

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
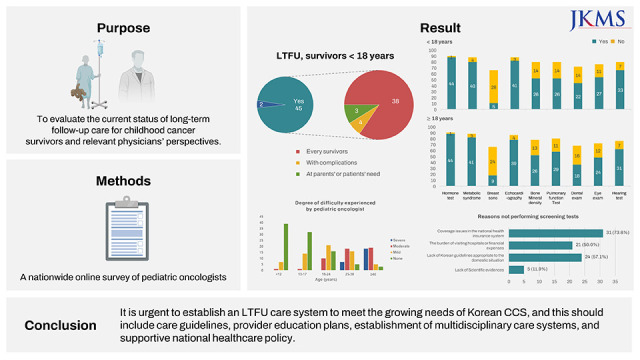
The treatment outcomes of childhood cancer have improved significantly over the past decades, and almost 70–80% of childhood cancer patients are cured.12 This improvement has resulted in a growing population of long-term childhood cancer survivors (CCSs). Although there are no accurate data, it is estimated that there are approximately 30,000 CCSs in Korea. Many studies have shown that chemotherapy and radiotherapy at a young age can affect multiple organ systems and cause various late effects or therapy-related sequelae, including organ dysfunction, neuroendocrine dysfunction, and secondary malignant neoplasm.345 The incidence of late treatment-related complications may differ depending on the cancer treatment modality and individual susceptibility. In Western countries, guidelines have been established to provide CCS with risk-based long-term health care.678910 For example, the Children’s Oncology Group developed clinical guidelines to increase awareness of potential late effects and to standardize and enhance follow-up care for CCSs.8 In this guideline, long-term follow-up (LTFU) for CCSs begins about two years after the end of treatment when patients are in remission and fully recovered from the previous therapy and continues throughout life. However, a standard protocol for LTFU care for CCS has not yet been developed in Korea, and data on the current status of LTFU care are lacking. Furthermore, there is no consensus on a follow-up strategy for adult CCSs, particularly given that pediatric hematologists/oncologists are unfamiliar with adult diseases that may occur in adult CCSs.
This nationwide survey of pediatric hematologists/oncologists was conducted to evaluate the current status of LTFU care for CCS and physicians’ perspectives on the LTFU care plan, especially for adult CCS.
METHODS
Study population and survey distribution
A list of board-certified pediatric hematologists/oncologists in South Korea was used to identify the potential participants. A total of 105 members were identified. Excluding members who were not currently working in the Korean pediatric hematology/oncologic field, 74 currently active members were identified as potentially eligible participants. An email was sent to all 74 members, with an invitation to participate in an online survey in September 2021.
Survey instrument
The investigators developed a survey instrument, which included 35 multiple-choice questions and one open-ended question (Supplementary Data 1). Some of the multiple-choice questions included text boxes to allow the respondents to provide additional comments or information. The questionnaire consisted of four different sections. In the first section, demographic characteristics of respondents such as age, sex, practice environment, and years of experience, were asked. The second and third sections queried participants regarding the current practice patterns for childhood and adolescent survivors (< 18 years in section 2) and adult survivors (≥ 18 years in section 3). These included questions regarding the duration and interval of the LTFU for CCSs, whether they transfer CCSs to nearby hospitals, institutional regular LTFU programs, and screening tests for the detection of late complications. In section 3, the additional question of whether they transfer adult CCSs to adult care physicians was also queried. In the fourth section, the degree of difficulty experienced by physicians according to the age of CCSs was asked. Questions regarding opinions about the desired direction and necessary national policy for an optimal LTFU care system in Korea were also included. In this survey, CCS was defined as patients diagnosed with pediatric cancer before 18 years of age and in remission for at least five years after completing primary cancer treatment. LTFU care was defined as care for CCS even five years after completing the primary cancer treatment.
RESULTS
Demographic data
A total of 47 pediatric hematologists/oncologists participated in the survey, with a response rate of 63.5%. The demographic characteristics of the respondents are summarized in Table 1. The distribution of sex and region of affiliated institutions did not differ between respondents and non-respondents. However, age distribution and years in clinical practice differed between respondents and non-respondents (P = 0.048 and P = 0.039, respectively). Among the respondents, the proportion of physicians aged 35–44 years and with 5–9 years of clinical practice was higher than that of non-respondents.
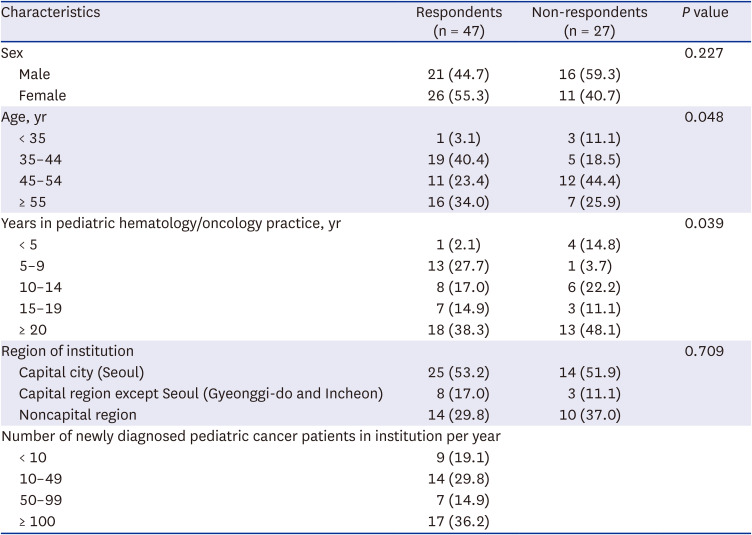
Table 1
Demographic characteristics of respondents
![]()
Regular follow-up schedule in survivors
Forty-five of the 47 respondents (95.7%) reported that they provided LTFU care for CCSs five years after the completion of primary cancer treatment. However, some of the 45 respondents did not provide LTFU care for every survivor. Thirty-eight (84.4%) respondents provided care to every childhood and adolescent CCS, and 33 (73.3%) provided care to every adult CCS. The remaining seven and 12 respondents answered that they provided LTFU care only for CCS with late complications or CCS requesting LTFU care, respectively.
The follow-up intervals were mostly every 6 or 12 months: 31.1% and 62.2% of pediatric hematologists/oncologists provided LTFU care to childhood and adolescent CCS at 6- and 12-month intervals, respectively, and 6.9% and 79.3% provided LTFU care to adult CCS at 6- and 12-month intervals, respectively. When queried about the endpoint of LTFU care for childhood and adolescent CCS, 7/45 (15.5%) respondents answered ten years after the completion of cancer treatment, 9/45 (20.0%) answered that they decided to stop LTFU care by considering both the patient’s age and the duration after the completion of treatment, and the remaining respondents (29/45, 64.4%) did not specify the endpoint of LTFU. For adult CCSs, 9/45 (20.0%) respondents answered that they continued to provide LTFU care until ten years (n = 8) or 20 years (n = 1) after the completion of treatment, and 34/45 (75.6%) respondents reported that the endpoints differed depending on the patients’ individual situations, including late complications (n = 18), treatment history (n = 8), or patients’ or parents’ needs (n = 8).
Fourteen (31.1%) respondents answered that they transferred a portion of childhood and adolescent CCSs to patients’ nearby hospitals for LTFU care, while 20 respondents (44.4%) answered that they transferred some adult CCSs. However, the proportion of CCSs transferred to nearby hospitals for LTFU care was less than 20%. The main reasons for continuing LTFU care for CCSs without transferring to nearby hospitals were the patients’ or parents’ preferences (n = 9), difficulties in delivering treatment summaries (n = 5), and inability to find physicians who are familiar with the LTFU care of CCSs (n = 3).
LTFU care programs
When asked if their center had an institutional regular LTFU care program for childhood and adolescent survivors, 26/45 (57.8%) respondents answered yes. Twenty-three respondents answered that the directors of the LTFU care programs were pediatric hematologists/oncologists. The other three responded that their LTFU care programs were operated by pediatric hematologists/oncologists and other specialists such as pediatric endocrinologists.
Regarding the main physician involved in LTFU care for adult CCSs, 20/45 (44.4%) responded that pediatric hematologists/oncologists were in charge of LTFU care, and 25/45 (55.6%) answered that they referred CCSs to adult care physicians for LTFU care. Adult CCSs were most frequently transferred to adult oncology (n = 7), followed by general internal medicine (n = 6) and family medicine (n = 6).
Screening tests for late complications
For screening examinations performed to detect late complications in CCSs with risk factors, the performance rate varied according to the type of test. More than 80% of the respondents reported conducting hormone tests, metabolic syndrome tests, echocardiography, and hearing tests if CCSs had risk factors (Fig. 1). Meanwhile, more than 20% of the respondents reported not performing bone mineral density tests, pulmonary function tests, and ophthalmologic examinations, even though the CCSs they cared for had risk factors. In particular, the rates of breast ultrasonography and dental examination were very low. These findings were similar, regardless of the age of the CCS.
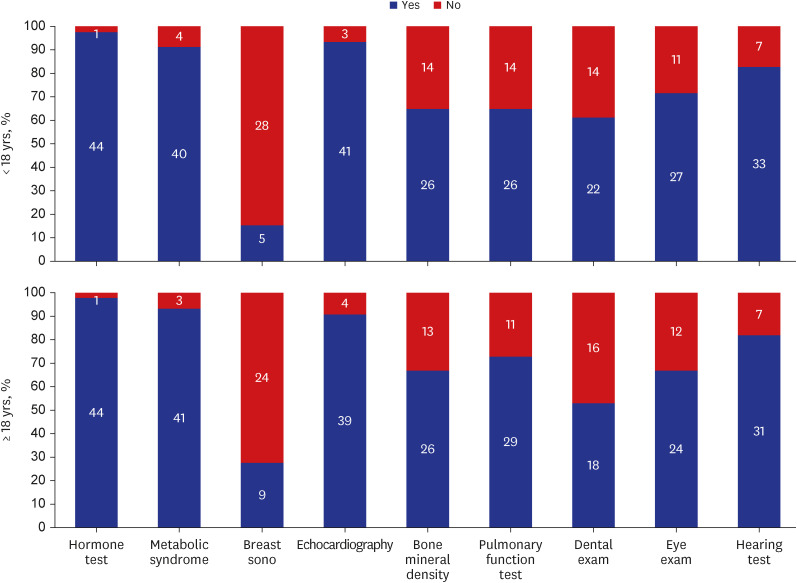
Fig. 1
Current status of screening tests that detect late complications. Many pediatric hematologists/oncologists did not perform screening tests, especially breast sonography, bone mineral density tests, pulmonary function tests, dental exams, and ophthalmologic exams, even though the CCS they cared for had risk factors for each complication.
CCS = childhood cancer survivor.
![]()
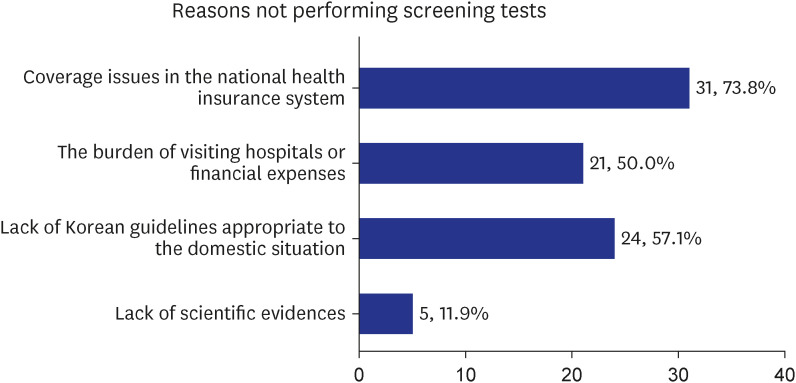
When we asked about the reasons for not performing screening tests for late complications, 31 out of 42 respondents (73.8%) answered that insurance coverage issues precluded these tests, and 24 (57.1%) indicated a lack of Korean LTFU guidelines for CCSs (Fig. 2).
A desirable LTFU care system in Korea
Pediatric hematologists/oncologists experience greater difficulties as the age of the CCS increases (Fig. 3). Regarding a desirable LTFU care system for CCSs in Korea, 27 of the 46 respondents (58.7%) answered that it is desirable to establish a multidisciplinary CCS care system in which pediatric hematologists/oncologists and adult physicians cooperate, whereas 12 (26.1%) preferred the establishment of a specialized LTFU care system run by the pediatric oncology group. When asked whether they were willing to actively participate in the management of adult CCSs, 38 of the 46 respondents (82.6%) answered yes. The remaining eight respondents responded that they did not intend to participate in the management of adult CCSs because of the burden of managing adult CCSs (n = 4), the burden of managing patients currently undergoing treatment (n = 3), and the lack of interest (n = 1).

When asked to give their opinion on what is most needed to establish an optimal LTFU care system for CCSs in Korea, 31 out of 47 respondents (66.0%) indicated that they wanted a Korean LTFU guideline for CCSs and 13 (27.7%) indicated reimbursement for the LTFU care service, such as multidisciplinary team care and LTFU plan establishment. Many respondents (53.2%) also suggested the need for additional insurance coverage for CCSs care over a long period to alleviate the financial burden on patients.
DISCUSSION
CCSs are a unique population that requires LTFU care because they are highly vulnerable to a range of health problems that develop later in life, because of early cancer treatment. Previous studies have shown that CCSs have a high risk of morbidity and early mortality from various health problems, such as secondary malignancies, cardiac problems, and pulmonary complications.1112131415 Almost 60–75% of patients who were CCSs had at least one chronic health condition, and 30–40% had at least one severe or life-threatening condition, showing the severe burden of adverse events in this population.1617 A recent study also showed that the cumulative incidence of severe or life-threatening chronic health conditions at 50 years of age was 96.0% in CCSs.3 Some chronic health conditions can develop after a long latency period, while others occur during or shortly after the cancer treatment.18 Given that CCSs can develop health problems over a lifelong period that are unique compared to the general population, CCSs need lifelong management within a special program. Despite the need for well-established LTFU care for CCSs, the findings of the present study suggest that many CCSs in Korea are not yet managed systematically and that the LTFU periods and methods may vary depending on the judgment of clinicians. This study showed that many CCSs receive LTFU care only for a certain period after the end of treatment, and in some situations, required tests that were not performed despite patients’ risks.
The lack of LTFU care guidelines suitable for the Korean domestic situation could be a significant cause of this problem. Several Western countries across North America and Europe have developed clinical practice guidelines for CCSs since the early 2000s.19202122 Efforts have been made to harmonize these guidelines internationally to enhance LTFU care of CCSs.2324 One of the barriers to implementing these guidelines into clinical practice is the complexity of the guidelines, which are different based on the individual treatment history. To overcome this, web-based electronic survivorship passport tools have been developed by a few groups.25 Even though there are international guidelines available, efforts are needed to modify the guidelines to reflect the domestic clinical situation and meet clinical needs. Many respondents in our study indicated that developing LTFU guidelines for CCSs is necessary to establish the LTFU care system in Korea. Accordingly, there is an urgent need to develop such guidelines and educate healthcare providers.
In the present study, 44.4% of respondents answered that they continued to provide LTFU care to adult CCSs aged over 18 years in the pediatric department, and 55.6% responded that they referred patients to internal medicine, adult oncology, or family medicine departments for problems other than primary or secondary cancers. Many pediatric hematologists/oncologists continue to provide follow-up care to adult CCSs because the LTFU care system for these individuals has not yet been established in Korea. Even when referrals are made to adult care clinics, there are more requests for follow-up of specific late complications than requests for comprehensive LTFU care. Furthermore, the present study also showed that pediatric hematologists/oncologists experienced greater difficulties providing LTFU care for CCSs in the older age group. Pediatric hematologists/oncologists can have knowledge deficits regarding health issues that may occur in adulthood, which can be a barrier to the delivery of good LTFU care for adult CCSs.
Transitional care, defined as the transfer of CCSs from pediatric- to adult-centered providers, has been studied in many countries.262728293031 However, the best model for delivering LTFU care to adult CCSs has not been established worldwide. There are adult cancer survivor programs in many institutions, but adult cancer survivor clinics differ from childhood cancer survivor clinics in several ways, including the patient population, type of cancers, and the frequent problems they are dealing with. A more specialized model having a multidisciplinary team of healthcare professionals is needed to provide comprehensive care for CCSs. The appropriate model may differ from country to country depending on the country’s healthcare system. One of the problems commonly presented in previous studies is the lack of available partnerships among adult healthcare providers. Establishing effective collaboration between pediatric and adult care providers is essential for delivering good LTFU care for adult CCSs. In this study, 58.7% of respondents indicated that a multidisciplinary system consisting of pediatric hematologists/oncologists and adult care physicians is desirable for establishing the LTFU care system for adult CCSs, and most of the respondents expressed their willingness to participate in the system. Based on the study findings, an ideal nationwide LTFU system model for adult CCSs should be established through further discussion.
One of the essential aspects of the LTFU care system is the need for reimbursement of comprehensive LTFU care services. A comprehensive LTFU care system should cover the development of an LTFU plan for each CCS, management of medical and psychosocial sequelae, delivery of interventions to prevent late effects, health screening, counseling, and education. To achieve this goal, a multidisciplinary team approach is critical, including pediatric hematologists/oncologists and adult care physicians and other specialists, including endocrinologists, nurses, and social workers. Without sufficient reimbursements, comprehensive LTFU care services cannot operate properly. Currently, reimbursement systems are limited or absent for many parts of this care, and healthcare policy changes and proper reimbursement will be required to support the appropriate LTFU care for CCSs.
The present study has some limitations. First, 36.5% of the initially targeted Korean pediatric hematologists/oncologists did not respond to the survey. Thus, the findings of our study may not fully represent the current situation of Korean CCSs’ care. To gain insight into the impact of this limitation, we compared the general characteristics of the respondents to those of all Korean pediatric hematologists/oncologists. Second, we collected study data based on the self-reports of pediatric hematologists/oncologists, instead of using direct observation data or objective clinical statistics. In addition, we surveyed individual physicians instead of institutions, while some survey questions were related to the institutional system, such as the LTFU care program. Therefore, our findings may underestimate or overestimate the current situation. However, the present study is the first to comprehensively evaluate the current status of Korean CCSs’ care and the perspectives of pediatric hematologists/oncologists on LTFU care through a nationwide survey.
In conclusion, the LTFU care system for CCS seems primitive in the Republic of Korea. It is urgent to establish an LTFU care system to meet the growing needs of the Korean CCSs, which should include care guidelines, provider education plans, the establishment of multidisciplinary care systems, and a supportive national healthcare policy.
 XML Download
XML Download