

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since coronavirus disease 2019 (COVID-19) emerged as a global health crisis in early 2020, the COVID-19 pandemic has posed a devastating threat to the health and lives of vulnerable individuals. Stringent measures, including mandatory face mask-wearing and social distancing were implemented to prevent the spread of COVID-19.1 In addition, after new COVID-19 vaccines were approved for use, public health authorities strongly encouraged vaccination, emphasizing the preventive effect of the COVID-19 vaccine.2 However, some individuals felt that these measures violated their freedom, and even raised concerns about the efficacy and safety of the vaccines.3
COVID-19 vaccination has been controversial. The new COVID-19 vaccines were developed and authorized in an unprecedentedly short time because of the serious and urgent nature of the pandemic.4 Early evidence showed that the COVID-19 vaccines were effective at preventing COVID-19 infection and were relatively safe in terms of side effects.5 However, many individuals were still concerned about rare but serious side effects, such as blood clotting and myocarditis.6 Some even distrusted the new mRNA vaccine technology, pharmaceutical companies, and public health authorities.7 These negative attitudes toward COVID-19 vaccines may contribute to vaccine hesitancy, which has been a major obstacle to public health policies aimed at curbing the spread of COVID-19.8
Vaccine acceptance refers to the degree to which an individual accepts, hesitates to accept, or refuses vaccination.9 This may be influenced by an individual’s experience, personal values, and psychological characteristics as well as environmental factors.10 Therefore, individual behavioral and psychological characteristics influencing the decision to get vaccinated must be explored. Recent studies have found a variety of factors associated with COVID-19 vaccine acceptance or hesitancy, including demographic characteristics, economic status, vaccine information, personal values, and personality.11121314 However, most studies have evaluated COVID-19 vaccine acceptance and hesitancy based on only a few simple questions about vaccination intent.1516 No validated survey tool is available to assess vaccination behavior. Considering that vaccine acceptance is an outcome resulting from a complex decision-making process, we needed to find a new way to investigate the various attitudes and behaviors toward COVID-19 vaccination more comprehensively.
Since the COVID-19 pandemic began, we have been studying the impact of the pandemic on the daily life, behavior, and mental health of the general population and patients with mental illness in Korea. As part of this series, the present study aimed to characterize COVID-19 vaccination behavior in the Korean general population and to explore the psychological factors involved in individual decision-making on vaccination. Thus, we investigated attitudes toward COVID-19 vaccination in the Korean general population and performed clustering analysis to identify individuals’ vaccine acceptance based on various aspects of willingness and reluctance to be vaccinated for COVID-19. Then, we examined the behavioral and psychological characteristics associated with vaccine acceptance.
METHODS
Participants
The present study was a part of several mental health surveys on the psychosocial effects of COVID-19 in the general population and patients with a mental disorder.1718192021222324 We conducted an online survey of the general population with participants ranging in age from 19 to 69 years in South Korea on September 14–24, 2021, when 67–73% of the entire population had received at least the first dose of a COVID-19 vaccine since the start of COVID-19 vaccination at the end of February 2021.25 Participants were selected from a panel of an online survey service provider (Macromill Embrain). Three geographic areas were surveyed: the Seoul metropolitan area (Seoul and Gyeonggi Province [around Seoul], n = 500), Daegu City and the surrounding area (n = 500), and Gwangju City and the surrounding area (n = 500). A total of 1,500 participants were recruited using a quota sampling method with identical distributions of age and sex among these regions. Only participants who provided consent for the use of personal information were included.
Measures
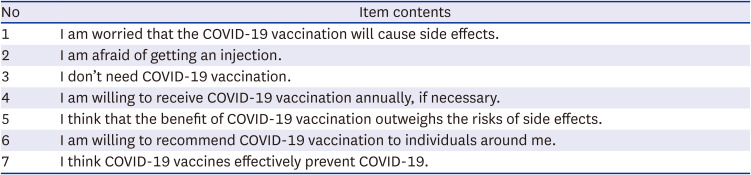
The participants indicated their acceptance and hesitancy toward COVID-19 vaccination via seven items on the COVID-19 vaccination attitude questionnaire, which we developed based on the existing literature and our experience (Table 1). The responses were rated using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). These seven items were classified into two factors in an exploratory factor analysis: ‘necessity of vaccination’ (questions 3–7) and ‘concern about vaccination’ (questions 1–2) (Supplementary Table 1). The internal consistency of this questionnaire was acceptable (Cronbach’s α = 0.81, when questions 1–3 were reverse-scored). Additionally, the participants were asked about their vaccination status for COVID-19 and influenza. The participants also responded to yes/no questions about reasons for receiving the vaccine and trustworthy sources of information regarding COVID-19 vaccination.
Table 1
COVID-19 vaccination attitude questionnaire
Depression and anxiety were measured using the Korean version of the Patient Health Questionnaire (PHQ)-9 and the Generalized Anxiety Disorder (GAD)-7 tool, respectively, which are reliable and valid tools for screening depressive and anxiety symptoms in Korean populations.2627 Gratitude was assessed using the Gratitude Questionnaire (GQ)-6, which evaluates the experience and expression of gratitude in daily life.28 We used the Korean version of GQ-6, which was validated by Kwon et al.29 Personality traits were assessed using the Big Five Inventory (BFI)-10, which is a short-form version of the BFI that measures five dimensions of personality, including extraversion, agreeableness, conscientiousness, neuroticism, and openness to experience.30 We used the Korean version of BFI-10, which was adapted by Kim et al.31 with good reliability and validity.
Statistical analysis
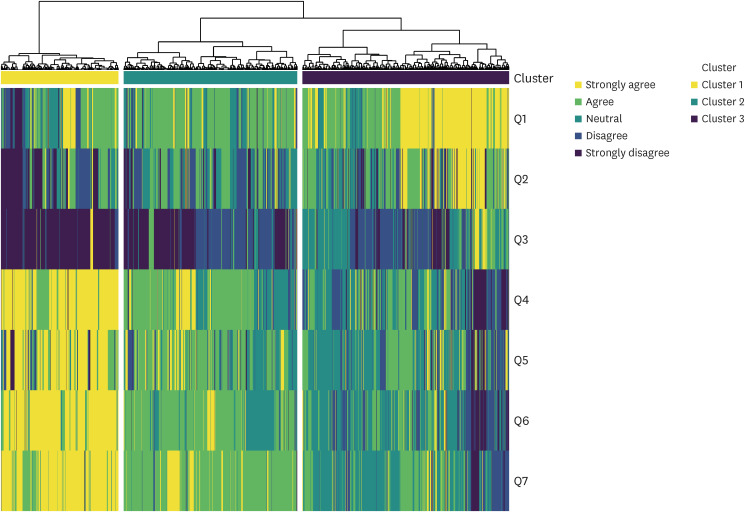
We performed a cluster analysis of the responses to the seven questions comprising the COVID-19 vaccination attitude questionnaire to identify a set of individuals with similar levels of vaccine acceptance. The 5-point Likert scale scores were subjected to hierarchical clustering using Ward’s minimum variance method and Gower’s distance as a dissimilarity matrix. The optimal number of clusters was determined using the elbow method. We visualized individuals’ response patterns to determine the properties of the clusters. This process was performed using the R packages ‘cluster’ and ‘factoextra’ (The R Foundation for Statistical Computing, Vienna, Austria). Then, we compared vaccination behaviors and psychological characteristics among the clusters using the χ2 test for categorical variables and the Quade non-parametric covariance analysis for covariate-adjusted continuous variables. All statistical tests were two-tailed, and a P < 0.05 was considered significant. Statistical analyses were performed using R (version 4.0.3; The R Foundation for Statistical Computing) and SPSS software (version 27.0; IBM Corp., Armonk, NY, USA).
RESULTS
Identification of clusters
Hierarchical clustering revealed that the study population could be grouped into clusters 1–3 (Fig. 1). In cluster 1 (n = 354, 23.6%), most respondents strongly agreed with the items related to a positive attitude toward COVID-19 vaccination (questions 4–7) and strongly disagreed with question 3 (i.e., “I don’t need the COVID-19 vaccination”). More than half of the respondents in cluster 1 strongly agreed or agreed that they were concerned about the potential side effects of the COVID-19 vaccines described in question 1. Similarly, in cluster 2 (n = 523, 34.9%), most participants agreed with questions 4–7 and disagreed or strongly disagreed with question 3. In contrast, most participants in cluster 3 (n = 623, 41.5%) were neutral toward or disagreed, or strongly disagreed, with questions 4–7, and many of them strongly agreed or agreed with question 3. In addition, about 90% of the respondents in cluster 3 expressed concerns about the side effects mentioned in question 1. Based on these patterns of responses, clusters 1–3 were labeled ‘totally accepting,’ ‘somewhat accepting,’ and ‘reluctant,’ respectively.
Demographic characteristics
Of the 1,500 participants, 50% were men, with an average age of 38.73 ± 11.95 years. In addition, 45.6% were married, 81.1% had a high school diploma or higher, 70.1% had a job, and 95.1% had health insurance.
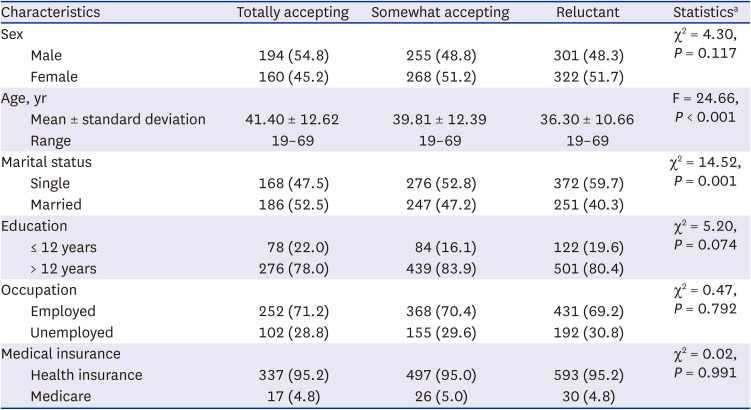
Table 2 summarizes the demographic characteristics of the three groups according to vaccine acceptance. The participants in the ‘totally accepting’ group were the oldest, followed by those in the ‘somewhat accepting’ group and the ‘reluctant’ group (F = 24.66, P < 0.001). No differences in sex, education level, occupation, or medical insurance status were observed among the three groups, except the ‘totally accepting’ group had the highest proportion of married participants (χ2 = 14.52, P = 0.001). We controlled for age as a covariate when comparing other continuous variables among the three groups.
Table 2
Demographic characteristics
Vaccination behavior
About 90% of the participants in the ‘totally accepting’ and ‘somewhat accepting’ groups had already received the first dose of the COVID-19 vaccine (Table 3). However, less than 60% of the participants in the ‘reluctant’ group had been vaccinated. The proportion of participants who seldom received the influenza vaccine was significantly higher in the ‘reluctant’ group (44.8%) than in the other two groups (34.2–35.0%).
Table 3
Behavioral characteristics associated with vaccine acceptance
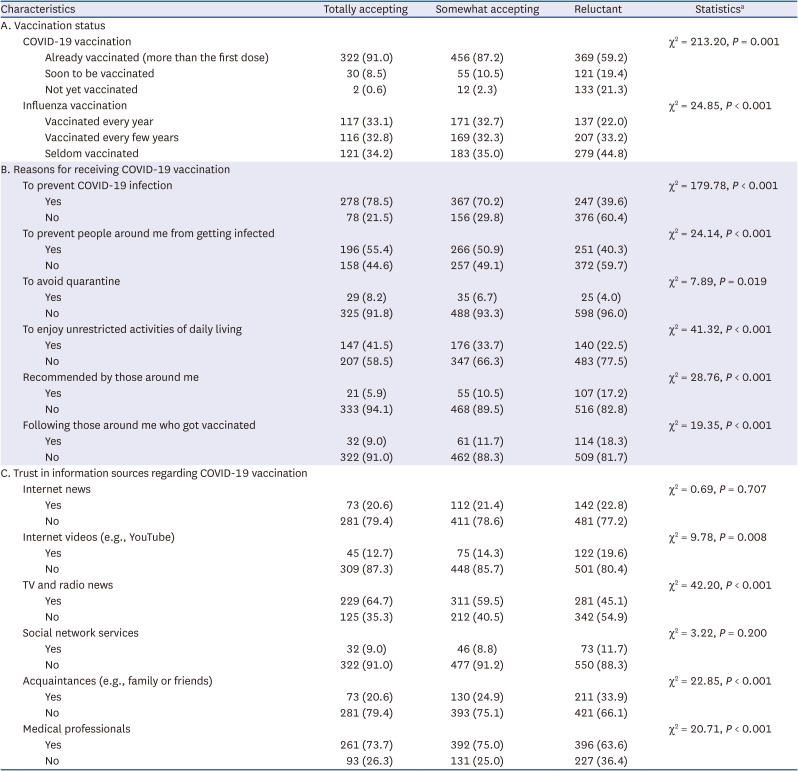
The participants in the ‘totally accepting’ and ‘somewhat accepting’ groups were more likely to state that preventing infection and unrestricted activities of daily living were the major reasons for receiving a COVID-19 vaccine compared to those in the ‘reluctant’ group (Table 3). However, the proportion of those participants who had been vaccinated against their will was significantly higher in the ‘reluctant’ compared to the ‘totally accepting’ group.
About 60–70% of the participants in the ‘totally accepting’ and ‘somewhat accepting’ groups stated that they trusted the information related to COVID-19 vaccination presented on TV and radio news, as well as by medical professionals (Table 3). However, in the ‘reluctant’ group, the proportion of participants who trusted these sources of information was significantly lower than in the other two groups, whereas the proportion of those who had more trust in information obtained from internet videos or acquaintances was significantly higher.
Psychological characteristics associated with COVID-19 vaccine acceptance
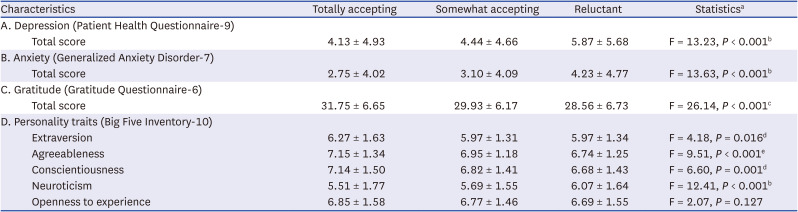
The total PHQ-9 and GAD-7 scores were significantly different among the three groups (PHQ-9: F = 13.23, P < 0.001; GAD-7: F = 13.63, P < 0.001). The participants in the ‘reluctant’ group experienced higher levels of depression and anxiety compared to the ‘totally accepting’ and ‘somewhat accepting’ groups (Table 4).
Table 4
Psychological characteristics associated with vaccine acceptance
Data are presented as the mean ± standard deviation or numbers (%).
aQuade’s nonparametric analysis of covariance (included age as a covariate).
bTotally accepting, Somewhat accepting < Reluctant.
cTotally accepting > Somewhat accepting, Somewhat accepting > Reluctant, Totally accepting > Reluctant.
dTotally accepting > Somewhat accepting, Reluctant.
eTotally accepting, Somewhat accepting > Reluctant.
The total GQ-6 score was significantly different among the three groups (F = 26.14, P < 0.001; Table 4). Post hoc tests showed that the ‘totally accepting’ group had the highest level of gratitude, followed by the ‘somewhat accepting’ group and the ‘reluctant’ group.
For the BFI-10 scores, significant differences in extraversion (F = 4.18, P = 0.016), agreeableness (F = 9.51, P < 0.011), conscientiousness (F = 6.60, P = 0.001), and neuroticism (F = 12.41, P < 0.001) were observed among the three groups (Table 4). Post hoc tests showed that the levels of extraversion and conscientiousness were higher in the ‘totally accepting’ than in the ‘somewhat accepting’ and ‘reluctant’ groups, and the level of agreeableness was higher in the ‘totally accepting’ and ‘somewhat accepting’ groups than in the ‘reluctant’ group. The level of neuroticism was higher in the ‘reluctant’ group than in the ‘totally accepting’ and ‘somewhat accepting’ groups.
DISCUSSION
In this study, we investigated the attitudes toward COVID-19 vaccination in the Korean general population, and categorized individuals according to the degree of vaccine acceptance using clustering analysis. This study shows that more than half of the participants were willing to receive a COVID-19 vaccine and perceived it as efficacious and necessary. We also identified several behavioral and psychological characteristics associated with COVID-19 vaccine acceptance and hesitancy.
Clustering is an exploratory analytical technique used to identify subgroups of individuals within a larger population who share similar characteristics.32 Hierarchical clustering constructs a dendrogram of nested clusters by repeatedly merging or splitting clusters.33 In the absence of a validated tool for assessing vaccination behavior, we expected that clustering analysis would be a useful method to classify individuals according to COVID-19 vaccine acceptance. Felten et al.34 categorized patients with autoimmune and inflammatory diseases into three main patterns according to beliefs and intentions related to COVID-19 vaccination using cluster analysis. That study also showed that COVID-19 vaccine hesitancy among immunocompromised patients was related to specific concerns about the use of new vaccine technology, lack of long-term data, and potential financial links between governments and pharmaceutical companies, but not the fear of contracting COVID-19.34
In the present study, hierarchical clustering identified three main attitudes toward COVID-19 vaccination in the Korean general population: ‘totally accepting,’ ‘somewhat accepting,’ and ‘reluctant.’ Most participants in the ‘totally accepting’ group strongly agreed that COVID-19 vaccines are efficacious and necessary, and expressed a high willingness to be vaccinated. Additionally, many participants in the ‘somewhat accepting’ group were somewhat willing to be vaccinated and agreed with the necessity of vaccination. However, a considerable proportion of participants in the ‘totally accepting’ and ‘somewhat accepting’ groups were also concerned about the potential side effects of the COVID-19 vaccines. The ‘totally accepting’ and ‘somewhat accepting’ groups included approximately 60% of all participants, which is similar to or slightly lower than the vaccine acceptance rates in other studies conducted in Western countries.353637 In contrast, most participants in the ‘reluctant’ group were lukewarm, hesitant, or resistant to receive the COVID-19 vaccine, and were also highly concerned about side effects. Hwang et al.12 conducted a study in late 2020 showing that about 40% of the population hesitated or refused to receive the COVID-19 vaccine in Korea, which is largely in agreement with our findings. These data suggest that COVID-19 vaccine acceptance may be categorized according to beliefs regarding its efficacy and necessity, as well as concerns about side effects.
The participants in the ‘totally accepting’ group were the oldest and those in the ‘reluctant’ group were the youngest among the three groups. This finding is largely consistent with those of recent studies showing that older people were more willing to get vaccinated.38 The higher vaccine acceptance seen in older patients may be explained by their awareness of worse COVID-19 outcomes in the unvaccinated.39 However, we found no significant difference in sex among the three groups. Results regarding sex differences in vaccine acceptance have been inconsistent, but some studies have reported higher vaccine hesitancy in women, which was likely due to some reports of fatal vaccine side effects in women.40 In addition, we found no difference in occupational status or education level among the three groups.
The COVID-19 vaccination rate reached about 90% in the ‘totally accepting’ and ‘somewhat accepting’ groups, but was less than 60% in the ‘reluctant’ group. At the time of this survey (mid-September 2021), about 70% of the entire Korean population had received more than the first dose of a COVID-19 vaccine.25 The high vaccination rate in those who were accepting of vaccination indicates that an accepting attitude toward COVID-19 vaccines could eventually lead to vaccination. In addition, we considered that there might be a considerable number of individuals who remained lukewarm or reluctant about vaccination even though they had been vaccinated. Coercive measures, such as a vaccine pass, only forced individuals to get vaccinated but might not essentially change the negative attitude toward vaccination.41 The fact that many individuals today are unwilling to receive omicron-containing booster vaccines supports this assumption.
The ‘reluctant’ group had the lowest rate of previous influenza vaccination as well as current COVID-19 vaccination, suggesting that existing perceptions and attitudes toward vaccination might play important roles in the decision to receive a COVID-19 vaccine. We assumed that an individual’s predisposition may underlie vaccine hesitancy for COVID-19 and influenza vaccines in common. Recent studies have reported a correlation between COVID-19 vaccine acceptance and influenza vaccine uptake.4243 A systematic review also pointed out concerns over safety, lack of trust, lack of need for vaccination, and cultural reasons as common causes of vaccine hesitancy for COVID-19 and influenza vaccines.44
Among participants who were accepting of COVID-19 vaccination, preventing COVID-19 infection and exemption from restrictions on daily life were important factors in the decision to be vaccinated. This shows that in addition to preventing infection and reducing mortality, the benefits of vaccination for daily life may be important in the decision to be vaccinated.45 However, participants who were reluctant to get vaccinated more often responded that they would get the COVID-19 vaccine because of recommendations or trends of their acquaintances, not because of their will. Hwang et al.12 indicated that the most common reason for vaccine hesitancy in Koreans was a lack of confidence in the COVID-19 vaccines.
Participants who exhibited high vaccine acceptance considered traditional mass media and medical professionals as reliable information sources. However, participants who were reluctant to receive the COVID-19 vaccine had less trust in these information sources, but they were more likely to trust information obtained from internet videos or acquaintances than those who were accepting of vaccination. Tan et al.46 reported that trust in formal rather than informal sources of information was associated with complete vaccination among middle-aged and older individuals. In contrast, some studies have shown that social media use could increase vaccine hesitancy.47 Providing appropriate professional medical information through formal mass media and informal internet media (e.g., YouTube) is required to promote public health.48
Taken together, our findings suggest that encouraging positive perceptions and attitudes toward COVID-19 vaccines can increase the likelihood of COVID-19 vaccination. The provision of appropriate information on COVID-19 vaccination by medical professionals and mass media is important to enhance vaccine acceptance. It is necessary to establish public health strategies that can effectively communicate the necessities and benefits of COVID-19 vaccines to improve individuals’ awareness of vaccination.
Participants who were reluctant to receive the COVID-19 vaccine were more likely to be depressed and anxious than those who were accepting of vaccination. This is largely consistent with the findings of Sekizawa et al.49 who showed that depression and generalized anxiety were associated with unwillingness and indecisiveness to get vaccinated against COVID-19. Depressed or anxious individuals are likely to become ambivalent, have reduced adaptive coping resources, and are reluctant to take preventive actions against COVID-19.24 Conversely, vaccination may reduce the perceived risk of COVID-19 and associated psychological distress.50
The more accepting the participants were of COVID-19 vaccination, the higher the level of gratitude. Gratitude is a general state of thankfulness and appreciation in response to the receipt of something valuable and meaningful.51 Gratitude improves adaptive coping in the face of adversity.52 In particular, it was associated with better mental health during the COVID-19 pandemic, including less depression and anxiety, as well as a higher level of subjective well-being.5354 The role of gratitude in reducing anxiety and depression, which are associated with reluctance to receive the vaccine, may positively affect vaccination behavior. Although little is known regarding the effects of gratitude on vaccination behavior during the pandemic, we assume that grateful individuals would cope better with concerns about the new COVID-19 vaccines. In addition, gratitude may be associated with an altruistic attitude, which is a potential reason for getting vaccinated.55
Participants who exhibited high vaccine acceptance had higher levels of extraversion, agreeableness, and conscientiousness as well as less neuroticism compared to those who were reluctant to be vaccinated. Extraversion is a personality trait characterized by sociability, assertiveness, and high emotional expressiveness; individuals high in extraversion are outgoing and enthusiastic.56 Agreeableness refers to an individual’s level of cooperativeness and compassion; individuals with a high level of agreeableness are more likely to be warm, caring, and supportive toward others.57 Conscientiousness is a personality trait that reflects the tendency to be responsible, hard-working, goal-directed, and to adhere to rules; high conscientiousness means an individual is responsible and reliable.58 In contrast, neurotic individuals are characterized by anxiety, sadness, and emotional instability; individuals with a high level of neuroticism feel more depressed, impulsive, and insecure.59 A national survey conducted before the COVID-19 pandemic in the US found that individuals high in agreeableness and conscientiousness were more likely to regard vaccination as beneficial, highlighting the importance of personality in shaping individual vaccination behavior.60 Recent studies since the COVID-19 outbreak have also shown that personality traits, such as agreeableness, conscientiousness, and neuroticism, are associated with COVID-19 vaccine acceptance and hesitancy.116162
Taken together, our findings suggest that the psychological state and traits of individuals play an important role in the willingness or reluctance to receive the COVID-19 vaccine. In this regard, we must consider individual psychological factors to understand and resolve anti-vaccination behavior, including vaccine hesitancy or refusal.
This study had some limitations. First, because the study population was grouped using clustering analysis rather than based on cutoff scores or criteria, the differences in vaccine acceptance among the ‘totally accepting,’ ‘somewhat accepting,’ and ‘reluctant’ groups were not definite or conclusive. In particular, the ‘reluctant’ group may be a heterogeneous population, such as individuals who were lukewarm, hesitant, or resistant to vaccination. The socio-demographic characteristics of the study population may also influence clustering. As a result, different classifications of vaccine acceptance may be feasible when using a data-driven approach, depending on the study population or the investigator’s judgement. Second, this study did not address various factors that may be associated with vaccination behavior, including economic status, political ideology, and religious affiliation. Third, this study was conducted during the COVID-19 vaccination program; the phased nature of the program should be considered when generalizing the results.
In conclusion, more than half of individuals were willing to receive the COVID-19 vaccine, while a considerable number remained lukewarm or reluctant about vaccination. In particular, many individuals were concerned about side effects regardless of whether they were accepting of COVID-19 vaccination or not. Individuals may differ in their perceptions of the efficacy and necessity of COVID-19 vaccines, and weigh the benefits and risks of vaccination in different ways; these factors may influence vaccine acceptance and hesitancy. Psychological states and traits, such as depression, gratitude, and personality, also play important roles in attitudes and decisions about COVID-19 vaccination. Understanding the role of coping mechanisms and psychological characteristics in vaccination behavior could aid in establishing effective public communication strategies to encourage COVID-19 booster vaccinations.
 XML Download
XML Download