

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease (COVID-19) pandemic, which began at the end of 2019, has become a prolonged global event with no prior precedent. The healthcare system faced numerous crises that threatened to overload existing medical systems, leading to a sudden increase in demand for COVID-19 treatments, a shortage of medical resources, and a temporary disruption in the provision of care for patients with other illnesses. Brain tumor patients were not exempt from these difficulties, and healthcare professionals struggled to provide adequate management under these resource-constrained conditions. However, providing effective management for patients in a crisis without proper guidelines can be difficult.
In response to this, the Korean Society for Neuro-Oncology (KSNO), a multidisciplinary academic society, has developed specialized clinical guidelines for brain tumor patient care during a crisis. As part II of the guideline, this consensus survey was conducted to provide appropriate management options in specific clinical situations during the crisis period. The crisis period is defined as a situation in which medical resources for the management of brain tumor patients are restricted because of various causes, such as natural disasters, infectious diseases, and wars, making it impossible to proceed with management as usual. This survey addresses the following five types of brain tumors: newly diagnosed astrocytoma with isocitrate dehydrogenase (IDH)-mutant type, newly diagnosed oligodendroglioma with both IDH-mutant and 1p19q co-deletion, newly diagnosed glioblastoma, newly developed symptomatic brain metastases, and newly diagnosed atypical meningioma.
METHODS
The details of the survey design, outline, and implementation are described in the previous article of the series in this issue. In the current consensus survey, we investigated appropriate management options in five specific clinical scenarios during the crisis period. Scenario 1 was designed to evaluate the appropriate management option considering Karnofsky Performance Scale (KPS) and risk in the newly diagnosed astrocytoma with IDH-mutant type during the crisis period. Scenario 2 was a survey about the appropriate treatment strategy considering KPS and risk in the newly diagnosed oligodendroglioma with both IDH-mutant and 1p19q co-deletion during the crisis period. Scenario 3 aimed to investigate appropriate adjuvant treatment and radiotherapy schedules considering age, KPS, the extent of resection, and methylation status of the O6-methylguanine-DNA methyltransferase (MGMT) promoter in the newly diagnosed glioblastoma during the crisis period. Scenario 4 aimed to select an appropriate radiotherapy strategy considering KPS and the number of brain metastases in newly developed symptomatic brain metastases during the crisis period. Lastly, Scenario 5 concerned appropriate adjuvant management and radiotherapy schedule in the newly diagnosed atypical meningioma during the crisis period. All questionnaires regarding the five clinical scenarios are presented in the Supplementary Material (in the online-only Data Supplement).
RESULTS
Newly diagnosed astrocytoma, IDH-mutant
For patients with World Health Organization (WHO) grade 2, KPS ≥60, and low risk, the majority of responses (85.7%) favored observation. For patients with WHO grade 2, KPS ≥60, and high risk, radiotherapy alone was the preferred treatment for 81% of responses, while radiotherapy with adjuvant PCV (procarbazine, lomustine, and vincristine) or radiotherapy with concurrent and adjuvant temozolomide (TMZ) each were preferred by 4.8%. For patients with WHO grade 3 or 4 and KPS ≥60, radiotherapy with concurrent and adjuvant TMZ was the most favored treatment, with 42.9% of responses. Radiotherapy with adjuvant TMZ was the second most favored with 38.1% of responses, followed by radiotherapy with adjuvant PCV with 14.3% of responses. For patients with KPS <60 regardless of WHO grade, best supportive care alone was favored by 66.7% of responses. Table 1 shows the summary of responses regarding treatment for patients newly diagnosed with astrocytoma, IDH-mutant during the crisis period.
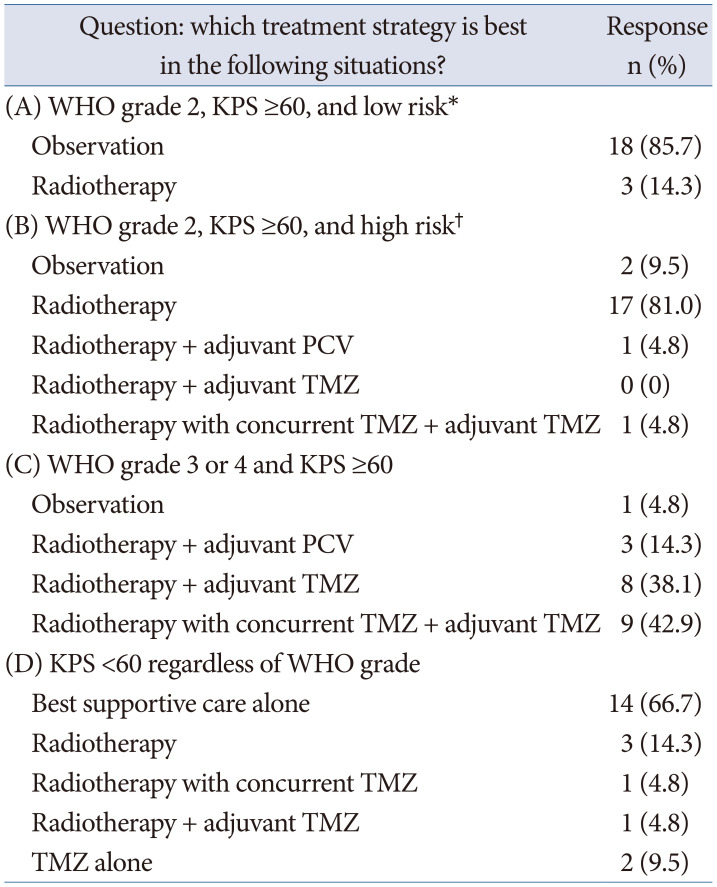
Table 1
Summary of responses regarding treatment for patients newly diagnosed with astrocytoma, IDH-mutant during the crisis period
![]()
Newly diagnosed oligodendroglioma, IDH-mutant and 1p19q codeleted
For patients with WHO grade 2 and KPS ≥60, the majority (90.5%) chose observation as the best treatment strategy in low-risk cases, while radiotherapy was selected by 9.5%. In high-risk cases, the majority (57.1%) chose radiotherapy alone, while 23.8% chose radiotherapy with adjuvant PCV, 4.8% chose radiotherapy with concurrent and adjuvant TMZ, and only 14.3% chose observation. For patients with WHO grade 3 and KPS ≥60, the majority (81%) chose radiotherapy with neoadjuvant or adjuvant PCV, 9.5% chose radiotherapy with adjuvant TMZ, 4.8% chose radiotherapy with concurrent and adjuvant TMZ, and only 4.8% chose observation. For patients with KPS <60 regardless of WHO grade, the majority (71.4%) chose best supportive care alone, 14.3% chose radiotherapy alone, 4.8% chose radiotherapy with concurrent TMZ, 4.8% chose radiotherapy with adjuvant TMZ, and only 4.8% chose TMZ alone. The summary of responses regarding treatment for patients newly diagnosed with oligodendroglioma and IDH-mutant 1p19q codeleted is presented in Table 2.
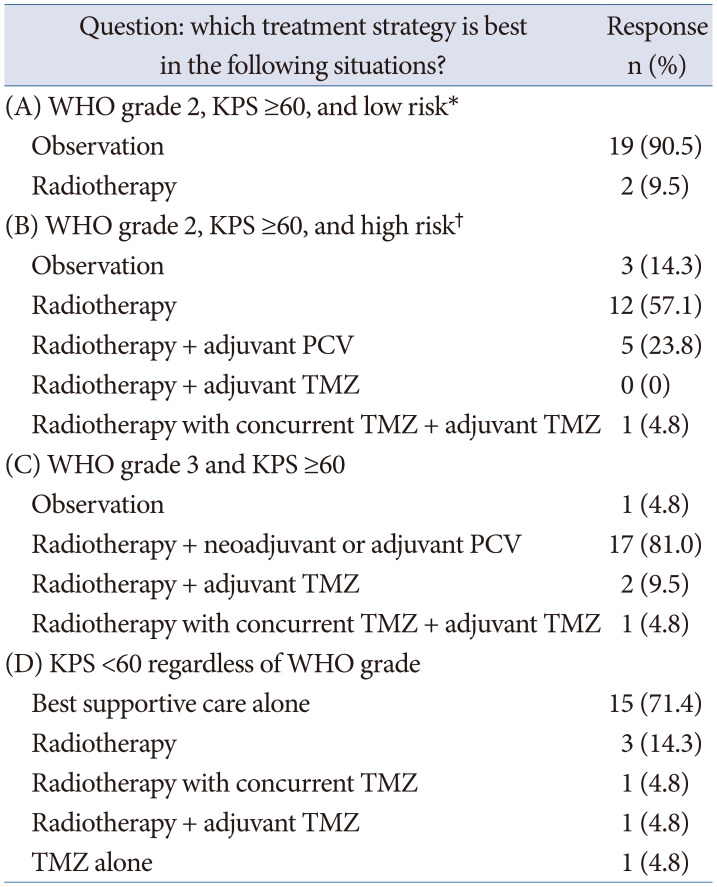
Table 2
Summary of responses regarding treatment for patients newly diagnosed with oligodendroglioma, IDH-mutant and 1p19q codeleted during the crisis period
![]()
Newly diagnosed glioblastoma
Sixteen potential clinical scenarios of newly diagnosed glioblastoma based on age (64 vs. 76 years), KPS (90 vs. 60 points), extent of resection (gross total resection vs. partial resection), and methylation status of the MGMT promoter (methylated vs. unmethylated) were created. Expert panels were required to answer the most appropriate adjuvant treatment combination (best supportive care, radiotherapy alone, radiotherapy plus TMZ, or TMZ alone) and radiotherapy dose-fractionation (60 Gy in 30 fractions, 40 Gy in 15 fractions, 34 Gy in 10 fractions, or 25 Gy in 5 fractions) during the crisis period with shortage of healthcare resource.
The most frequently answered treatment combination and radiotherapy dose per scenario is summarized in Table 3. Combination of radiotherapy plus TMZ was the preferred adjuvant treatment method in almost all case-scenarios (87.5%, 14/16). Radiotherapy alone was the preferred regimen only in patients aged 76 years with KPS of 60 points and unmethylated MGMT promoters. Interestingly, in no case-scenario was TMZ alone the preferred adjuvant treatment combination. In patients aged 64 years with KPS of 90 points, 60 Gy in 30 fractions was the most preferred radiotherapy regimen despite the shortage of resources during the crisis period. However, besides those patients, 40 Gy in 15 fractions was the most preferred regimen.
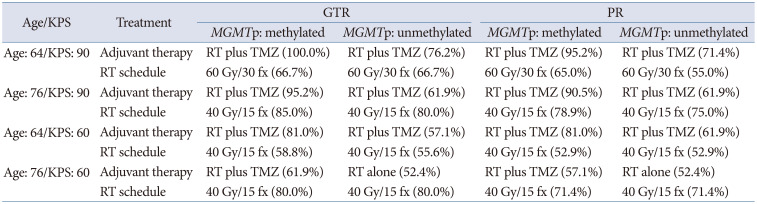
Table 3
Most frequently answered adjuvant treatment and radiotherapy dose-fractionation schedule per case-scenario in newly diagnosed glioblastoma during the crisis period
![]()
Newly diagnosed symptomatic brain metastases
Based on performance status (KPS 70 vs. 40) and number of brain metastases (3 vs. 10), four case-scenarios were developed, and expert panels answered the survey on the most appropriate radiotherapy type (radiosurgery, whole brain radiotherapy, or best supportive care) and whole brain radiotherapy dose-fractionation during the crisis period for each case (Table 4). For patients with 3 brain metastases, no panel recommended whole brain radiotherapy during the crisis period. In contrast, in patients with 10 brain metastases, whole brain
radiotherapy (76.2%) and best supportive care (61.9%) was the preferred treatment in patients with KPS 70 and KPS 40, respectively. Despite the shortage of medical resources, the most preferred whole brain radiotherapy regimen was 30 Gy in 10 fractions (66.6%) over 20 Gy in 5 fractions (33.3%) in patients with 10 brain metastases and KPS of 70.
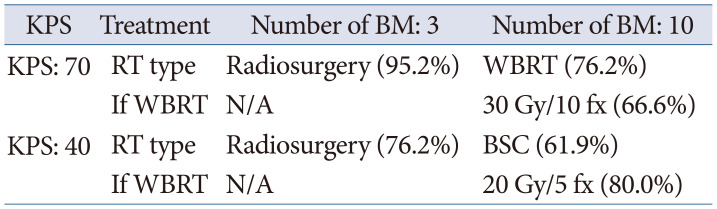
Table 4
Most frequently answered radiotherapy strategy per case-scenario in newly developed symptomatic brain metastasis during the crisis period
![]()
Newly diagnosed atypical meningioma
Similarly, based on age (57 vs. 82 years), KPS (90 vs. 60), extent of resection (gross total resection vs. subtotal/partial resection), and mitotic count, 16 clinical scenarios were proposed for patients with newly diagnosed atypical meningioma. The optimal adjuvant treatment (surveillance, conventional radiotherapy, or radiosurgery) and radiotherapy dose-fractionation (60 Gy in 30 fractions, 54 Gy in 30 fractions, or other) in case of conventional radiotherapy during the crisis period were surveyed (Table 5). For 82-year-old patients who underwent gross total resection, surveillance was the most preferred treatment regardless of mitotic count or KPS. In case of conventional radiotherapy, 54 Gy in 30 fractions was the most preferred regimen in most scenarios (Table 5).
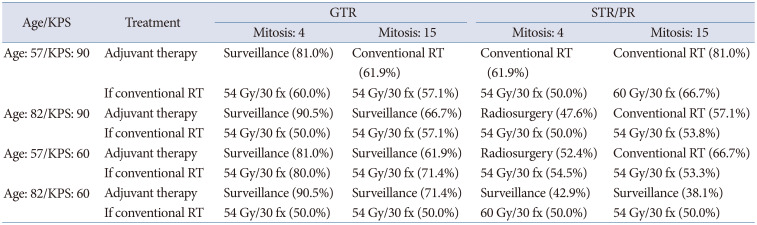
Table 5
Most frequently answered adjuvant treatment and radiotherapy dose-fractionation schedule per case-scenario in newly diagnosed atypical meningioma during the crisis period
![]()
DISCUSSION
Newly diagnosed astrocytoma, IDH-mutant and oligodendroglioma, IDH-mutant and 1p19q codeleted
The majority of the panel agreed that a more conservative approach to treatment is suitable for patients newly diagnosed with WHO grade 2 astrocytoma and oligodendroglioma during the crisis period. The EORTC 22845 trial demonstrated that early radiotherapy after surgery improved progression-free survival by two years compared to deferred radiotherapy until progression in patients with low-grade astrocytoma and oligodendroglioma with KPS ≥60, but did not affect overall survival [1]. The panel mostly agreed that this conservative strategy should be maintained for patients with low-risk IDH-mutant astrocytoma and low-risk IDH-mutant, 1p19q codeleted oligodendroglioma during the crisis period. However, in cases of WHO grade 2 astrocytoma and oligodendroglioma with high risk, particularly those with IDH mutations, radiotherapy with adjuvant PCV was found to have superior progression-free and overall survival compared to radiotherapy alone after surgery [2]. For these high-risk patients, the National Comprehensive Cancer Network (NCCN) guideline suggests using radiotherapy with adjuvant PCV as a category 1 recommendation during non-crisis periods [3]. Nevertheless, the panel did not believe that the addition of adjuvant PCV would have the same degree of benefit during the crisis period. The PCV regimen has a more toxic profile and requires more frequent hospital visits for intravenous vincristine administration and a multiple-dose oral medication schedule [45]. The panel expressed concern that the chemotherapy schedule and management of its adverse effects may be impacted by the crisis situation.
The panel had varying preferences for postoperative treatment strategies between patients with grade 3 oligodendroglioma, IDH-mutant/1p19q codeleted and grade 3 or 4 astrocytoma, IDH-mutant who have KPS ≥60. For patients with grade 3 oligodendroglioma, IDH-mutant/1p19q codeleted, the panel strongly recommended radiotherapy with adjuvant PCV, which is suggested as a preferred option in the national guidelines in the non-crisis period [36]. This recommendation is based on the findings of RTOG 9402 and EORTC 26951 trials, which demonstrate the substantial improvement in overall survival for patients with 1p19q codeleted oligodendroglioma who receive radiotherapy with adjuvant PCV compared to those who receive adjuvant radiotherapy alone [47]. With a median overall survival of 14.7 years and a nearly 50% reduced risk of death, respectively, these results provide strong evidence for the superiority of radiotherapy with adjuvant PCV over adjuvant radiotherapy alone. Even during the crisis period, which tends to favor more conservative treatment strategy, the panel agreed that the remarkable survival benefit seen with radiotherapy with adjuvant PCV justifies its use in these patients. Although the CODEL trial which compare radiotherapy with adjuvant PCV to radiotherapy with concurrent and adjuvant TMZ for grade 3 oligodendroglioma is ongoing, its result is still immature [8]. In contrast, the panel did not favor radiotherapy with adjuvant PCV as the postoperative treatment strategy for patients with grade 3 or 4 astrocytoma, IDH-mutant. A large retrospective study showed that while radiotherapy with adjuvant PCV improved progression-free survival compared to concurrent and adjuvant TMZ, it did not improve overall survival and was associated with a higher frequency of grade 3 or greater toxicity [9]. The results of the interim analysis of the CANTON trial, which evaluated TMZ-based treatment in patients with grade 3 IDH-mutant/1p19q non-codeleted astrocytoma showed that compared to adjuvant radiotherapy alone, radiotherapy with adjuvant TMZ significantly improved overall survival with a hazard ratio of 0.48 [10]. Despite the interim nature of the results, the panel considered radiotherapy with adjuvant TMZ with or without concurrent TMZ to be the preferred option for patients with grade 3 IDH-mutant/1p19q non-deleted astrocytoma during the crisis period, given the lower toxicity profile compared to the PCV regimen and the promising results from the CANTON trial. However, the panel was unable to conclude whether the addition of concurrent TMZ to adjuvant TMZ further improves outcomes for this cohort. As such, the panel made a weak recommendation for radiotherapy with concurrent and adjuvant TMZ for this cohort during the crisis period. During the non-crisis period, the NCCN guideline indicates a uniform consensus favoring either radiotherapy with concurrent and adjuvant TMZ or radiotherapy with adjuvant TMZ, based upon lower-level evidence [3]. For patients with KPS <60, the panel highly recommended best supportive care alone as the preferred option, followed by adjuvant radiotherapy alone, given the rarity of randomized studies in this cohort and the crisis situation.
Newly diagnosed glioblastoma
In the current survey for the optimal adjuvant treatment and radiotherapy dose-fractionation schedule in newly diagnosed glioblastoma during crisis period, radiotherapy plus TMZ and radiotherapy of 40 Gy in 15 fractions were the most preferred treatment in most scenarios. Of note, despite the shortage of radiotherapy resources, conventionally fractionated standard radiotherapy of 60 Gy in 30 fractions was the most preferred regimen in 64-year-old patients with good performance status regardless of extent of resection and methylation status of the MGMT promoter. Additionally, despite the presence of published NOA-08 and Nordic trials where TMZ alone was proven to be potentially equivalent to radiotherapy alone (60 Gy in 30 fractions) [1112], TMZ alone was not the preferred adjuvant treatment even in patients aged over 70 years with KPS 60 and methylated MGMT promoter.
The most preferred hypofractionated radiotherapy regimen during crisis was 40 Gy in 15 fractions which reflects the seldom usage of 34 Gy in 10 fractions and 25 Gy in 5 fractions in Korea, similar to the limited worldwide experience in Europe and USA [13]. Compared to the results of the KROG 21-05 survey study in elderly patients with newly diagnosed glioblastoma where 60 Gy in 30 fractions was the most preferred regimen except for 75-year-old patients with KPS of 60 [14], in the current survey assuming a crisis setting with shortage of radiotherapy resources, the utilization of conventionally fractionated standard radiotherapy was lower. Although the international expert guideline published by Bernhardt et al. [13] recommends hypofractionated radiotherapy in 3 weeks even for favorable patients (young age and good performance status) with glioblastoma during the crisis phase of COVID-19, our expert panels preferred conventionally fractionated radiotherapy in 6 weeks for these favorable patients. In contrast, in patients aged over 70 years or with poor performance status, it seems that a higher portion of physicians prefer an abbreviated course of radiotherapy during the crisis period compared to usual practice which was observed in the KROG 21-05 study [12]. This is probably because only a few retrospective studies support the use of conventionally fractionated standard radiotherapy in elderly patients with newly diagnosed glioblastoma [15]. However, since the respondents were not identical, these results should be interpreted with caution.
Newly diagnosed symptomatic brain metastases
In the current survey on symptomatic brain metastases during crisis, radiosurgery was the most preferred treatment in patients with limited number of metastases recommended by the EANO–ESMO Clinical Practice Guidelines and the ASCO-SNO-ASTRO Guideline [1617]. Of note, despite the shortage of medical resources, 30 Gy in 10 fractions was preferred over 20 Gy in 5 fractions for whole brain radiotherapy in patients with 10 brain metastases and KPS of 70. Although 1-week whole brain radiotherapy is widely used in the clinic [1618], physicians seem to prefer a potentially better intracranial disease control with higher doses even in the crisis setting [19].
Newly diagnosed atypical meningioma
During the COVID-19 pandemic, some groups have suggested that even elective surgery for meningiomas can be postponed in case of shortage in medical resources [20]. In our survey, most respondents chose surveillance as the preferred adjuvant strategy during the crisis period in patients with newly diagnosed atypical meningioma for cases where the tumor is completely resected and the mitotic count is low (Table 5), which is a considerable option according to international practice guidelines [2122]. Furthermore, for 82-year-old elderly patients, most respondents also recommended surveillance after gross total resection. This is probably due to the relatively high local control around 70% at 5 years [23], and the consideration of the shortage of medical resources. In contrast, despite the shortage of radiotherapy resources, most respondents chose to proceed with adjuvant radiotherapy in patients with completely resected tumor but high mitotic counts.
Although 54 Gy in 30 fractions was the most preferred radiotherapy dose-fractionation schedule, a similar portion of respondents also chose 60 Gy in 30 fractions (results not shown). Both regimens are recommended by published guidelines [2122]. However, despite the shortage of radiotherapy resources during the crisis period, only 1 respondent chose hypofractionated radiotherapy in 2 case-scenarios. Since short-course hypofractionated radiotherapy and radiotherapy doses under 50 Gy result in poor disease control in grade 2 or 3 meningiomas [2425], and most neuro-oncologists have limited experience in utilizing short-course hypofractionated radiotherapy in atypical meningiomas, our expert panel concluded 54–60 Gy as the optimal radiotherapy dose even in the crisis period as for non-crisis clinical settings.
Conclusions
The results of this survey could be a useful resource for the treatment of brain tumor patients in crisis situations that could cause shortages of medical resources, such as COVID-19, which may occur again in the future. Even in the midst of crisis situations, it remains imperative to endeavor towards providing optimal treatment modalities that may enhance patient survival rates and maximize their quality of life.
 XML Download
XML Download