

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chondrosarcomas are a group of neoplasms comprised of tumors cells that produce a cartilage matrix [1]. They have an annual incidence of approximately 1 per 200,000 [2], and the majority (83%) are low grade [2]. Metastases occur in 10%–21% of grade II and 60%–71% of grade III chondrosarcomas, most commonly to the lung [34]. The 5-year overall survival of patients who develop metastatic chondrosarcoma is 28.6% [5].
While 1%–8% of all sarcoma patients develop brain metastases [6], intracranial metastasis in chondrosarcoma is exceedingly rare. A prior review reported only 9 cases of chondrosarcoma brain metastases [7]. Large retrospective reviews estimate that chondrosarcoma metastatic to the brain accounts for 0.0%–5.6% of sarcoma patients with brain metastases [8910111213], 0.0%–0.24% of all sarcoma patients [6891314], and 0.17% of brain metastases [15]. A 6-year surveillance, epidemiology, and end results (SEER) analysis found only 3 out of 1,533 chondrosarcoma patients had brain metastases (0.2%) [16]. These prior retrospective studies each enfold just a few chondrosarcoma patients into a larger analysis of sarcomas without chondrosarcoma subset analysis [6891011121314]. Consequently, the nature of chondrosarcoma metastatic to the brain is poorly understood.
In this paper, we report a case of 66-year-old male patient with Maffucci syndrome who developed a cerebral chondrosarcoma metastasis as well as the results of a systematic literature review through which we identified sixfold more cases than previously accounted for. Combining our case with those in the literature, we analyzed patient demographics, tumor characteristics, treatment modalities, and outcomes to identify factors that impact patient survival.
METHODS
Ethics statement
This report was conducted according to the guidelines of the Declaration of Helsinki for biomedical research, and was deemed exempt by the Institutional Review Board for individual patient consent (2021P000600).
Search method
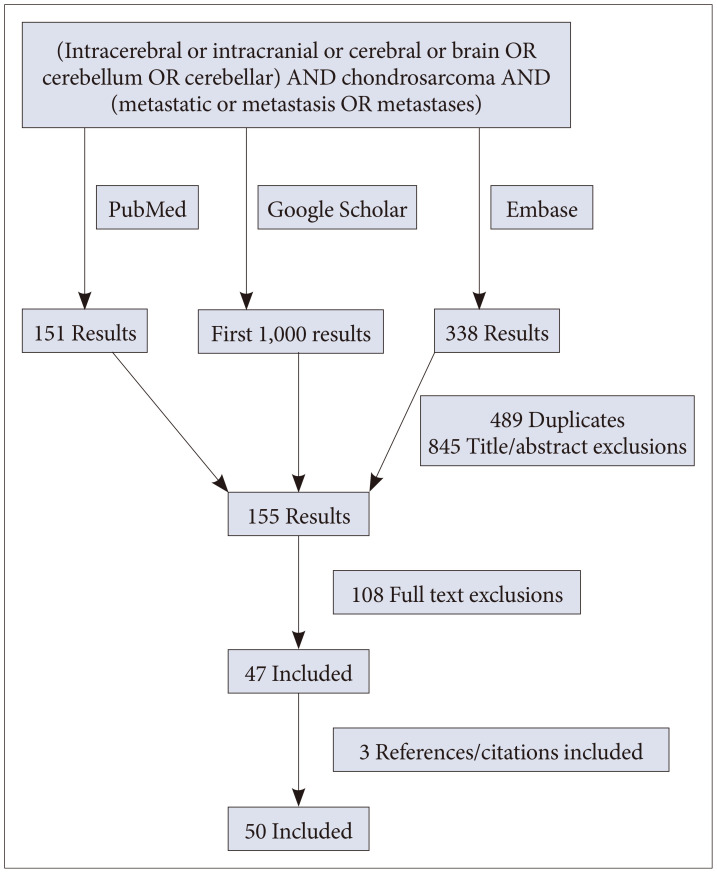
A systematic review was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines using the electronic databases of PubMed/MEDLINE, Embase, and Google Scholar for publications through April 2022 by the first author (CM). Titles and abstracts were reviewed; duplicates and results not matching search objectives were excluded. Full-text articles were reviewed for relevant references/citations. Inclusion criteria were 1) a peer-reviewed article or conference presentation 2) with at minimum an abstract in English 3) describing a remote, secondary intracranial chondrosarcoma. Extracted variables included patient demographic, tumor characteristics, and outcomes.
Statistics
SPSS Statistics Version 25 (IBM Corp., Armonk, NY, USA) was used for statistical calculations. The nonparametric Mann-Whitney U-test was used for continuous variables and chi-square or Fisher’s exact test for categorical variables. Generated Kaplan-Meier survival curves were compared using log-rank tests for univariate analysis. A stepwise multivariate Cox proportional hazards model was created for the time-dependent outcome of mortality. Median survival was listed as median± standard error. A p≤0.05 was considered to be significant.
RESULTS
Illustrative case
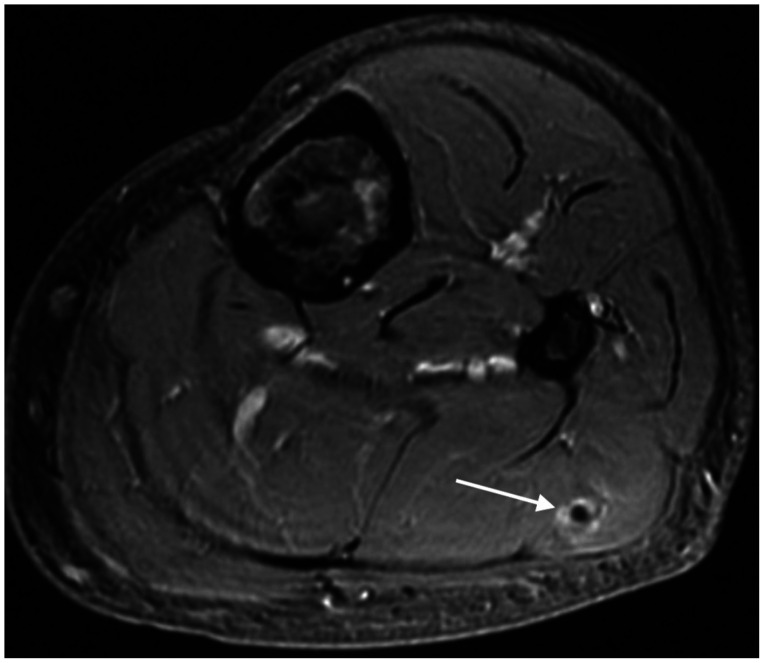
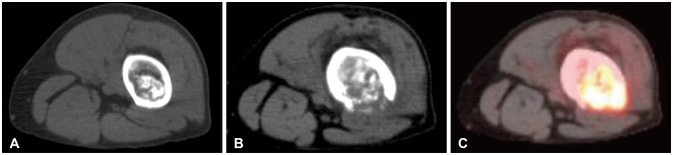
A 66-year-old male patient presented in May 2020 following 2 months of left thigh pain. His medical history was significant for multiple enchondromatosis misdiagnosed in childhood as fibrous dysplasia. A 2010 bone scan demonstrated enchondromas of the bilateral femurs, tibias, fibulas, and right hallux, and an MRI calf showed a subcutaneous calf hemangioma consistent with Maffucci syndrome (Fig. 1). Interval imaging demonstrated stable disease burden until a fluorodeoxyglucose (FDG)-positron emission tomography (PET) scan obtained in the setting of new symptoms demonstrated a 12-cm signal abnormality of the distal femur with cortical destruction and soft tissue mass (Fig. 2). The remainder of the FDG was negative for malignancy.
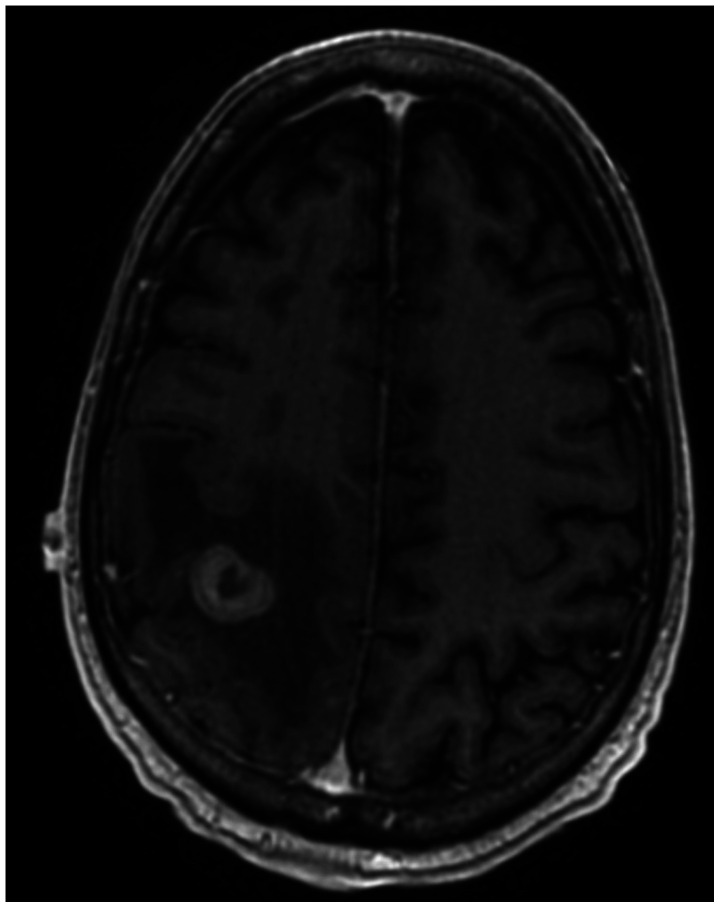
Biopsy of the lesion revealed dedifferentiated chondrosarcoma, and he underwent wide resection with reconstruction endoprosthesis in July 2020. After 4 cycles of doxorubicin-cisplatin chemotherapy, a re-staging chest CT in October 2020 demonstrated multiple pulmonary nodules. Two weeks later, he developed partial seizures involving the left arm. An MRI revealed an enhancing 2.8-cm right parietal mass with edema (Fig. 3). Gross total resection of the mass was achieved, and he underwent hypofractioned stereotactic radiation (3×8 Gy). However, he was readmitted 2 weeks post-resection in status epilepticus. Repeat MRI excluded an acute process. He was discharged on 3 anti-epileptic drugs and initiation of gemcitabine-docetaxel. Three days after discharge, he returned with somnolence, confusion, and left hemiparesis. Interval head CT showed worsening hemispheric edema without an underlying mass. Chest CT showed significant progression of his pulmonary disease. He was transitioned to comfort measures and passed away in December 2020 at age 67.
Histopathology
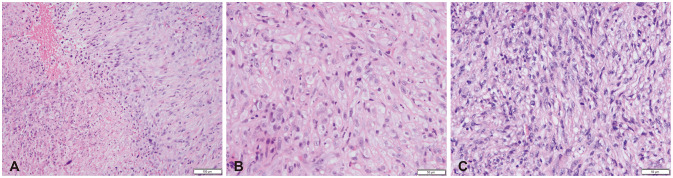
On gross examination, the femoral lesion was an ill-defined, tan-white gelatinous mass extending from the diaphysis into soft tissue. Microscopy revealed a low-grade cartilaginous tumor juxtaposed to a high-grade, spindle cell neoplasm with a mitotic rate of 24 per 10 high-power field (HPF) in tumor-rich areas (Fig. 4). Margins were negative. Immunohistochemistry included positive staining for MLH1, MSH2, MSH6 and PMS2, and negative staining of S100, MNF116, SMA, desmin, and GFAP. FoundationOne analysis showed mutations of CHEK2
S428F, IDH1 R132C, and TERT promoter-124C>T as well as amplification of CDK4 and MDM2. A diagnosis of femoral grade 3 dedifferentiated chondrosarcoma was made. The brain metastasis demonstrated focal GFAP positivity but was architecturally similar to the femoral lesion. Since GFAP is a marker of cartilaginous differentiation [17] and the sample otherwise resembled the primary lesion, a diagnosis of high-grade dedifferentiated chondrosarcoma metastatic to the brain was rendered.
Primary site
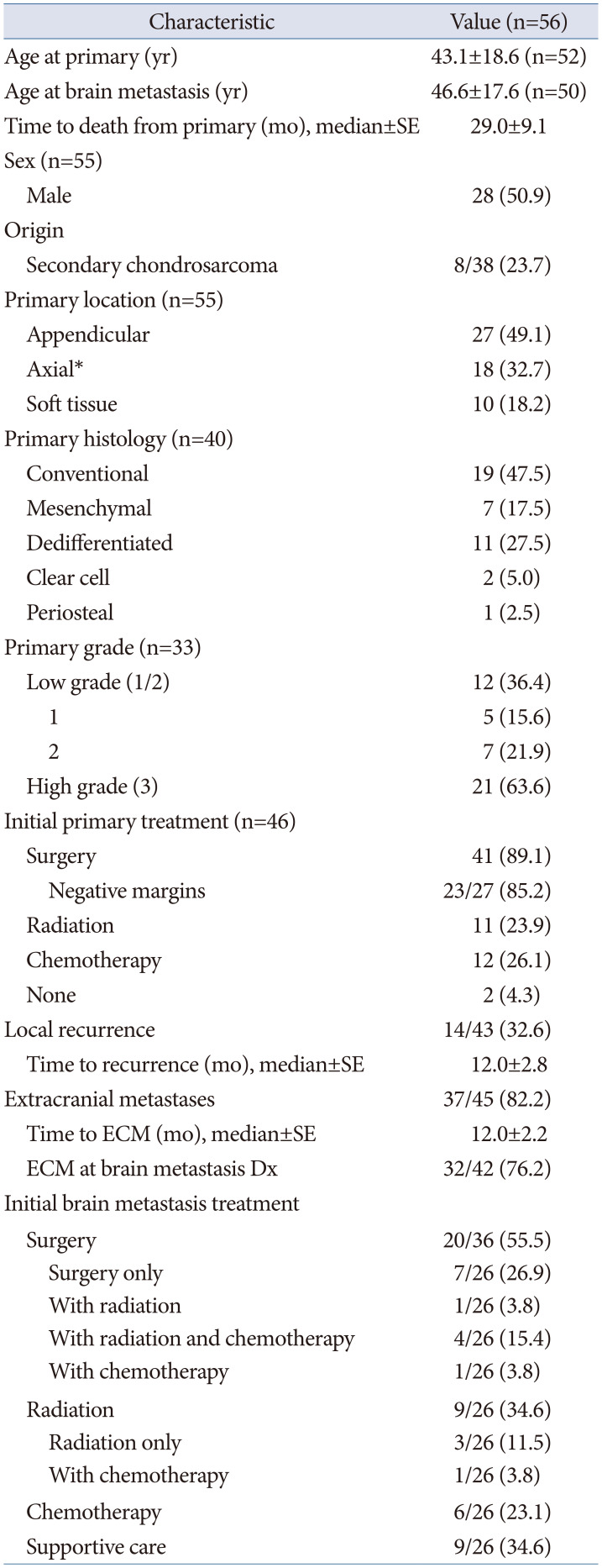
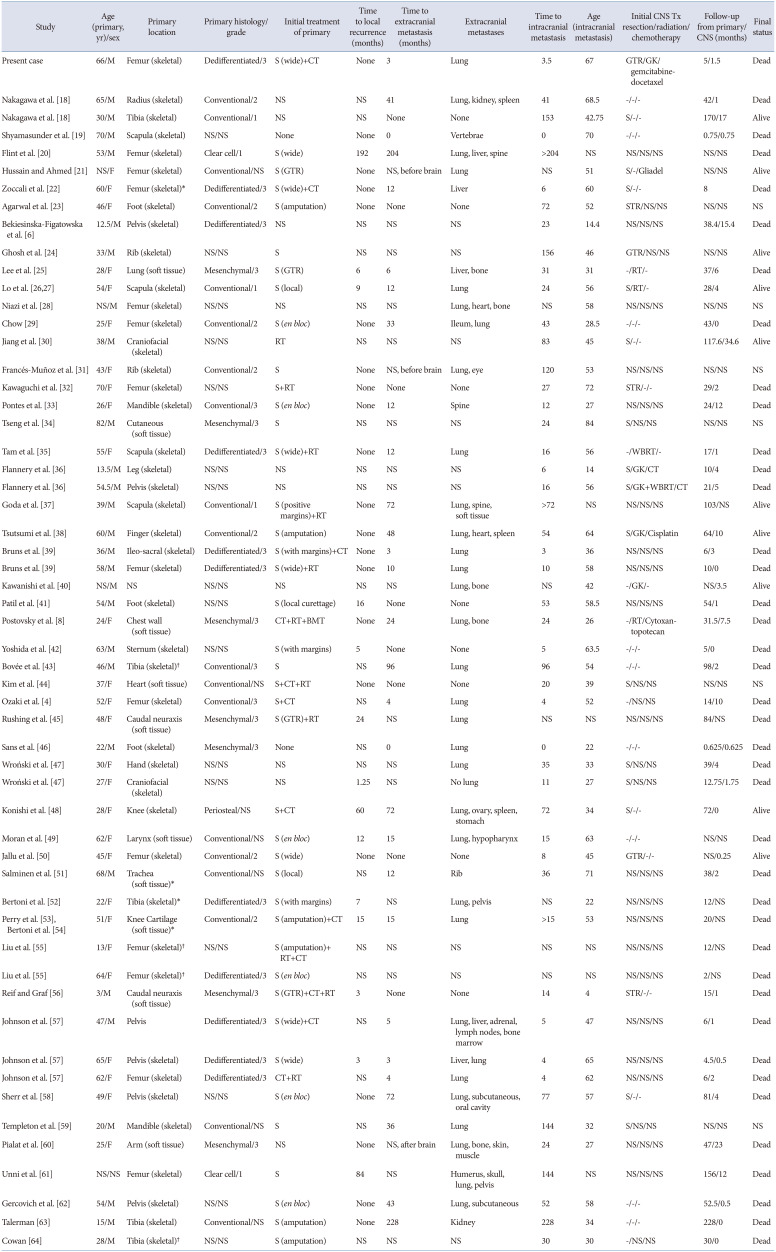
Fifty-six cases met the inclusion criteria, including the present case (Fig. 5, Tables 1 and 2) [4681819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364]. The mean age at diagnosis of the primary chondrosarcoma was 43.1±18.6 years with an even distribution between the sexes. The most common primary site, histology, and grade were the appendicular skeleton (27/55 cases, 49.1%), conventional chondrosarcoma (19/40 cases, 47.5%), and grade 3 (21/33, 63.6%), respectively. Surgery was pursued as initial primary site treatment in 89.1% of cases (41/46) with 23/27 cases documenting clean resection margins. Radiation and chemotherapy were utilized in a quarter of cases. A third of cases had local recurrence (14/43) at a median of 12±2.8 months from initial diagnosis, and 82.2% of cases developed extracranial metastases at a median interval of 12±2.2 months from the time of initial diagnosis. The median survival from primary diagnosis was 29±9.1 months (Table 1).
Development of brain metastasis
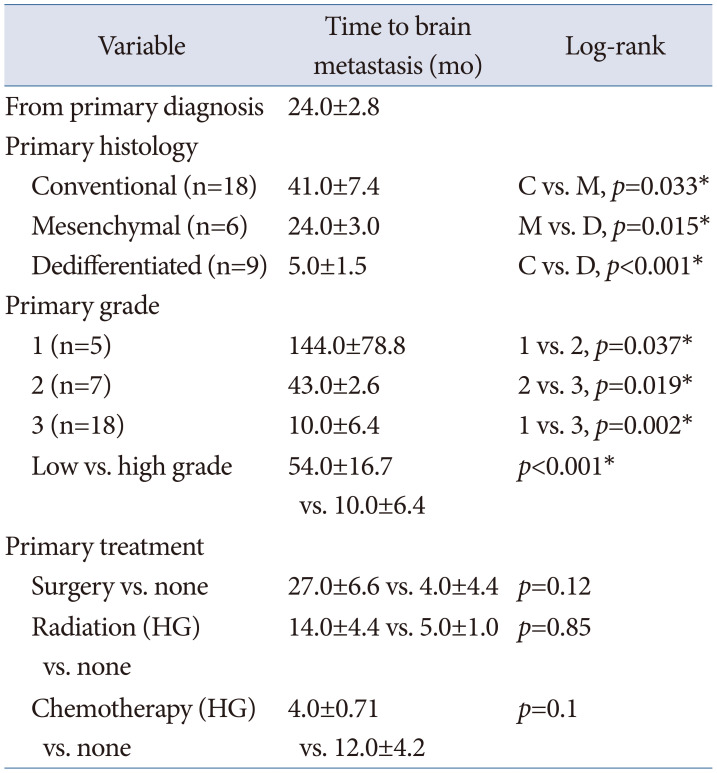
The average age at brain metastasis was 46.6±17.6 years. At the time brain metastases were diagnosed, extracranial metastases were already identified in 76.2% of cases (32/42). Brain metastasis occurred at a median of 24±2.8 months from primary diagnosis (Table 3). Primary histology and grade were correlated with the time to brain metastasis with dedifferentiated and high-grade chondrosarcomas demonstrating earlier median times to brain metastasis (dedifferentiated 5±1.5 months, mesenchymal 24±3.0 months, conventional 41±7.4 months, p<0.05; low grade 54±16.7 months vs. high-grade 10±6.4 months, p<0.001) (Table 3).
Survival from brain metastasis
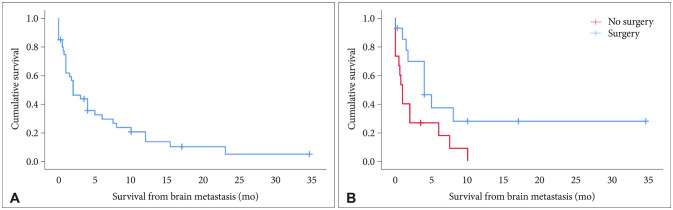
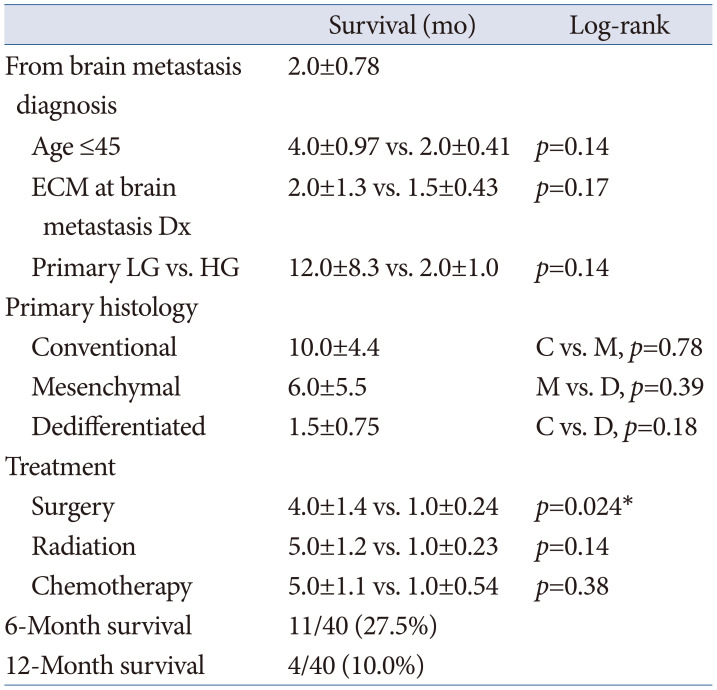
Median survival after the development of brain metastasis was 2.0±0.78 months with a 1-year survival of 10.0% (4/40) (Table 4). Surgery for a single or symptomatic metastases was performed in 55.5% of cases (20/36). Radiation therapy was used in 34.6% of cases (9/26). One third of patients received supportive care only (9/26). Surgery was associated improved median survival (4.0±1.4 months vs. 1.0±0.24, p=0.024) (Fig. 6). On multivariate Cox regression analysis controlling for sex, age, extracranial tumor burden at the time of intracranial metastasis, and treatment modality, surgery demonstrated reduced brain metastasis mortality risk (hazard ratio [HR] 0.22, 95% confidence interval [CI] 0.064–0.763, p=0.017) and radiation trended towards reduced mortality risk (HR 0.31, 95% CI 0.091–1.072, p=0.064).
DISCUSSION
Here, we present the largest systematic review of intracranial metastatic chondrosarcoma to date. Our analysis indicates that most chondrosarcomas metastatic to the brain occur in the fifth decade of life (46.6±17.6 years), evenly distributed between the sexes, have pre-existing extracranial metastases at presentation (76.2%), and arise at a median of 24±2.8 months after primary chondrosarcoma diagnosis. The development of chondrosarcoma brain metastases is a particularly grim event. Although chondrosarcoma metastases in general yield a median survival of 14.0±2.5 months and a 5-year overall survival of 28.4% [5], our data suggest that when chondrosarcoma metastasizes to the brain that the median survival is only 2.0±0.78 months with a 1-year survival of 10.0%.
The overall 5-year survival for chondrosarcomas across grade and location is 75.2% [65]. Tumor- and patient-specific factors impacting survival include patient age [66], tumor histology [267] and grade [26667], molecular profile [68], primary location [16669], primary site surgery [153766], and primary site radiation [169]. Although local recurrence shortens survival, metastatic spread particularly impacts mortality [16667]. In a long-term study of primary central chondrosarcomas, Andreou et al. [69] noted a 5-year overall survival among nonmetastatic tumors of 89% compared to 23% for those with metastases. Wang et al. [5] reported high grade chondrosarcomas with metastases at presentation (grade 3) had worse median survival than low grade (grade 1 or 2) chondrosarcomas presenting with metastases (9.0±1.7 vs. 49±15.7 months). Amer et al. [67] observed that 19.8% of dedifferentiated and 10.6% of mesenchymal chondrosarcomas present with metastases.
We observed significantly shorter intervals to brain metastasis among higher grade primary tumors than lower grade tumors (10±6.4 vs. 54±16.7 months). Dedifferentiated tumors (5.0±1.5 months) have the shortest interval from primary to metastatic diagnosis followed by mesenchymal (24±3.0 months) and conventional chondrosarcomas (41±7.0 months). Accounting for brain metastasis, primary tumor histology or grade did not impact survival, which likely reflected interval progression of primary low-grade tumors to higher grade tumors at metastasis as one-third of low-grade primaries (4/12) [2026273859] demonstrated progression on tissue obtained after recurrence. While primary site surgery exhibited a trend towards longer interval in the development of brain metastases (27±6.6 vs. 4.0±4.4 months, p=0.12), the rarity of nonsurgical primary site management (n=5) restricted this analysis. In light of the dismal prognosis of metastatic chondrosarcoma, high clinical suspicion for malignant progression of low-grade primaries and systemic surveillance of high-grade primaries is warranted.
Among 38 cases for which there was sufficient clinical history, an underlying benign cartilaginous lesion transformed to a chondrosarcoma in 23.7%. In 5 of 8 cases, the cartilaginous lesion was part of a multiple enchondromatoses syndrome. Four cases had a diagnosis of Ollier disease; ours represented the first probable case of Maffucci syndrome. Ollier disease has a prevalence of 1 per 100,000 people and is differentiated from the rarer Maffucci syndrome by the presence of concurrent hemangiomas in the latter [70]. While malignant conversion is rare (<1%) among non-syndromic enchondromas [71], conversion to chondrosarcoma ranges from 20%–45.8% in Ollier disease and 30.5%–57.1% in Maffucci syndrome [72]. In our review, the time from syndromic diagnosis to diagnosis of chondrosarcoma ranged from 10–63 years with brain metastasis occurring 2 months to 8 years after malignant conversion [435564]. Although the sarcomatous transformation may take years to occur, once it happens the resulting lesion is as metastatically aggressive as primary chondrosarcomas. With fewer than 200 cases of Maffucci syndrome in the literature [70], our patient is the first to have intracranial chondrosarcoma metastasis described.
Chondrosarcomas subdivide into five categories: 1) grade 1–3 primary or secondary, central or peripheral conventional; 2) grade 3 dedifferentiated; 3) grade 1 clear cell; 4) grade 3 skeletal or extra-skeletal mesenchymal; and 5) periosteal [73]. The presence of cartilaginous matrix on histopathology is a critical diagnostic marker [1]. We excluded 6 cases of “extraskeletal myxoid chondrosarcomas” from analysis [747576777879] because they lack cartilaginous differentiation and are not considered to be true “chondrosarcomas” [80]. Although chondrosarcomas do not have a specific molecular marker, somatic mutations of IDH1/IDH2 help differentiate chondromas/chondrosarcomas from other mesenchymal bone tumors. Since mesenchymal IDH1/IDH2 mutations promote chondrogenic differentiation over osteogenic differentiation, it is unsurprising that nearly 80% of chondrosarcomas arising in multiple enchondromatosis syndromes demonstrate this mutation [81]. Although the importance of IDH1/IDH2 mutations in chondrosarcoma prognosis is unsettled, some studies have evinced its negative impact on survival [68]. Because of its relative recency as a marker, an IDH1 mutation was formally reported in only 2 other cases in addition to ours [18].
A third of metastatic intracranial chondrosarcoma patients were managed with supportive care only, which reflects the aggressiveness of the disease and its systemic burden with 82% of cases with intracranial metastases ultimately developing extracranial metastases. Both surgery and radiation of intracranial metastases improved median survival by 3–4 months, which suggests that patients with single or symptomatic brain metastases and reasonable systemic burden may benefit from intracranial treatment. Multivariate analysis further suggested reduced mortality risk following surgery (HR 0.22, p=0.017). Radiation therapy had a nonsignificant association with improved mortality (HR 0.31, p=0.064). Chemotherapy for intracranial disease burden was not associated with survival benefit. Although ours is the first study to specifically examine management of chondrosarcoma brain metastases, it has been previously shown that metastasectomy generally confers survival benefit in metastatic chondrosarcoma [6982]. The modest benefit of surgery or radiation in appropriately selected patients with chondrosarcoma brain metastases reflect treatment outcomes of sarcomatous brain metastases more generally [712].
Limitations
This systematic review has several limitations. First, it combines case reviews and series; therefore, it is highly susceptible to publication and retrospective-study biases. Second, techniques of radiation, surgery, and chemotherapy continue to improve, confounding treatment comparisons. Third, study heterogeneity complicates analysis, including differences in treatment approaches, patient characteristics, and histologic reports. Finally, outcome data remains significantly limited by small sample size and lack of long-term follow-up.
Conclusion
Metastatic cerebral chondrosarcomas are rare but aggressive neoplasms. On average, they arise 24±2.8 months after primary chondrosarcoma diagnosis. Following their development, median survival is 2.0±0.78 months with a 1-year survival of 10%. Primary lesion histology and grade influence the interval between initial diagnosis and the identification of a brain metastasis. Where feasible, surgical resection improves survival. Multiple enchondromatoses syndrome underlie 13.2% (5/38) of cases of chondrosarcomatous brain metastases and warrant high clinical suspicion.
 XML Download
XML Download