

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic, which began at the end of 2019, has become an unprecedented, prolonged global event. The healthcare system faced numerous crises that posed a threat of overwhelming the existing medical systems. This resulted in a sudden surge in demand for COVID-19 treatments, shortage of medical resources, and a temporary disruption in providing care to patients with other ailments. Brain tumor patients were not immune to these challenges, and healthcare professionals found it challenging to provide adequate management given the limited resources available. However, providing effective management for patients during a crisis can be challenging in the absence of proper guidelines.
Several leading international medical associations in the field of neuro-oncology have proposed guidelines for the management of brain tumor patients during the COVID-19 pandemic [123]. The American Association of Neurological Surgeons (AANS)/Congress of Neurological Surgeons (CNS) Tumor Section and the Society for Neuro-Oncology (SNO) released general treatment guidelines for prioritizing inpatient and outpatient cases during the pandemic in 2020 [2]. Likewise, the neuro-oncology community in the UK also presented guidelines for the management of neuro-oncology patients during this period [3]. However, these guidelines have limitations in their applicability in Korea due to the uniqueness of the domestic medical environment.
In response to this, the Korean Society for Neuro-Oncology (KSNO), a multidisciplinary academic society, developed specialized clinical guidelines for the management of brain tumor patients in the domestic medical environment during a crisis. The aim of this project was to develop comprehensive guidelines that can be applied universally to various situations that may cause a scarcity of medical resources, not limited to the COVID-19 pandemic. In this guideline, a crisis period is defined as a situation in which medical resources for managing brain tumor patients are limited due to various causes such as natural disasters, mass infection crisis, and wars, making it impossible to proceed with usual management. The guideline addresses the selection of treatment priorities, including surgery, radiotherapy, chemotherapy, clinical trials, radiographic surveillance, and telemedicine, for managing brain tumor patients during the crisis period.
METHODS
This guideline concerns the management of brain tumor patients during crisis situations where there is insufficient evidence available. To address these issues, the Delphi technique was employed. This method involves gathering and synthesizing the expert opinions through multiple rounds of surveys and summarizing them as a collective decision. The Delphi process is a proven and validated method for achieving consensus within medical groups [45]. The Delphi process employed in this guideline is detailed in Fig. 1.

The expert group comprised 22 multidisciplinary members of the KSNO Guideline Working Group, consisting of 16 neurosurgeons, 4 radiation oncologists, 1 medical oncologist, and 1 pathologist. They undertook a review of various guidelines related to the management of brain tumor patients during crisis situations, primarily the COVID-19 pandemic, and identified the issues to be addressed in this guideline. Subsequently, a questionnaire was formulated for each round of surveys, and experts were requested to provide comments for each question explaining their responses. Three rounds of surveys were conducted between June and August 2022, and the questionnaire was modified and expanded based on the results of each preceding round.
A final survey was conducted in October 2022 consisting of seven categories: treatment priority, pathology, surgery, radiotherapy, chemotherapy and clinical trial, radiological surveillance, and telemedicine. The survey included 39 questions (Supplementary Material in the online-only Data Supplement). Feedback from the previous rounds was provided to the experts during the final survey, allowing them to consider the views of their peers and revise their original responses. To ensure that no one expert’s opinion dominated the consensus, responses were submitted anonymously. The entire survey process was conducted remotely using Google Forms (https://forms.google.com/). The results of the final survey were used to draft the current consensus recommendations. Consensus was defined as an agreement level of 50% or higher among the panel of experts [5]. A consensus statement was considered “recommended” for clinical practice when agreement reached 50%–74%, and “highly recommended” when agreement reached 75% or higher. No confidential or patient information was used in the survey, and ethics committee approval was not deemed necessary, as is typical in Delphi method studies conducted in the medical field [6].
RESULTS
All participating experts completed the final survey process. The results of the survey for each question are presented in the Supplementary Material (in the online-only Data Supplement).
General treatment priority
When determining treatment priority for brain tumor patients during crisis periods, it is crucial to consider various factors such as the presence or absence of acute neurological deterioration with symptoms of increased intracranial pressure (IICP), the progression rate of the tumor, the possibility of neurological improvement following treatment, the long-term prognosis after treatment, the patient’s age, and underlying medical conditions. Expert panels suggest that the presence or absence of acute neurological deterioration with IICP symptoms is the most significant factor in determining treatment priority, with 85.7% of the panel in agreement. Furthermore, 71.4% of expert panels agreed that, in cases where other factors are similar, a newly diagnosed case should receive higher priority during a crisis period than a recurrent case. All expert panels agreed that treatment priority for cases with a very poor prognosis, even with prompt treatment, can be postponed to allocate medical resources effectively during the crisis period. However, it is essential to consult adequately with the patient and their caregiver before making any decisions.
Surgery
During the crisis period for brain tumor patients, a vast majority of expert panels (95.2%) have agreed on the surgical priority level based on the “time window-based criteria.” It has also been widely agreed (95.2%) that reassessment of surgical priority should be done regularly, considering factors such as the severity of neurological symptoms, availability of medical resources, and the possibility of adjuvant treatment after surgery. The recommended levels of surgical priority are detailed in Table 1. However, consensus has not been reached among expert panels regarding whether benign tumors, with a relatively better long-term prognosis than malignant tumors, should be given surgical priority during the crisis period. While some experts (52.4%) have agreed that the extent of tumor resection for malignant tumors can be reduced to effectively allocate limited medical resources, there are substantial opposing opinions (42.9%). Finally, a significant majority of expert panels (90.5%) have agreed that surgical intervention for brain tumor patients with a legally communicable disease, such as COVID-19, should only be carried out on patients classified as surgical priority A. Surgery for patients with lower surgical priority should be postponed until the quarantine period has ended.

Table 1
Proposed surgical priority during the crisis period
![]()
Pathology
In terms of pathology examination, a particular matter was scrutinized. A significant majority of experts (95.2%) agreed that a treatment plan could be developed based on conventional histological diagnoses alone, without molecular genetic information, especially during the crisis period for diagnosing World Health Organization (WHO) 2021 diffuse glioma.
Radiotherapy
Radiotherapy is an essential treatment modality in neurooncology. Therefore, during times of crisis such as outbreaks of infectious diseases (e.g., COVID-19) or natural disasters which can cause shortage of medical resources, ensuring efficient distribution of radiotherapy resources including medical staff, space, equipment availability, is crucial. Furthermore, for high-risk patients vulnerable to infectious diseases, reducing the visit to radiotherapy facilities is essential. In this study, we conducted a survey to reach a consensus among Korean neuro-oncologists on the issues described below.
Prioritizing radiotherapy during the crisis
In order to provide guidance to physicians during periods of crisis, where there may be a shortage of medical resources, expert panels have established a consensus on how to prioritize patients in need of radiotherapy. Specifically, the panels were asked to consider whether a simple “time window-based criteria” or a “disease-specific clinical scenario-based criteria” would be more appropriate for prioritization purposes. Out of the 21 respondents, 85.7% recommended that patients be prioritized based on treatment time window and prognosis, as detailed in Table 2.

Table 2
Proposed radiotherapy priority during the crisis period
![]()
Radiotherapy dose-fractionation for patients with high-grade gliomas during the crisis
An expert panel was consulted to determine whether hypofractionated radiotherapy could be routinely prioritized over conventionally fractionated radiotherapy in 6 weeks for elderly patients with high-grade gliomas. All 21 respondents (100.0%) agreed that hypofractionated radiotherapy should be preferred for elderly patients during the crisis period. Additionally, respondents commented that hypofractionated radiotherapy should also be preferred for high-grade glioma patients with poor performance or frailty during the crisis.
We also conducted a survey to determine the most preferred hypofractionated radiotherapy regimen for high-grade glioma patients during the crisis. Among the 21 respondents, the most preferred regimen for hypofractionated radiotherapy when medical resources are scarce was “40–45 Gy in 3 weeks” (57.1%). Six respondents (28.6%) suggested that the hypofractionated dose-fractionation schedule should be determined based on the severity of medical resource shortage. This was followed by 34 Gy in 2 weeks (9.5%) and 25–30 Gy in 1 week (4.8%).
Utilization of radiotherapy resource during the crisis
In the survey, expert panels were presented with three options for choosing between hypofractionated and conventionally fractionated radiotherapy for brain tumor patients. These options were: 1) hypofractionated radiotherapy for all brain tumor cases; 2) hypofractionated radiotherapy only for cases where adequate treatment efficacy is expected, or sufficient evidence is published; and 3) conventionally fractionated standard radiotherapy in all cases. Most respondents (76.2%) agreed that hypofractionated short-course radiotherapy can be preferred over conventionally fractionated standard radiotherapy, but only when adequate treatment efficacy is expected or sufficient evidence is published, even in a resource-constrained crisis setting. None of the respondents agreed that conventionally fractionated standard radiotherapy is the preferred dose-fractionation for all cases.
Regarding brain tumor patients who require radiotherapy and have a legally communicable disease such as COVID-19, 81% of expert panels responded that only patients with “priority level A” (Table 2) should be considered for radiotherapy as required. Only 9.5% of respondents agreed to treat patients with “priority level B” (Table 2) as well. Apart from patients with “priority level A,” some experts recommended considering radiotherapy in cases such as germinoma or lymphoma where a high response rate can be expected with radiotherapy, and chemotherapy is not feasible due to the shortage of healthcare resources.
Chemotherapy
According to a survey of experts, 85.7% believe that chemotherapy should be administered when it can significantly improve the patient’s prognosis or alleviate tumor-related symptoms. The priority of chemotherapy goals should be curative first, followed by neoadjuvant/adjuvant, and then palliative, according to the majority of respondents. Specifically, 85.7% of the respondents consider neoadjuvant/adjuvant chemotherapy to be a higher priority than palliative chemotherapy. During the crisis period, most experts (85.7%) prefer a chemotherapy regimen that is relatively effective, has low toxicity, and minimizes visits to medical institutions. For non-emergency patients who are unable to receive chemotherapy immediately due to lack of resources, the majority (85.7%) believe that chemotherapy should be postponed for a certain period, with transfer to a medical institution if the problem persists. Finally, the survey found that decisions regarding the chemotherapy regimen for a patient during the crisis period should be made through a multidisciplinary approach or care, according to 52.4% of the respondents.
Clinical trial
The majority of experts (76.2%) advocated for the continuation of ongoing subjects while suspending new subject registration and new clinical trials. A minority of the experts (14.3%) proposed that clinical trials should proceed without restrictions. Only a small percentage (4.8%) suggested that all clinical trials should be suspended during the period of crisis.
Radiological surveillance
In situations where medical resources are limited, such as during the COVID-19 pandemic, it is crucial to establish a routine surveillance interval. Efficient allocation of resources may be more important than prioritizing treatments as mentioned previously. A survey was conducted for each content, and a sufficient consensus was reached.
The modified radiological surveillance schedule during the crisis
The adequate radiological surveillance schedule for patients with a primary malignant brain tumor (e.g., malignant glioma) or brain metastasis after standard treatment during the crisis period was asked according to their disease status such as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD).
For primary malignant brain tumors, the majority of respondents (66.7%, 71.4%, and 71.4% for CR, PR, and SD, respectively) recommended extending the follow-up period beyond the existing protocol. Similarly, for cases of brain metastasis, most respondents suggested a longer follow-up period than the current protocol for all response categories (66.7%, 81.0%, and 76.2% for CR, PR, and SD, respectively). Moreover, nearly all respondents (95.2%) concurred with the decision to defer follow-up MRIs for benign brain tumors that do not exhibit any clinical signs of progression.
However, other panel opinions recommended that follow-up MRI should be conducted routinely in certain cases, even in the absence of clinical progression. These include 1) types of tumors known to have high risk of malignant transformation, 2) lesions located near the brainstem or cranial nerve where there is a serious risk of irreversible growth, and 3) tumors with an expected high growth rate.
The feasibility of using an alternative to MRI
When asked whether CT (with or without contrast) can be used as a substitute for MRI, assuming limited resources for MRI, 76.2% of respondents said it is possible to replace it in the case of an extra-axial tumor, while 57.2% said it can be used as a substitute for an intra-axial tumor.
Telemedicine
Due to the COVID-19 outbreak, non-face-to-face treatment have become inevitable, resulting in an increased interest in telemedicine. Telemedicine can be a crucial tool during crises like the COVID-19 pandemic. In this regard, a survey was conducted.
Necessity of telemedicine
All respondents (100%) agreed that telemedicine can be actively considered when treating brain tumor patients in an infectious disease crisis such as the COVID-19 pandemic. Regarding the question of whether telemedicine can serve as a substitute for all clinical situations, most respondents answered affirmatively for patients who have completed standard treatment for malignant brain tumors, as well as patients who have undergone treatment for brain metastasis (such as surgery, stereotactic radiosurgery [SRS], whole brain radiation therapy [WBRT], chemotherapy, or combined treatment). However, respondents noted that telemedicine may not be suitable for cases where the disease status is PD.
Regarding the benign brain tumors, most respondents (90.5%) answered that telemedicine can be used, regardless of whether there is a residual tumor. Additionally, most respondents agreed that telemedicine can be substituted for patient interviews or progress checks during chemotherapy (90.5%) or radiotherapy (95.2%). However, when asked whether telemedicine can be used to treat new patients who need surgery, radiotherapy, or chemotherapy, a significant number of respondents answered that it is not substitutable (71.4%, 66.7%, and 61.9%, respectively).
Platform for telemedicine
In general, telemedicine can be done using video and audio communication equipment between the doctor and the patient. However, many respondents (66.7%) stated that further advanced platforms are needed to ensure safe and efficient telemedicine as a substitute for in-person treatment. There were additional opinions that a remote digital measuring instrument for vital signs and a nervous system function evaluation system could prove beneficial.
DISCUSSION
This study aims to gather insights and experiences from expert panels through the Delphi process to develop a suitable response plan in the event of a potential crisis that might cause a scarcity of healthcare resources in the future. The final consensus recommendations for the management of brain tumor patients during a crisis period have been summarized in Table 3 based on the result of the Delphi process. The KSNO Guideline Working Group acknowledges the need for a personalized management plan for each brain tumor patient, best discussed and implemented within a hospital-based multidisciplinary team. The consensus recommendations outlined in this guideline can serve as a reference for these discussions.
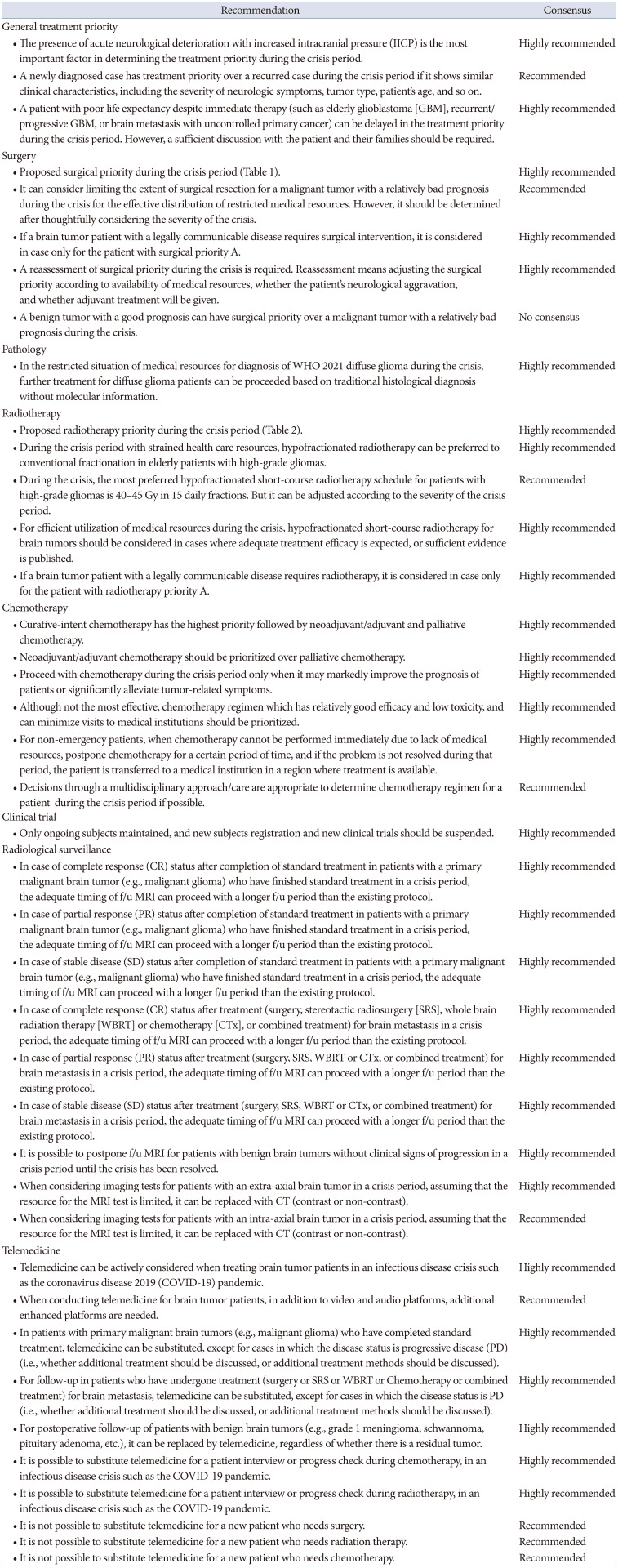
Table 3
Recommendations of the Korean Society for Neuro-Oncology (KSNO) for managing brain tumor patients during the crisis period
![]()
The surgical prioritization level described in this guideline was developed by adopting “time window-based criteria” from other guidelines during the COVID-19 pandemic with modifications to suit the domestic medical situation [78]. While other guidelines have presented a more specific surgical prioritization based on clinical scenarios [9], this approach may limit flexibility and adaptability during future crisis periods. It is also necessary to apply the surgical priority reevaluation system mentioned in this guideline to each medical facility’s circumstances. The neurosurgical treatment algorithm and checklist system developed by the University of California, San Francisco (UCSF) group during the COVID-19 pandemic may be useful in reevaluating surgical priority during crisis periods [7].
Previous radiotherapy guidelines for crisis periods such as COVID-19 have suggested prioritizing patients for radiotherapy based on their diagnosis [1011]. However, in this consensus guideline, Korean neuro-oncologists have prioritized patients for radiotherapy based on the timing of radiotherapy and the potential benefit in terms of oncological and neurological outcomes. Evidence from prospective randomized studies have demonstrated comparable outcomes with radiotherapy of 60 Gy in 6 weeks, 40 Gy in 3 weeks, 34 Gy in 2 weeks, and 25 Gy in 1 week in elderly patients with glioblastoma when treated with radiotherapy alone [1213141516]. In this context, hypofractionated radiotherapy is the preferred regimen for elderly patients with high-grade gliomas when medical resources are limited during a crisis. Among the hypofractionated dose-fractionation schedules, many Korean neuro-oncologists (57.1%) feel comfortable using the 3-week 40–45 Gy regimen for high-grade gliomas. Tabrizi et al. [17] reported that individual elderly glioblastoma patients’ risk of COVID-19 infection and mortality was mathematically calculated using hypothetical scenarios (low-, medium-, and high-risk scenarios) based on published prospective trials [1416]. The calculated risks were then compared with the risk of death due to glioblastoma. The study found that reducing visits to the radiotherapy facility with hypofractionation resulted in non-inferior outcomes compared to 6-week radiotherapy.
Consensus recommendations on chemotherapy during crisis periods emphasize the need to balance effective treatment with resource limitations. This viewpoint is in line with several guidelines [101819]. The panel agreed that priority should be given to treatments with a higher chance of cure and long-term survival, such as curative-intent and neoadjuvant/adjuvant chemotherapies. In contrast, palliative chemotherapy that does not significantly relieve tumor-related symptoms should be postponed. It is worth noting that multimodal treatment plans, including surgery, radiotherapy, and chemotherapy, are often necessary to achieve long-term survival and cure. For example, in patients with glioblastoma, omission of radiotherapy and/or temozolomide leads to a worse prognosis compared to the standard protocol [202122]. If it is not feasible to provide post-surgery treatment during a crisis period, curative-intent surgery may not be justified. Thus, the panel emphasizes the importance of providing the best possible care through a multidisciplinary approach.
The panel has reached a consensus regarding the prioritization of chemotherapy regimens that effectively balance efficacy and low toxicity, thereby reducing the number of hospital visits for patients. In addition, to ensure patient safety, the consensus recommends the suspension of new clinical trial registrations and only the continuation of ongoing trials. In the case of oligodendroglioma with 1p19q codeletion, the current standard treatment after surgical resection is radiotherapy along with neoadjuvant or adjuvant PCV (procarbazine, lomustine, and vincristine) [2324]. The adjuvant PCV regimen has been shown to improve overall survival and progression-free survival in patients with 1p19q codeleted oligodendroglioma compared to radiotherapy alone [25]. However, the PCV regimen is associated with a higher toxicity profile and requires more frequent hospital visits for intravenous vincristine and multiple-dose oral medication schedule [2324]. On the other hand, radiotherapy with concurrent and adjuvant temozolomide has a relatively lower toxicity profile and a simpler dosing schedule without intravenous drug administration [26]. The initial results of the ongoing CODEL phase III randomized trial indicate a 5-year overall survival rate of 91% in patients receiving concurrent and adjuvant temozolomide in combination with radiotherapy in 1p19q codeleted oligodendroglioma [27]. Despite the preliminary and inconclusive nature of these results, the consensus recommendation determined by the panel and previous study results do not necessarily suggest a clear advantage for PCV-based adjuvant therapy over alternative postoperative treatment strategies for grade 2 or 3 gliomas during the crisis period [28].
With the COVID-19 outbreak, non-face-to-face medical care has gained significant momentum, and there has been a surge of interest in telemedicine. While many patients have hailed its convenience, some medical professionals have been cautious of its potential risks. As a result, several IT companies are now expediting the development of platforms related to telemedicine. Moreover, many countries are also making changes to their legal systems to accommodate this new paradigm. Recently, several preliminary studies on feasibility of telemedicine have been reported according to this atmosphere [293031]. The present guideline also tried to explore the potential role and direction that telemedicine may have in the field of neurooncology in the future.
In the event of future crises that result in a shortage of medical resources, such as the COVID-19 pandemic, it is expected that these consensus recommendations will serve as a reference for prioritizing the management of brain tumor patients. They will also provide guidance for making decisions in various scenarios that may arise during the management of brain tumor patients. Additionally, it is worth noting that the development of these guidelines differs from the conventional method of developing clinical guidelines, which typically rely on evidence from a review of existing literature. This guideline was developed through the Delphi process, which involves synthesizing and consolidating the opinions of experts by inducing their views and reaching a consensus judgment, to solve specific problems. The experience of the KSNO Guideline Working Group in this process is expected to serve as a valuable foundation for future guideline development when similar needs arise.
 XML Download
XML Download