at all on T1CE, a significantly longer survival time was observed compared to cases with residual tumor, and differences in survival time were noted depending on the extent of remaining tumor even when complete resection could not be achieved [3]. Therefore, it can be concluded that maximizing tumor removal is helpful for improving survival even when GTR is not achievable. Notably, there was a considerable difference between the group with 98% removal and the group with 100% removal. This may be due to the inclusion of patients who had more than 100% removal based on T1CE criteria in the 100% removal group, implying that additional T2 lesions in the periphery were also removed in these patients. In another study, the median survival for patients with complete removal of T1CE lesions on postoperative MRI was approximately 27.9 months, which is longer than the previously known 15 months [2].
The association between the extent of resection on T1CE and longer survival has been somewhat established, but the results must be interpreted cautiously. Studies conducted before the discovery of IDH mutant gliomas in 2009 and the introduction of the molecular classification-based WHO classification in 2016 might have had a higher likelihood of including predominantly IDH-mutant tumors, which are more likely to undergo complete resection, in the GTR group [24].
However, even after the 2016 WHO classification, consistent results have been reported regarding the impact of T1CE extent of resection on survival. These findings confirm the close relationship between T1CE GTR and increased survival in a homogenous group of patients, including only IDH-wildtype GBM.
Extent of resection on T2-FLAIR in GBMs
Reports have been published regarding the association between T2-FLAIR extent of resection and survival duration in patients with GBM who underwent complete removal on T1CE. Pessina et al. [29] reported that among 282 GBM patients with complete tumor removal on T1CE, 21 patients with complete lesion removal on T2-FLAIR had better survival duration than the group with remaining T2-FLAIR lesions. Additionally, those with more than 45% of the lesion removed on T2-FLAIR had longer survival duration compared to those with less removal (24.5 months vs. 15.7 months). Li et al. [30] analyzed the T2-FLAIR extent of resection in 643 of 1,229 GBM patients who underwent T1CE GTR. When divided into two groups with a 53.21% cut-off, it was observed that the group with less than 53.21% removal had a survival duration of 15.5 months, while the group with more than 53.21% removal had a survival duration of 20.7 months.
These findings were confirmed before the release of the 2021 CNS WHO 5, predominantly including histologically diagnosed GBM and some IDH-mutant GBMs. According to current standards, those study population included non-GBMs and excluded molecular GBMs that appeared as low-grade gliomas in MRI.
Systematic reviews on supramaximal resection of GBMs
Meta-analyses and systematic reviews examining the survival benefit of supratotal or supramaximal resection in GBM have largely shown that patients who undergo supratotal or supramaximal resection have longer progression-free survival (PFS) and OS compared to those who undergo GTR. Moreover, these studies have demonstrated that the complication rate associated with supratotal resection is not significantly higher than that associated with GTR (Table 1) [12173132].
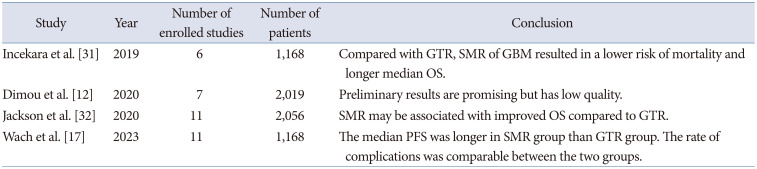
Table 1
Recent publications of systematic review and meta-analysis regarding supramaximal resection in GBMs
| Class | Year | Number of enrolled studies | Number of patients | Conclusion |
|---|---|---|---|---|
| Incekara et al. [31] | 2019 | 6 | 1,168 | Compared with GTR, SMR of GBM resulted in a lower risk of mortality and longer median OS. |
| Dimou et al. [12] | 2020 | 7 | 2,019 | Preliminary results are promising but has low quality. |
| Jackson et al. [32] | 2020 | 11 | 2,056 | SMR may be associated with improved OS compared to GTR. |
| Wach et al. [17] | 2023 | 11 | 1,168 | The median PFS was longer in SMR group than GTR group. The rate of complications was comparable between the two groups. |
![]()
Postoperative tumor residual volume or proportion compared to preoperative tumor volume
Many previous studies have focused on the proportion of the tumor removed relative to the total tumor size. However, in the case of GBM, there are cases where the T2 lesion is not much larger than the T1CE lesion, and there are also cases where the opposite is true. Additionally, the overall size of the tumor can vary significantly. For a tumor that is 100 cm3 in size, 1 cm3 accounts for only 1%, while for a 10 cm3 tumor, 1 cm3 corresponds to 10% [20]. Tripathi et al. [16] showed that, for tumors with relatively larger T2 lesions compared to T1, a more extensive removal of T2 lesions is necessary. Instead of using a complex method of assessing the relative size of the remaining tumor compared to the preoperative size, simply looking at the absolute size of the remaining tumor postoperatively can effectively reflect the prognosis. There is an advantage in knowing the absolute size of the remaining tumor, as it does not require knowledge of the preoperative tumor size, which is necessary when determining the proportion of the remaining tumor.
Go to :
RANO RESECT GROUP CLASSIFICATION FOR EXTENT OF RESECTION
The RANO resect group aimed to unify the definition of extent of resection used in different clinical trials by retrospectively analyzing 744 patients who met the WHO 2021 criteria for GBM and received chemoradiation. These patients were selected from the databases of seven institutions in Europe and the United States. The study found that the absolute size of the remaining contrast-enhanced (CE) tumor showed a significant difference in survival rates, and they investigated which measurement better reflected the prognosis [20].
By standardizing the definition of extent of resection, the RANO resect group has contributed to more consistent and comparable results in clinical trials, ultimately improving the understanding of the impact of extent of resection on GBM patients’ outcomes. Such efforts in the research community can help guide the development of more effective treatment strategies and improve patient prognosis.
Patients who underwent “maximal CE resection” (class 2) had better outcomes than patients with “submaximal CE resection” (class 3) or “biopsy,” which had lower absolute remaining tumor volumes (in cm3) (class 4). To define class 1 (“supramaximal CE resection”), extensive excision of non-CE tumor (5 cm3 residual non-CE tumor) was linked to improved survival among patients with complete CE resection (Fig. 1). After correcting for molecular and clinical variables, multivariate analysis maintained the prognostic significance of the resection classes (Table 2) [20].

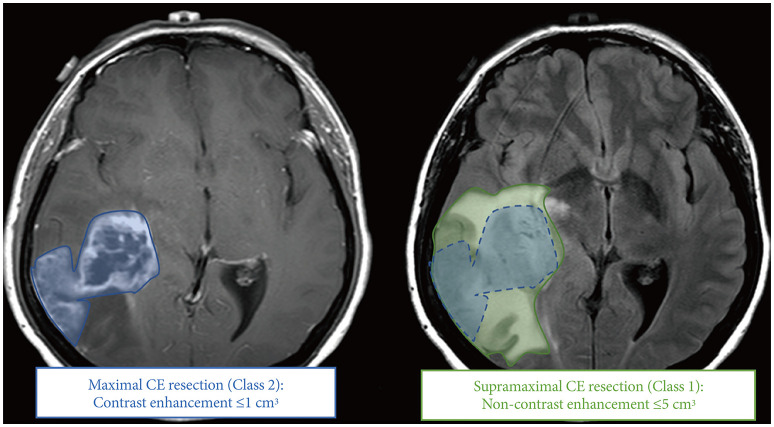 | Fig. 1Scheme of supramaximal resection of GBM based on RANO resect group criteria. Maximal CE resection (blue) requires less than 1 cm3 of residual contrast-enhanced lesion. Complete CE resection means the absence of a residual contrast-enhanced lesion. It is a subset of maximal CE resection (Class 2). Supramaximal CE resection (green) requires fulfilling Class 2 criteria plus less than 5 cm3 of noncontrast-enhanced lesion.
|
Table 2
RANO categories for extent of resection in GBM
RANO, Response Assessment in Neuro-Oncology; GBM, glioblastoma; CE, contrast-enhancement; nCE, non-contrast-enhancement; CI, confidence interval. Adapted from Karschnia et al. Neuro Oncol 2023;25:940-54, under the Creative Commons License (CC-BY-NC) [20].
![]()
Go to :
STRATEGIES FOR SUPRAMAXIMAL RESECTION
Role of 5-aminoleuvelinic acid for resection of GBMs
5-Aminolevulinic acid (5-ALA) is a fluorescent dye that is used during surgery to aid in the resection of GBMs. The use of 5-ALA has been shown to improve the extent of tumor resection in GBM patients, as it enables the detection and removal of small, non-enhancing tumor foci that would be difficult to identify using conventional radiologic techniques [1033]. Moreover, several clinical trials have demonstrated that 5-ALA-guided surgery results in longer PFS and OS in patients with GBM [34]. Therefore, 5-ALA has become an important tool for neurosurgeons in the supramaximal resection of GBMs.
Lobectomy as a supramaximal resection
In the case of GBMs located in specific areas, performing supramaximal resection can be relatively feasible, as seen in Dandy’s example [21] mentioned earlier. This is predominantly true for tumors in the non-dominant hemisphere, typically the right hemisphere. The rationale behind performing a lobectomy is to remove the tumor and its surrounding area as much as possible, thereby reducing the tumor burden from potential infiltration. Roh et al. [35] demonstrated significant differences in PFS and OS when performing lobectomy for GBMs in the right frontal and temporal lobes compared to cases where GTR was performed without lobectomy, despite similar extents of tumor (PFS: 11.5 months vs. 30.7 months; OS: 18.7 months vs. 44.1 months). Studies from other groups, employing the same design, have reported significant differences in PFS and OS when including only temporal lobe GBMs [36]. Similarly, when involving GBMs that arose in the occipital lobe, the addition of lobectomy has been reported to be associated with longer PFS and OS [3738].
Supramaximal resection for GBMs in eloquent area
Due to the infiltrative nature of gliomas, it has been argued that the supramaximal removal of these tumors may impair patients’ performance and yield unfavorable outcomes. This is particularly true when the tumor is located near an eloquent area, where supramaximal removal can be challenging.
However, recent research analyzing 3,919 glioma patients with tumors located in eloquent areas across four centers has reported that the survival period is longer when an awake craniotomy is performed (17 months; n=134) as compared to asleep resection (14 months; n=402) [39]. This is likely attributed to a higher extent of resection achieved during awake craniotomy. Furthermore, subsequent studies have demonstrated that in patients under 70 years of age with a preoperative performance score of 90 or above, awake surgery allows for both maximum resection and preservation of neurological function [40].
Research has also been conducted on the feasibility of supramaximal resection for GBMs arising in the dominant hemisphere. Di et al. [11] have reported that supramaximal resection can be achieved for left-sided GBMs through awake surgery and that survival periods are increased when maximal resection is achieved, as observed on FLAIR imaging.
Conclusions and future directions
In summary, based on the 2021 WHO CNS 5 criteria, it appears that for GBMs (those defined as IDH-wildtype by this classification), the removal of CE tumor followed by additional removal of non-CE tumor is beneficial in terms of patient survival. However, the level of evidence provided by these studies is not very high, as they are all retrospective in nature, except for one prospective study. Due to the characteristics of surgical treatment, it is anticipated that conducting randomized controlled trials will be challenging in the future. Furthermore, these results should not be overinterpreted. While the utility of additional non-CE tumor resection has been substantiated for typical GBMs as per the 2021 WHO criteria, the same cannot be applied to other types of gliomas.
In the future, it is expected that research employing artificial intelligence for the automatic analysis of resection boundaries will become more active, allowing for a more objective assessment of the extent of resection. This will enable further stratification of patients and determination of the optimal degree of tumor removal for each specific case. Consequently, it is anticipated that personalized treatment tailored to individual patients will become increasingly possible.
Go to :
 XML Download
XML Download