

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ductal carcinoma in situ (DCIS) accounts for approximately 30% of newly diagnosed breast malignancies.1 DCIS is a localized tumor within the ducts without invasion of the basement membrane. DCIS is associated with excellent survival rates. The 20-year cancer-specific mortality rate following a diagnosis of DCIS is 3.3%.2 Therefore, it is an important to reduce the incidence of complications caused by excessive treatment and to increase the quality of life for the patients with DCIS.
By definition, pure DCIS has no potential to spread to the axillary lymph nodes. Pure DCIS is associated with a rare incidence of lymph node metastasis.3 In a previous report, the incidence of axillary metastasis in pure DCIS was 0.5%.4 Other studies showed sentinel lymph node positivity rates ranging from 0.0% to 3.4% among patients with a final pathology of DCIS.56 Based on these results, the National Comprehensive Cancer Network (NCCN) guidelines recommend neither excessive axillary evaluations, such as axillary lymph node dissection (ALND), nor routine sentinel lymph node biopsy (SLNB) for patients undergoing breast conserving surgery (BCS) with DCIS.7
However, there is controversy regarding whether SLNB should be performed in cases of DCIS diagnosed via preoperative biopsy, because around 25% of the preoperative DCIS cases have been diagnosed as invasive breast cancer on final pathological analysis.89 Axillary evaluation is often performed because of concerns regarding the upstaging risk of DCIS.1011 If surgeons do not perform axillary staging for preoperative DCIS patients, some of them undergo additional axillary staging procedures when invasive foci are identified in the permanent pathological analysis after BCS without SLNB.
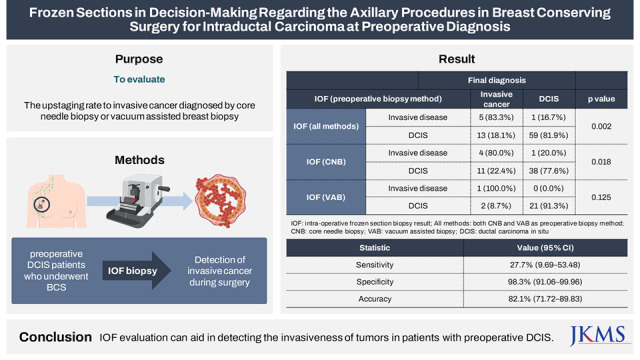
It is necessary to determine whether SLNB should be performed by assessing the upstaging status of the preoperative DCIS. The ability to predict the probability of upstaging of preoperative DCIS is beneficial for determining whether an SLNB should be performed. Several studies have reported on the prediction of the upstaging of the preoperative DCIS, such as identification of predictive factors or establishing nomograms.481213 As part of these efforts, we evaluated the role of intraoperative frozen section (IOF) biopsy of tumors in identification of the invasiveness of tumors in patients with preoperative DCIS.
Go to : 
METHODS
Patient cohort
We performed a retrospective analysis using the Breast Cancer Registry database of Yonsei University Severance Hospital. The computerized medical database was constructed in MS Access (Microsoft, Seattle, WA, USA) and contained patients’ clinical characteristics, pathologic data of preoperative or postoperative evaluations, and preoperative findings. There were 269 patients preoperatively diagnosed with DCIS from January 2013 to March 2018. Patients diagnosed with preoperative DCIS who underwent BCS and IOF were included in the study. Of these patients, 104 patients receiving total mastectomies and 87 patients who did not receive IOF were excluded from the study. The remaining 78 patients were enrolled in this study. IOF was performed at the discretion of the surgeon preoperatively. The results of the IOF biopsy were confirmed by several general pathologists supported by breast specialists using a consistent set of criteria and format. This procedure added and additional twenty to thirty minutes to the usual operative time, including resection margin frozen biopsy.
Clinicopathologic factors
The clinicopathologic factors were determined by referring to previous studies.481213 Age, lesion size, microcalcification or mass existence on imaging study, biopsy method, and nuclear grade were considered the predictive factors for invasiveness. Breast ultrasonography (USG) and mammography (MMG) were performed as preoperative evaluations for all patients. In the USG and MMG results, microcalcification, mass existence, and lesion size were reviewed. The pathology results in the medical records were reviewed to analyze the histopathological variables, including preoperative histologic findings, DCIS nuclear grade, microinvasive or suspicious invasive foci based on the IOF biopsy findings, and the final permanent pathology.
Preoperative biopsy methods
The patients received into the core needle biopsy (CNB) and vacuum-assisted biopsy (VAB) as previously described.8 A 14-gauge semi-automatic core needle was used for CNB under ultrasonic guidance.8 An 8- or 11-gauge vacuum-assisted large-core breast biopsy system was performed for VAB under ultrasonic or stereotactic guidance.8
IOF biopsy
During BCS, the main specimens sent to the pathology department were frozen, cut into 2-mm thick sections, and assessed by a pathologist. The results reported whether the lesion was DCIS, equivocal lesion, or invasive cancer. In addition to reporting invasive cancer in the IOF biopsy results, micro-invasion with DCIS or equivocal lesion such as suspicious invasion was also reported; we regarded them as invasive disease. This decision was made based on the notion that there may be a high possibility of upstaging of the permanent pathology to invasive cancer.
Axillary evaluation
SLNB was performed simultaneously in patients with invasive cancer based on the IOF biopsy findings and was performed as a secondary surgery for patients with invasive cancer based on their permanent pathology. SLNB was performed with a dual tracer technique using blue dye and technetium-99m. ALND was performed if the patients showed lymph node metastasis in SLNB.
Statistical analysis
According to the permanent pathology findings, the patients were divided into the DCIS and invasive lesion groups. Univariate analysis was performed to confirm the association of the factors in each group using Pearson’s χ2 test or Fisher’s exact test. Multivariate analyses were performed using binary logistic regression to identify the independent factors associated with the upstaging to invasive cancer.
In addition, the correlation between the IOF biopsy findings and the final pathology according to the biopsy method was analyzed.
Sensitivity, specificity, and accuracy were calculated to evaluate the diagnostic efficacy of IOF biopsy for the detection of the invasiveness of cancer. An invasive lesion detected on IOF biopsy and permanent pathology evaluations was defined to be a true positive lesion; non-invasive disease detected by permanent pathology or IOF biopsy was defined to be a true negative disease. P values < 0.05 were considered statistically significant. Statistical analyses were performed using SPSS Statistics version 23 (IBM, Chicago, IL, USA).
Ethics statement
This study was reviewed and approved by the Institutional Review Board (IRB) of Severance Hospital, Yonsei University Health System (IRB No.2020-0558-001). The study was conducted in accordance with the provisions of the Declaration of Helsinki and Good Clinical Practice guidelines. As this study is a retrospective study, written informed consent was waived by the IRB.
Go to :
RESULTS
Clinicopathological characteristics
We reviewed 78 preoperative DCIS cases with BCS and IOF. There were 60 patients (76.9%) with DCIS, and 18 patients (23.1%) with invasive cancer at the final pathology. Clinicopathologic features of the DCIS group and the invasive cancer group are compared in Table 1. Presence of microcalcification on imaging did not significantly differ in each group (MMG microcalcification: absent vs. present in invasive disease group 26.7% vs. 23.8%, P = 0.783; USG microcalcification: absent vs. present in invasive disease group 24.5% vs. 20.0%, P = 0.658).
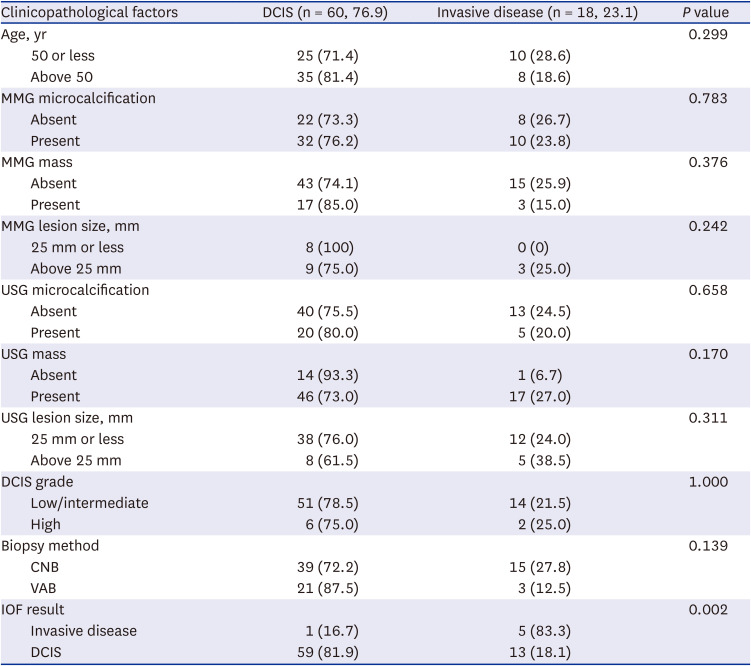
Table 1
Relationship between the clinicopathological factors and final pathology
Values are presented as number (%).
DCIS = ductal carcinoma in situ, MMG = mammography, USG = ultrasonography, IOF = intraoperative frozen section, CNB = core needle biopsy, VAB = vacuum-assisted biopsy.
![]()
Among the patients with lesions > 25 mm on MMG and USG, invasive cancer was detected in 25% and 38.5% of the patients, respectively (3/12 on MMG, 5/13 on USG). However, there were no significant differences in the tumor size > 25 mm with respect to the MMG and USG findings according to the final histologic type (MMG size: P = 0.242, USG size: P = 0.311).
Among the patients presenting with a mass on sonography, upstaging to invasive cancer was identified in 27.0% of the patients while upstaging was observed in 6.7% of the patients with absence of a mass on sonography. However, 25.9% of the patients with absence of a mass in MMG showed upstaging (15/58), while 15% (3/18) of the patients with a mass on MMG showed upstaging. However, this difference was not significant (USG mass: P = 0.170, MMG mass: P = 0.376).
DCIS grade was not correlated with upstaging to invasive cancer (P = 1.000). According to the biopsy methods, cases with CNB were upstaged to invasive cancer more frequently than those with VAB (CNB: 15/54, 27.8%, VAB: 3/24, 12.5%; P = 0.139), but it was not statistically significant in this study.
Upstage to invasive breast cancer
The final pathologic diagnoses of 18 preoperative DCIS patients were upstaged to invasive breast cancer (23.1%). Six patients were upgraded intra-operatively to invasive cancer based on the IOF biopsy findings, and SLNB was performed during the definitive surgery. Among these patients, 5 (83.3%) patients showed concordant results with the final pathology, and only 1 patient presented with pure DCIS as the final pathology. Of the 72 patients diagnosed with DCIS at IOF, 13 (18.1%) patients showed upstaging to invasive cancer (Tables 1 and 2). Upstaging to invasive cancer was significantly associated with the IOF biopsy result (P = 0.002).
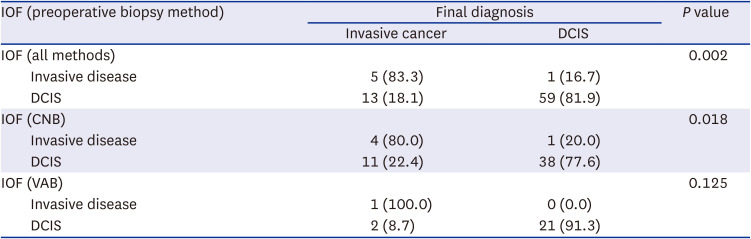
Table 2
Correlation between the IOF biopsy result and final diagnosis according to the preoperative biopsy methods
Values are presented as number (%). All methods: both CNB and VAB as preoperative biopsy method.
IOF = intraoperative frozen section biopsy result, DCIS = ductal carcinoma in situ, CNB = core needle biopsy, VAB = vacuum assisted biopsy.
![]()
There were 54 patients who received CNB and 24 patients who received VAB as the preoperative biopsy method. Considering the biopsy methods, in CNB group, 4 of 5 (80.0%) of the invasive disease of IOF were found to be invasive cancers in the final pathology (P = 0.018; Table 2).
Multivariate analysis of predictors for invasiveness
We performed multivariate analysis using IOF and the factors that were shown to be significant for upstaging to invasive cancer in previous studies.89 These factors were presence of mass and microcalcification, tumor size, and preoperative biopsy method. The presence of mass and microcalcification on USG and MMG may have high correlation and multicollinearity, which can affect the validity of multivariate analysis. Therefore, we excluded one of them from the analysis. Multivariate analyses of predictors for invasiveness are shown in Table 3. Only the IOF result was a significant independent predictor for upstaging to invasive cancer in multivariate analysis (odds ratio, 31.96; 95% confidence interval [CI], 2.38–429.14; P = 0.009). The absence of mass on MMG, and CNB as the preoperative biopsy method correlated with the tendency of upstaging to invasive cancer (MMG mass P = 0.054, biopsy method P = 0.063).
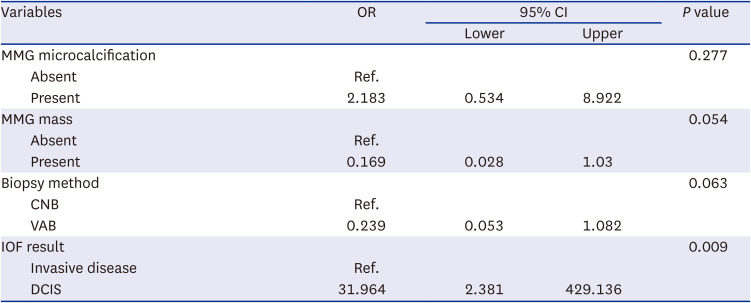
Table 3
Multivariate analysis for the factors associated with upstaging to invasive cancer
OR = odds ratio, CI = confidence interval, MMG = mammography, CNB = core needle biopsy, VAB = vacuum assisted biopsy, IOF = intraoperative frozen section.
![]()
Accuracy of IOF
IOF showed 27.7% sensitivity (95% CI, 9.69–53.48%) and 98.33% specificity (95% CI, 91.06–99.96%). The positive predictive value was 83.3% (95% CI, 38.41–97.57%). The negative predictive value was 81.9% (95% CI, 77.28–85.83%). The accuracy of IOF was 82.05% (95% CI, 71.72–89.83%; Table 4).
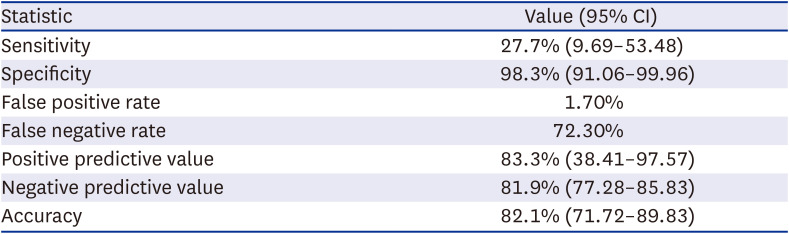
Table 4
Sensitivity, specificity, predictive value, and accuracy of IOF biopsy for upstaging
![]()
Axillary staging
In 1 out of 6 cases with invasive cancer at IOF, the SLNB showed lymph node metastasis. Axillary lymph node dissection was performed in this case. In the other group, with negative IOF results of invasiveness, 13 cases with invasive cancer in the permanent pathology underwent axillary staging as secondary surgery. None of them had a positive result.
Go to :
DISCUSSION
This study demonstrated the effectiveness of IOF for identifying invasiveness of preoperative DCIS. Positive results of IOF were significantly correlated with upstaging of preoperative DCIS (Table 1). However, other clinicopathologic factors including the tumor size in imaging, grade of DCIS, and preoperative biopsy method did not show significant correlation in the current study. These results are discordant with previous studies.49121314
Multiple clinicopathologic factors can be used to predict upstaging to invasive breast cancer from preoperative DCIS. In a meta-analysis of 7,350 patients in 52 studies reviewed by Brennan et al.,9 these factors included a palpable mass, size more than 20 mm on ultrasonography, presence of mass or Breast Imaging-Reporting and Data System (BI-RADS) category 5 on imaging, lesions diagnosed by core needle biopsy, and lesions with high nuclear grade. In our previous study, palpability in physical examination, presence of calcification or mass on ultrasonography, suspicious microinvasion in preoperative biopsy, and core needle biopsy as the biopsy method were independent predictors of an underestimation of invasive cancer.4 The presence of microinvasion had a 73% possibility of being invasive breast cancer on permanent pathology in a previous study.14 Several nomograms predicting invasiveness have been published, but no uniform pattern can be noticed overall.81213 A possible reason for no significant difference in the value of mass size in the current study is that we only analyzed patients who underwent BCS. We excluded patients who underwent total mastectomy, which is mainly performed in patients with large lesions or multicentric lesions. The small number of enrolled patients may also affect the results of the study. Nevertheless, only the IOF results showed significance predictive information of invasiveness in this study.
IOF showed low sensitivity and high specificity (Table 4), and 5 of 6 cases with a positive IOF result for invasive breast cancer were consistent with permanent pathology (Tables 1 and 2). Therefore, use of IOF can help to avoid unnecessary axillary surgery in many patients with preoperative DCIS. The use of IOF was helpful for avoiding secondary axillary surgery in about one-third of preoperative DCIS patients diagnosed with invasive cancer in permanent pathology. Our study showed lower sensitivity compared to a previous study by Murphy et al. that also evaluated the performance of IOF in DCIS cases.15 Their data from 827 patients who underwent either lumpectomy or mastectomy showed that upstaging to invasive breast cancer on permanent pathology was 14.1% (95% CI, 11.8–16.7%).15 In the lumpectomy group, intra-operative diagnosis had 80% sensitivity and 98.9% specificity with a mean DCIS size of 17.1 mm on preoperative imaging.15 The difference in sensitivity between the current and previous study may be due to the different sample size. A larger sample size and more IOF-experienced pathologists may increase the sensitivity.
In the past, the majority of patients with preoperative DCIS who underwent BCS at our institution underwent SLNB, because the possibility of upstaging to invasive cancer was over 40%.16 In this study, the upstaging rate decreased to 23%. This indicates that three-quarters of patients with preoperative DCIS could have avoided SLNB at the time of the definitive surgery if preoperative or intra-operative evaluations could accurately distinguish DCIS and invasive cancer. However, because of the uncertainty of identifying invasiveness in DCIS, axillary staging for patients with DCIS is a controversial issue. The frequency of axillary staging, including SLNB and ALND, in patients with DCIS in the USA increased from 44% to 63% since 1998.17 This suggests that unnecessary axillary procedures in patients with DCIS are still performed, and this adherence to guidelines might be partly influenced by the uncertainty in identifying invasiveness in preoperative DCIS and the wider application of SLNB. In meta-analysis by Knuttel et al.,16 one-fifth of patients with preoperative DCIS were underestimated for invasive cancer in final pathology, and they recommended routine use of SLNB in patients with DCIS. However, SLNB is not a risk-free procedure, although it has lower morbidity rates than ALND. The risk of complications such as lymphedema and postoperative pain still remains after SLNB. It is important for patients and surgeons to more accurately estimate the possibility of the upstage to invasive cancer because it can inform the decision whether SLNB should be performed. SLNB can increase patients’ complications. Therefore, the ability to predict the possibility of preoperative DCIS upstaging to invasive carcinoma and avoid unnecessary axillary procedures by IOF can reduce the necessity of SLNB at the time of definitive surgery.
Using intra-operative margin assessment in breast surgery facilitates identifying remnant breast disease and can help to decide additional treatment.1819 Applying a similar concept to examine breast lesions intra-operatively could help to avoid unnecessary axillary procedures at the definitive surgery. This may minimizes patient stress without axillary pain, operative scar and the continuous outpatient visits and dressing for drainage tube management for pure DCIS patients. Indeed, those patients with DCIS on intra-operative diagnosis had a low probability of harboring invasive breast cancer on final permanent pathology. It may be helpful to use not only IOF but also other predictive risk factors or nomograms to estimate the possibility of the upstaging.
Percutaneous biopsy techniques in DCIS cases are associated with underestimating invasive breast cancer. In our study, the rate of upstaging to invasive breast cancer on final pathology in cases with core needle biopsy was 27.8%, similar to other studies.16 A previous study reported that a larger needle or amount of tissue obtained are associated with lower rates of underestimation of preoperative DCIS.20 Using vacuum-assisted biopsy methods, the upstaging rates decreased by 31.7% in a previous study.4 Therefore, vacuum-assisted biopsy can be used for more accurate diagnosis of preoperative DCIS than core needle biopsy.
A retrospective design and the small number of cases in a single institution are the major limitations of this study. However, to our knowledge, few large-scale studies have used IOF of the main tumor specimen to assess tumor invasiveness. As such, our findings can support the potential utility of IOF in predicting the upstaging of DCIS. Furthermore, the consistency of data from a single institution is also one of the strengths of the study. The results of the biopsy and radiological interpretation were verified with unified criteria and formats. The pathological and imaging interpretation method may vary depending on the institution. Therefore, different institutions may show different results in IOF interpretation. IOF is sometimes difficult and confusing for pathologists; therefore, well-skilled and experienced pathologists are needed to perform IOF accurately. However, experienced pathologists are not always available due to institutional limitations. Machine learning for the interpretation of IOF can help to reduce inter-observer discrepancies among pathologists.
Several trials on de-escalation or omission of axillary surgery, and active surveillance without any surgery, are ongoing in early breast cancer.21222324 As the studies progress, the status quo in the wide use of axillary surgery for patients with DCIS may change. As part of this, efforts are needed to determine the appropriate extent of surgery necessary for patients to reduce the occurrence of complications. In this regard, this study introduced the role of IOF in reducing axillary surgery in preoperative DCIS.
The use of IOF during BCS showed high specificity and accuracy for detecting invasiveness in cases with preoperative DCIS. However, low sensitivity is a limitation of IOF. Further prospective study is needed to validate the role of IOF during BCS for patients with preoperative DCIS.
In conclusion, IOF can be a potential adjunctive diagnostic tool for identifying invasiveness in patients with preoperative DCIS. This approach may help to reduce the stress of patients by avoiding unnecessary axillary surgery for pure DCIS patients in selected cases.
Go to :
 XML Download
XML Download