

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a mild disease which usually starts with respiratory complaints and is sometimes mortal due to multiple organ failure secondary to the uncontrolled inflammatory response it triggers. Inflammation, organ damage, and death due to viral infection in patients with COVID-19 may occur directly from the cytotoxic effect of the virus, from secondary damage from an immune response triggered by the pathogen, or from pathogen-induced immunosuppressive response.12
The hyperinflammatory status is a recognized component of COVID-19 and is associated with organ dysfunction, disease severity, and death.34 Many agents were used to control the dysregulated inflammatory response in COVID-19 patients, and steroids are one of these agents. Different types and doses of steroids were used for this purpose. However, there is no common consensus. Conflicting results were reported in several randomized controlled trials (RCTs) using high-dose methylprednisolone.56 Some researchers said that higher doses of steroids, including pulse dose, are associated with good results.78 Fatal COVID-19 most commonly occurs with severe hypoxemia, and treatment with corticosteroids was shown to reduce mortality in these conditions.910 There are also studies which report that the use of high-dose (80 mg and above) steroids is associated with increased mortality.11
While corticosteroids are beneficial in critically ill COVID-19 patients, the precise threshold of illness at which corticosteroids should be administered remains unclear. In particular, it is unclear whether corticosteroids are beneficial in mild patients.12 Due to the different results in studies, the most appropriate type of corticosteroid, dose, and time of initiation in COVID-19 are still unclear.
The aim of this multicenter retrospective study is to determine whether the types of steroids (dexamethasone and methylprednisolone), doses, administration time and duration used in the treatment of COVID-19 patients are associated with an improvement in the outcome of these patients.
METHODS
Study design and inclusion criteria
Subsequently, the files of the patients who were admitted to the intensive care unit (ICU) due to COVID-19 between March 2020 and September 2021, who were diagnosed with polymerase chain reaction (+) and/or clinically and radiologically, were reviewed retrospectively. The study was carried out with the participation of 6 training and research hospitals which collected the data. Patients who are over the age of 18 who received steroid therapy for more than 3 days, were intubated or not, had a PaO2/FiO2 (P/F) ratio of < 300 in arterial blood gas, met the criteria for mild, moderate and severe ARDS, and had PCR(+) or had clinical and radiological diagnosis of COVID-19 were included to the study. The ARDS was diagnosed according to the Berlin definition criteria. Patients who took another immunosuppressive agent with or before steroids, those who used steroids for less than 3 days, patients who died or were discharged before 3 days, pregnancy or active breastfeeding, neutropenic, recent history of chemotherapy, and patients who had deficiencies in blood gases and laboratory data at first admission were excluded from the study.
Data collection
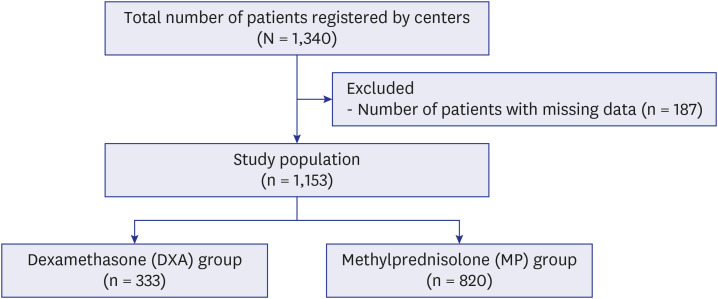
A secure database was created by the authors to record the data and sent to all centers. Using this data collection template, which was previously created by the principal investigators at the centers participating in the study, detailed data were collected on adult patients admitted to intensive care due to COVID-19. Demographic data and comorbidities of the patients, and laboratory data on the first day (day 0) and day 10 of their admission to the ICU (day of exit if exitus or discharged before the 10th day) Sequential Organ Failure Assessment (SOFA) score, PaO2/FiO2 (P/F) ratio, D-dimer, fibrinogen, ferritin, lymphocyte and C-reactive protein (CRP) levels, medications used, length of stay in the ICU and discharge patterns were recorded. In cases where infection occurred in the patients, endotracheal aspirate, blood and urine cultures were recorded. Antibiotics started according to both empirical and culture results were recorded. The data collected and sent by the centers in accordance with the data collection criteria were reviewed by a trained team of physicians (Fig. 1).
Grouping
The patients included in the study were divided into two main groups as dexamethasone and methylprednisolone according to the steroid types they used. Patients receiving methylprednisolone were divided into 3 subgroups according to the doses used in the treatment: pulse (500 mg and above/day; pulse MP group), mini-pulse (250 mg/day; mini-pulse MP group) and standard (1–2 mg/kg/day; standard dose MP group). Dexamethasone group (DXA group); Patients who received treatment at a dose of 6–16 mg/day for at least 3 days constituted the second group.
Primary and secondary endpoints
The primary endpoint of our study was to reveal the effects of methylprednisolone and dexamethasone on mortality. The secondary endpoint was the comparison of the effects of these agents on ICU length of stay and infections.
Statistical analysis
The data were evaluated in the R 4.1.1 package statistics program. The number of units, percent (%), mean ± standard deviation (x̄ ± ss), and median (Q1–Q3) values were given as descriptive statistics. Pearson χ2 and Fisher’s exact tests were used to evaluate categorical variables. The normal distribution of the data of continuous variables was evaluated with Shapiro-Wilk, normality test and QQ charts. In the comparison of continuous variables of the two groups, the Independent Sample t-test was used for normally distributed variables, and the Mann-Whitney U test for non-normally distributed variables. For comparison of continuous variables of three or more groups, homogeneity of variances in normally distributed variables was examined using Levene’s test. One-way analysis of variance was used if the distribution of variances was homogeneous, and the Welch test was used if the distribution of variances was not homogeneous. Kruskal-Wallis analysis was used for non-normally distributed variables. As a multiple comparison test, Tukey’s honestly significant difference was used if the variances were homogeneous in normally distributed variables, Games-Howell test was used if the variances were not homogeneous, and Dunn-Bonferroni test was used for non-normally distributed variables. Non-parametric two-way factor analysis was used to evaluate P/F ratio, SOFA score and laboratory parameters on the first day and on the 10th day.13
RESULTS
Our study was carried out by scanning the files of patients who were admitted to the intensive care unit due to COVID-19 in 6 centers between March 2020 and September 2021, and who had never received steroid treatment before, and recording the data of 1,340 patients who were eligible for the study. The collected data were re-evaluated before statistical analysis, and 187 patients with missing data and not meeting the study criteria were excluded from the study. A total of 1,153 patients, including 667 (57.8%) males and 486 (42.2%) females, who met the inclusion criteria were included in the study.
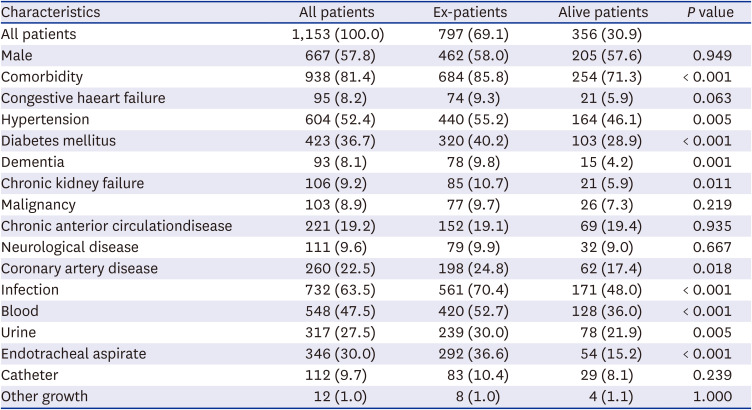
When the patients were evaluated in terms of demographic data, no relationship was found between gender and mortality. However, the presence of at least one comorbidity was associated with mortality, and especially hypertension, diabetes mellitus, chronic kidney failure, coronary artery disease, and dementia were found to be statistically significantly higher in patients who died than in those who survived. In the follow-up of the patients, the detection of infection proven by culture growth was associated with mortality. Significantly higher growth was observed in blood, urine and eta cultures taken from the ex-patient group. The most common causative agents were Acinetobacter 267 (23.2%), Klebsiella pneumonia 197 (17.1%) and Staphylococcus aureus 136 (11.8%) (Table 1).
Table 1
Distribution of patients’ demographic, comorbidity and infection rates
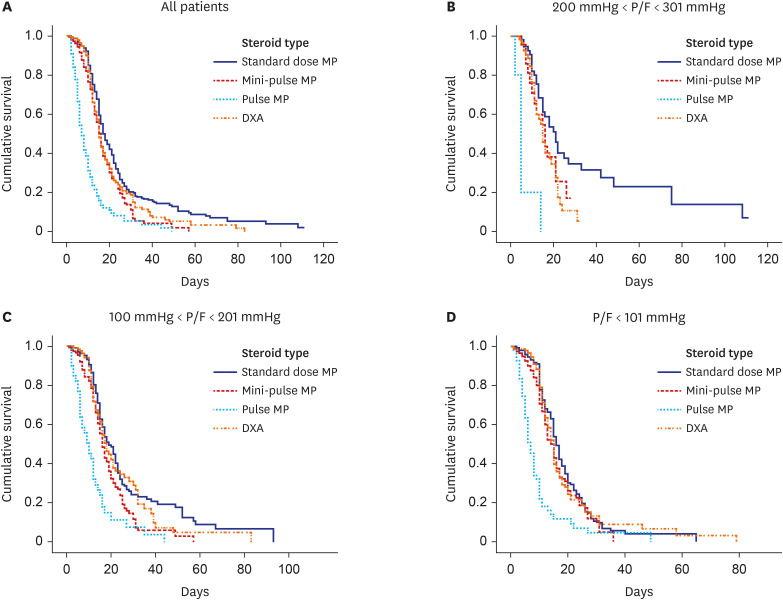
When the relationship between steroid use and mortality was examined, mortality in the pulse MP group was statistically significantly higher than the other 3 groups (P > 0.001). When the patients were analyzed by dividing them into 3 different groups according to their P/F ratios, Standard dose MP and DXA treatment survival was significantly higher than pulse MP group (P < 0.001). When the middle patient group was examined, survival was significantly higher in standard dose MP and DXA groups than pulse MP and mini-pulse MP groups. There were no significant differences between standard dose MP and DXA groups or mini-pulse MP and pulse MP groups (P < 0.001). Survival time was significantly shorter in pulse MP group than standard dose MP, DXA, and mini-pulse MP groups, there were no significant differences between Standard dose MP, DXA and mini-pulse MP in severe group (P < 0.001) (Fig. 2).
Fig. 2
Effect of steroid doses on survival times in ARDS groups. (A) All patients. (B) Mild ARDS. (C) Moderate ARDS. (D) Severe ARDS.
MP = methylprednisolone, DXA = dexamethasone, ARDS = acute respiratory distress syndrome, P/F = PaO2/FiO2.
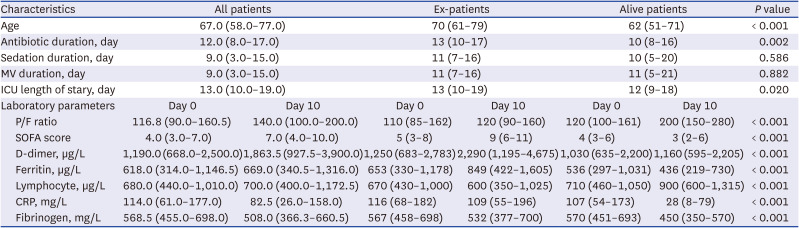
The age of the ex-patients was statistically significantly higher than the living patients (P < 0.001). Antibiotic treatment and ICU length of stay of patients with Ex were statistically significantly higher than the surviving patients (P = 0.002 and P = 0.020, respectively). In terms of sedation and MV times, no significant difference was found between patients who died and those who survived (P = 0.586 and P = 0.882, respectively). The increase in the 0 and 10 days P/F ratios of the surviving patients was significantly higher than the ex-patient group (P < 0.001). While SOFA scores increased on the 10th day compared to day 0 in the patient group with ex, the SOFA value on the 10th day decreased compared to the 0th day in the surviving patient group. The difference of SOFA score at 0 and 10 days was significantly different in both groups (P < 0.001). While D-dimer levels increased approximately 2 times in the patient group with ex, compared to the first measured value, it showed a minimal increase in the living patient group, and this difference was statistically significant (P < 0.001). While ferritin levels increased in the patient group with ex, they decreased in the living patients. This change in ferritin values was statistically significant in both groups (P < 0.001). In the ex-patient group, lymphocyte values decreased on the 10th day compared to day 0, while it increased in the living patient group. The trend of lymphocyte values was statistically significantly different in both groups (P < 0.001). Considering the day 0 and 10th day values of CRP, a slight decrease was observed in ex-patient group, while a greater decrease was observed in the living patient group. Considering the fibrinogen levels, the decrease rate in the living patient group was statistically significantly higher than in the ex-patient group (P < 0.001) (Table 2).
Table 2
Relationship between living and deceased patients’ age, clinical follow-up period and laboratory parameters measured on the 0th and 10th days
When the patients were divided into 4 groups according to the steroid doses used in the treatment, the median age of the patients in the mini-pulse MP group was significantly higher than in the DXA group (P = 0.011). The duration of antibiotic treatment received by the patients in the standard dose MP group was statistically significantly longer than the mini-pulse MP, pulse MP and DXA groups (P < 0.001). Sedation, MV and ICU stays of the patients in the pulse MP group were statistically significantly shorter than in the Standard dose MP, mini-pulse MP and DXA groups (P < 0.001). The duration of sedation was significantly longer in the standard dose MP group than in the DXA group (P < 0.001). In addition, the duration of ICU stay and MV in the standard dose MP group was statistically significantly longer than in the mini-pulse MP and DXA groups (P < 0.001).
The increase in SOFA score in the pulse MP group; standard dose MP was statistically significantly higher than mini-pulse MP and DXA groups (P = 0.013). The increase in D-dimer value was statistically significantly higher in the pulse MP, mini-pulse MP and DXA groups compared to the Standard dose MP group (P = 0.024). There was no statistically significant difference between the change in CRP levels and steroid groups (P = 0.012). The increase in ferritin levels was statistically significantly higher in the pulse MP group than in the mini-pulse MP, standard dose MP and DXA groups. In addition, ferritin values increased significantly more in the mini-pulse MP group than in the standard dose MP and DXA groups (P = 0.012). When the rate of change in lymphocyte count was examined, a decrease was observed in the pulse MP group, while an increase was observed in the standard dose MP, mini-pulse MP and DXA groups. The rate of change in lymphocyte counts differed significantly in the pulse MP group compared to the standard dose MP, mini-pulse MP and DXA groups (P = 0.001) (Table 3). While it increased in all steroid treatment groups in patients who experienced the change in lymphocyte count between days 0 and 10, it decreased in patients who died. Such a difference was not observed in other laboratory parameters. Therefore, it can be said that lymphocyte count can be used as a marker in determining the prognosis by distinguishing it from other laboratory parameters (Table 3).
Table 3
Relationship between steroids, age, duration of clinical follow-up, and laboratory parameters measured on days 0 and 10
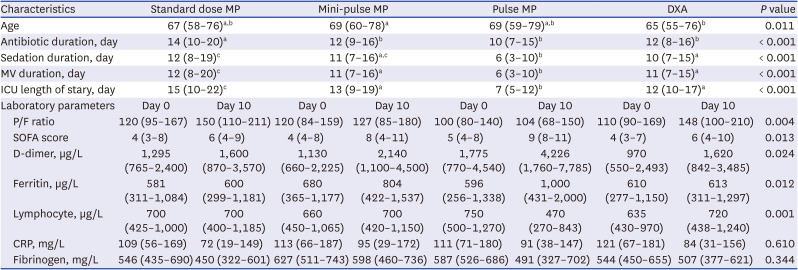
Values are presented as median (Q1–Q3).
MP = methylprednisolone, DXA = dexamethasone, MV = mechanical ventilation, ICU = intensive care unit, P/F = PaO2/FiO2, SOFA = Sofa Sequential Organ Failure Assessment, CRP = C-reactive protein.
a-cLetters a-c were used to indicate groups with statistically significant differences. There was no statistical difference between groups with the same letters.
In terms of infection, there was no statistically significant difference in the development of infection in all steroid groups (P = 0.103). There was no significant difference between the cumulative steroid dose received by the patients and the development of infection (P = 0.225). However, there was a statistically significant difference between the duration of steroid treatment and the development of infection (P < 0.001).
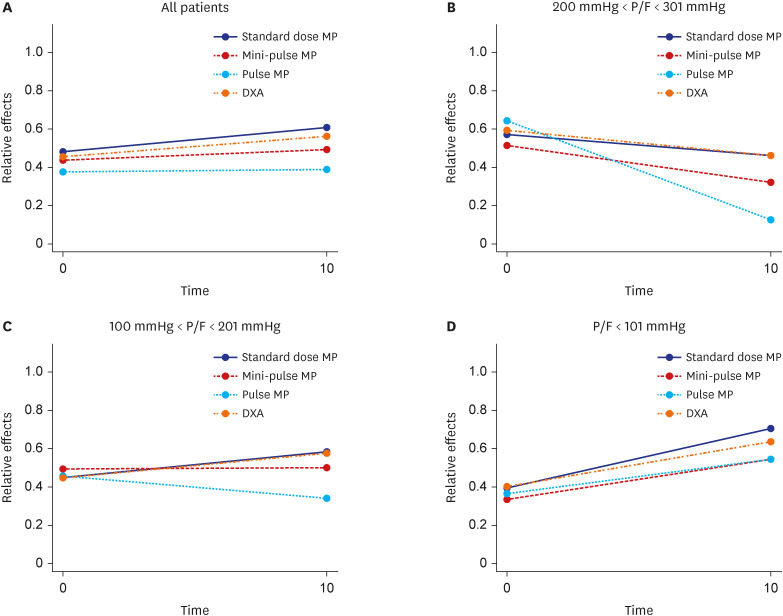
Considering the changes in P/F ratios without grouping, P/F ratios increased in all steroid treatment groups. The increase in P/F ratio was significantly higher in the standard dose MP group than in the mini-pulse MP and pulse MP groups (P = 0.001 and P = 0.002, respectively). Again, the increase in the P/F ratio was significantly higher in the DXA group than in the mini-pulse MP and pulse MP groups (P = 0.038 and P = 0.017, respectively) (Fig. 3A). When the groups were analyzed within themselves, a decrease in P/F ratios was found in all steroid treatment groups in mild patients. The decrease in this rate was statistically significantly higher in the pulse MP group than in the standard dose MP, mini-pulse MP and DXA groups (P < 0.001, P = 0.017, and P = 0.001, respectively) (Fig. 3B). When the middle patient group was examined, the P/F ratio increased in the standard dose MP and DXA groups, while the P/F ratio decreased in the mini-pulse MP and pulse MP groups. The P/F ratio in the intermediate patient group was statistically significantly different in the standard dose MP and DXA groups compared to the mini-pulse MP and pulse MP groups (P = 0.001, P < 0.001 and P = 0.007, P < 0.001). In addition, the decrease in P/F ratio in the pulse MP group was statistically significantly higher than in the mini-pulse MP group (P = 0.028) (Fig. 3C). When the severe patient group was examined, an increase in the P/F ratio was found in all steroid treatment groups. This increase was statistically significantly higher in the standard dose MP group than in the mini-pulse MP, pulse MP, and DXA groups (P = 0.010, P = 0.013, and P = 0.021, respectively) (Fig. 3D).
DISCUSSION
In our study, we tried to determine the effects of steroids type, dose, and onset time on mortality. We found that the effects of dexamethasone and standard dose methylprednisolone were similar, and pulse steroid doses were significantly associated with mortality.
The current hypothesis regarding pathology in COVID-19 patients is that lung damage is not directly related to the virus, that virus-induced immune and inflammatory responses lead to activation of immune cells, and that these responses occur due to secretion of multiple pro- and anti-inflammatory cytokines including tumor necrosis factor-α, interleukin (IL)-1β, and IL-6.14 Corticosteroids are classical immunosuppressive drugs that suppress the immune response, decrease the number and activity of T lymphocytes, and have anti-inflammatory properties. Methylprednisolone is an intermediate-acting product and is 5 times more potent compared to short-acting products (hydrocortisone), while Dexamethasone is a long-acting product and 25 times more potent compared to short-acting products.15 Because of these properties, corticosteroids have been used to control the dysregulated immune response in patients with COVID-19. Although many studies were carried out on this subject, the type, dose, duration of the steroid to be used and the stage of the disease to start are still not yet clear. Studies have shown that steroids used in mild cases of COVID-19 do not have positive effects on prognosis.12161718 In our study, we determined that all steroid groups caused a decrease in P/F ratios in the mild patient group. This decrease was especially severe in the mini-pulse MP (250 mg/day) and pulse MP (500 mg/day and above) groups. Therefore, we do not recommend the routine use of steroids in the mild patient group.
In the literature, there are studies reporting the effectiveness of dexamethasone in studies on the effectiveness of steroid types used in COVID-19 patients,1920 and there are also studies reporting the same opinion for methylprednisolone.521 In studies comparing the efficacy of the two drugs, it has been found that high-dose methylprednisolone is better than dexamethasone in improving the clinical condition, reducing the need for invasive ventilation, a shorter recovery time, and reducing the severity of inflammatory markers in COVID-19 patients.2223 Ko et al.24 found in their study that the effects of methylprednisolone and dexamethasone were similar, and that methylprednisolone was more effective only in the severely ill group. In our study, we reached similar results to the study of Ko et al.24 We found that methylprednisolone was more effective only in the severely ill group, where standard dose MP and dexamethasone had similar effects. In line with the current findings, we believe that the use of standard dose methylprednisolone in severe COVID-19 patients receiving MV therapy may be associated with better outcomes. One of the points we want to underline here is that the effects of pulse and mini-pulse MP are much less than standard dose MP and dexamethasone, and they even cause serious decreases in P/F ratios in mild and medium group patients.
Jamil et al.25 found that low-dose dexamethasone (6 mg/day) was associated with less mortality than methylprednisolone (500 mg/day) in their study in which they compared different doses and formulations of steroids with 433 patients. Monreal et al.26 compared high-dose (≥ 250 mg/day) and standard-dose (≤ 1.5 mg/kg/day) methylprednisolone in their study with 573 patients, and found the mortality rates to be 39% versus 18.6%, respectively, hence higher in the high-dose group. In their study where they compared low (0.5–1.0 mg/kg) (n = 21), moderate (1.0–2.0 mg/kg) (n = 19), and high (200–400 mg in 3 days) (n = 24) doses of methylprednisolone, Chen and Li27 found that there are no differences between the doses in terms of mortality. In our study, we found the mortality rates in the 3 methylprednisolone (standard dose, mini-pulse, pulse MP) and dexamethasone (DXA) groups to be 64%, 71.8%, 91%, and 63.9%, respectively. The results we found supported previous studies and revealed that high doses of methylprednisolone (pulse: 500 mg/day and above) were significantly associated with mortality. We found that the effects of standard dose MP and dexamethasone on mortality were similar. When we grouped the patients according to their P/F ratios and looked at the effects of steroid types and doses on mortality, we found that mortality was high in patients who were administered pulsed dose of methylprednisolone, except for the mild patient group. We believe that the mild patient group did not reach a statistically significant level since the number of cases in the group was very low.
Laboratory parameters are also used in estimating the efficacy of treatments and mortality in COVID-19 patients. Bivona et al.28 revealed in their study that D-dimer is a useful indicator of the course of serious disease. Again, Kim et al.29 found that lymphopenia is more common in severe cases. Soliman et al.30 conducted a study with 60 patients in which they compared the effects of dexamethasone (8 mg/day) and methylprednisolone (1 mg/kg/day) on laboratory parameters, and found that methylprednisolone decreased the neutrophil-lymphocyte ratio and CRP level more than dexamethasone does, and that its effects on D-dimer and ferritin were similar. This study also revealed that methylprednisolone reduced mortality more. Pinzón et al.22 compared dexamethasone (8 mg/day) and high-dose methylprednisolone (250–500 mg/day) in their study. They reported that high-dose methylprednisolone lowered CRP, D-dimer and ferritin levels more, and that high-dose methylprednisolone had better effects on mortality. In our study, D-dimer and ferritin levels increased in all groups. However, the increase in the pulse MP group with the highest mortality was statistically significantly higher than the other groups. Again, the decrease in lymphocyte count was statistically significantly higher in this group. We think that the decrease in the lymphocyte count as well as the elevation of D-dimer and ferritin may be useful in predicting the mortality as well as the effectiveness of the treatment. When we analyzed the lymphocyte count in line with the results we found, it increased in all steroid treatment groups in patients who experienced the change between days 0 and 10, while it decreased in patients who died. Such a difference was not observed in other laboratory parameters. Therefore, it can be said that lymphocyte count can be used as a better predictor in determining the prognosis by distinguishing it from other laboratory parameters.
In literature, there are studies reporting different results that steroids prolong3132 or shorten1933 the length of stay in ICU. In our study, the average hospital stay was 7 days in the pulse MP group with the highest mortality, and it was longer1215 days in the other groups. Although the general opinion is that steroids increase infections in terms of their effects on secondary infections,333435 there are studies which report the opposite.3637 Oh et al.38 in their study to compare COVID-19 patients receiving and not receiving steroids, found that bilateral pneumonia (76.5% vs. 27.2%) and antibiotic use (79.3% vs. 4.3%) were higher in the steroid group. They also found the rates of antibiotic use in patients receiving high and low-dose steroid therapy, respectively (94.7% vs. 76.0%). Na et al.39 found the rate of secondary infection in COVID-19 patients to be 70.2% in their study. They found the mortality rate in patients with secondary infection to be 2 times higher. They stated that mechanical ventilation, high frailty scale and steroids were effective as risk factors. The most common causative agents were Acinetobacter baumannii (23/73, 31.5%), Klebsiella species (16/73, 21.9%) and Streptococcus species (14/73, 19.2%). We found similar results in our study.
In our study, we found the secondary infection rate to be 732 (63.5%). There was no statistically significant difference in the development of infection in all steroid groups (P = 0.103). There was no statistically significant difference between the cumulative steroid dose received by the patients and the development of infection (P = 0.225). However, there was a statistically significant difference between the duration of steroid treatment and infection development (P < 0.001). We found the most common causative agents Acinetobacter baumannii 267(23.2%), Klebsiella pneumonia 197(17.1%) and S. aureus 136(11.8%). In our study, we found that the infection rate in patients who died was statistically significantly higher in 561 (70.4%) than in patients who survived 171 (48.0%). This shows us that secondary infections caused by steroids are an important factor on mortality.
In conclusion, although corticosteroids have been shown to be beneficial in critical COVID-19, the role of early corticosteroids in mild COVID-19 patients remains unclear. We found that all steroid groups used in the mild patient group caused a decrease in the P/F ratio. The anti-inflammatory effects of corticosteroids may have a positive effect by reducing mortality in severe cases of COVID-19. Although dexamethasone was first used for this purpose, methylprednisolone was found to be as effective as dexamethasone at standard doses. More importantly, the use of methylprednisolone at standard doses was associated with greater improvement in P/F ratios than dexamethasone, especially in the severely ill group requiring mechanical ventilation therapy. High-dose corticosteroids were not associated with mechanical ventilation, ICU length of stay, and improvement in P/F ratios. High dose pulse steroid doses are closely associated with mortality, and it is recommended to use standard doses of methylprednisolone. The available evidence about steroids usage with COVID-19 patients is scant, and even systematic reviews and meta-analyses on this subject come to different conclusions. Therefore, we believe that well-designed randomized controlled trials are needed in the future to provide a more reliable basis for treatment recommendations.
 XML Download
XML Download