

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) continues to become a global pandemic, with the omicron variant out-competing former variants.1 Following the onset of COVID-19 in children and adolescents, some of patients may present hyperinflammatory shock with multisystem involvement.234 These acute sequelae of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection are known as multi-system inflammatory syndrome in children (MIS-C).567 Common symptoms of MIS-C include high fever, rash, conjunctivitis, peripheral edema, and gastrointestinal symptoms.8
Previous observational studies revealed the difference in the incidence of MIS-C in patients with different variants of SARS-CoV-2.91011 In particular, MIS-C was less common in omicron than in delta, while symptoms were less severe in omicron than during the alpha or delta waves. However, little is known about the epidemiology of MIS-C cases in Asian countries, where the incidence of Kawasaki disease, a similar febrile syndrome with MIS-C, is the highest in the world.12 Furthermore, given the larger number of COVID-19 cases during omicron, the potential for increased number of children to experience MIS-C is a major concern.13
In this study, we aimed to investigate and compare the prevalence of the MIS-C during omicron-dominant period with that of previous periods in South Korea.
Go to : 
METHODS
Per Infectious Diseases Control and Prevention Act, the surveillance case definition and reporting threshold did not change over time of observation.14 COVID-19 vaccination started in adolescents since October 2021, reaching vaccine coverage of 67.8% for one dose and 46.3% for two doses, by the end of 2021.15 COVID-19 vaccination in children aged 5–11 started since March 2022, with low coverage of 1% by August 2022.16
We obtained clinical, epidemiological and laboratory data on MIS-C cases from ongoing national MIS-C surveillance scheme in South Korea. The surveillance was sponsored by Korea Disease Control and Prevention Agency, in collaboration with the Korean Society of Pediatrics, Korean Society of Pediatric Infectious Diseases, Korean Society of Pediatric Critical Medicine, and Korean Society of Kawasaki Disease, as described previously (Fig. 1).17 Briefly, the case definition for MIS-C included patients < 21 years of age hospitalized with fever, involvement of at least 2 organ systems, laboratory evidence of inflammation, laboratory confirmation of SARS-CoV-2 infection or recent exposure to a suspected or confirmed COVID-19 case and no alternative plausible diagnosis. All suspected MIS-C cases were reported to the surveillance scheme, which the prompts 1) epidemiological investigation, 2) laboratory surveillance, and 3) clinical ascertainment by the primary team (Fig. 1). Korea Disease Control and Prevention Agency performed serologic assays for SARS-CoV-2 original Wuhan strain, including plaque reduction neutralization test (PRNT) and the Anti-SARS-CoV-2 enzyme-linked immunosorbent assay (ELISA) for detection of IgG against S1 protein (EUROIMMUN), as described previously.17 Then the Case Assessment Committee (CAC) members were convened for individual case-based assessment. The CAC consist of four pediatric infectious disease specialists, three pediatric cardiologists, three pediatric intensivists, one clinical microbiologist, and one epidemiologist. Between June 2020 to May 2022, a total of 18 CAC meetings were held.

We calculated the reported number and incidence rate of MIS-C among Korean children aged 0–19 years following SARS-CoV-2 infection by dominant variant strain. Based on the national viral genomic surveillance data, we defined pre-delta period as January 2020–May 2021; delta period as June 2021–December 2021; and omicron period as January 2022–April 2022. We then describe the characteristics of MIS-C patients my dominant variant strains, including clinical variables (presence of hypotension, gastrointestinal, dermatologic, neurologic, or respiratory involvement, per medical record), laboratory values (PRNT, ELISA), and outcomes (use of inotropic, intensive care unit admission, and length of hospital stay). Lastly, we describe the treatment pattern (use of intravenous immunoglobulin [IVIG] and/or steroids, infliximab) and final health outcome (survival, disability, death, per medical record) after minimum of 6 months of follow-up.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital and the requirement for informed consent was waived (IRB 2012-136-1183).
Go to :
RESULTS
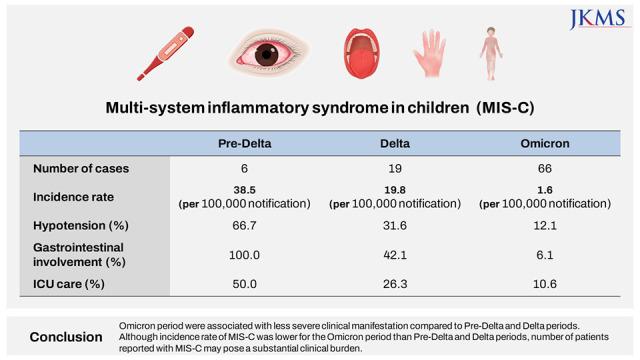
Between April 2020 and April 2022, a total of 124 suspected MIS-C cases were reported from 48 different institutions across the country; and 91 cases were assessed to be MIS-C cases (Fig. 2). The reasons for exclusion were: 1) no epidemiologic or laboratory evidence of prior SARS-CoV-2 infection or exposures; 2) other etiologies (Mycoplasma pneumoniae, parainfluenza virus) that explains the patient's symptoms; or 3) not meeting predefined clinical case definition of MIS-C. Number of MIS-C cases have increased from six cases during pre-delta period to 19 cases during delta, and 66 cases during omicron periods (Fig. 3 and Table 1). However, incidence rate (the number of MIS-C cases per 100,000 cases of reported COVID-19) has decreased from 38.5 cases per 100,000 (95% confidence interval [CI], 14.1–83.9) during pre-delta period to 19.8 cases per 100,000 (95% CI, 11.9–30.9) during delta and 1.6 cases per 100,000 (95% CI, 1.2–2.0) during omicron periods (Table 1).


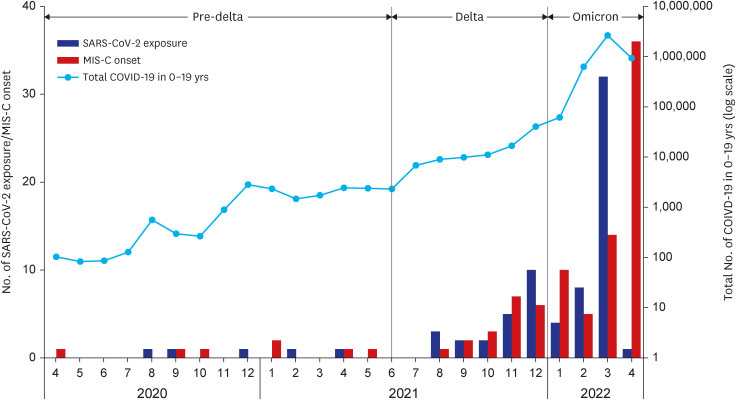 | Fig. 3Temporal trend of monthly putative SARS-CoV-2 exposures in MIS-C cases and their MIS-C occurrence (left axis), and total number of COVID-19 cases in 0–19 years (right axis, in log-scale).SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, MIS-C = multi-system inflammatory syndrome in children, COVID-19 = coronavirus disease 2019.
|
Table 1
Incidence of MIS-C among Korean children aged 0–19 years following SARS-CoV-2 infection by dominant variant strain
| Perioda | MIS-C cases | COVID-19 casesb | Incidence ratec | 95% CI |
|---|---|---|---|---|
| Pre-delta | 6 | 15,565 | 38.50% | 14.1–83.9 |
| Delta | 19 | 96,002 | 19.80% | 11.9–30.9 |
| Omicron | 66 | 4,251,386 | 1.60% | 1.2–2.0 |
MIS-C = multi-system inflammatory syndrome in children, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, COVID-19 = coronavirus disease 2019, CI = confidence interval.
aPre-delta, Jan 2020–May 2021; delta, Jun 2021–Dec 2021; omicron, Jan 2022–Apr 2022; bCOVID-19 cases in children aged 0–19 years; cper 100,000 notification.
![]()
Table 2 shows the demographic characteristics of MIS-C patients by dominant variant strains. Median age during pre-delta and delta periods were 10 years (interquartile range [IQR], 7–14 years) and 7 years (IQR, 3–10), respectively; while the median age during omicron period was 6 years (IQR, 5–11). During pre-delta period, 66.7% and 100% had hypotension and gastrointestinal involvement, respectively; while during omicron period, 12.1% and 6.1% had such clinical manifestations (Table 3). 50% of pre-delta MIS-C patients were taken intensive care unit (ICU) cares, while 26.3% and 10.6% of patients during delta and omicron periods were in ICUs. Median length of hospital stays were 10 days during pre-delta and delta periods; while during omicron period, it was 6 days (IQR, 5–9).
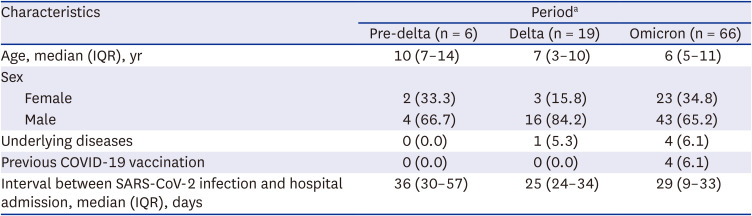
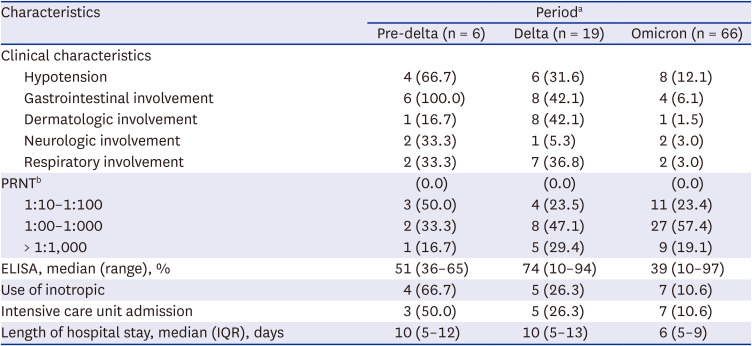
Table 2
Demographic characteristics of MIS-C patients by dominant variant strain
Values are presented as number (%) unless otherwise indicated.
MIS-C = multi-system inflammatory syndrome in children, IQR = interquartile range, COVID-19 = coronavirus disease 2019, SARS-CoV-2 = severe acute respiratory disease coronavirus 2.
aPre-delta, Jan 2020–May 2021; delta, Jun 2021–Dec 2021; omicron, Jan 2022–Apr 2022.
![]()
Table 3
Clinical characteristics of MIS-C patients by dominant variant strain
MIS-C = multi-system inflammatory syndrome in children, PRNT = plaque reduction neutralization test, ELISA = enzyme-linked immunosorbent assay (cut-off value, OD > 1.1), IQR = interquartile range.
aPre-delta, Jan 2020–May 2021; delta, Jun 2021–Dec 2021; omicron, Jan 2022–Apr 2022; bPRNT data available for 6 pre-delta, 17 delta, and 47 omicron cases.
![]()
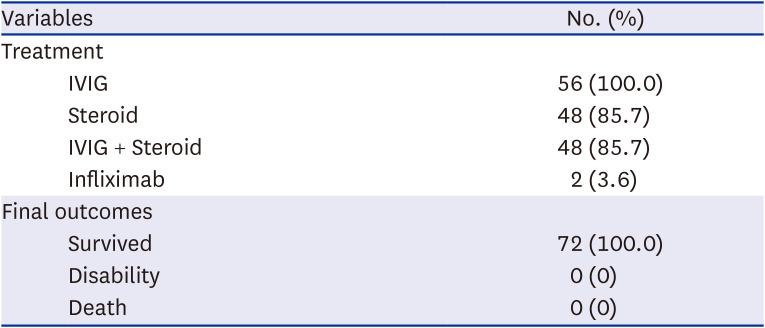
Table 4 shows the treatment regimen and final outcome of 91 MIS-C cases. Nearly all cases except two have received IVIG and 84.6% have received steroids. Only once case was treated with anakinra. All of 91 MIS-C cases were survived with no reported cases with disability after minimum of 6 months of follow-up.
Go to :
DISCUSSION
The predominant circulating SARS-CoV-2 variant in South Korea was changed to delta in June 2021 and then to omicron in January 2022.18 Understanding the clinical difference of MIS-C with each variant is essential for guiding clinical decision making and resource allocation. In this study, we investigated and compared the incidence of MIS-C in children during omicron-dominant period and pre-delta/delta-dominant periods. The main finding of this study was that the incidence of MIS-C during omicron period was lower, while the severity tended to be less severe than that of previous strain-dominant periods. However, more children were infected with omicron in South Korea, thus while the incidence rate may be lower during omicron period, the actual number of patients suffering from MIS-C was higher than during pre-delta or delta periods.
From this national representative surveillance in South Korea, we found that the MIS-C incidence rate ranged 1.6 (omicron) and 38.5 (pre-delta) per 100,000 per SARS-CoV-2 infected children, which was lower than incidence reported in Australia (130 per 100,000 during pre-delta, 50 per 100,000 during delta, and 8 per 100,000 during omicron), although the decreasing trend was identical.19 In the U.K., Cohen et al.,9 reported the incidence of MIS-C to be 231 per 100,000 during alpha variant period and 12 per 100,000 during omicron period. This is also consistent with an observational study in Israel that the incidence decreased from 54.5 per 100,000 during Alpha wave to 3.8 per 100,000 during omicron wave.11 Similar to our study, in the U.S., proportions in patients 0–4 years-of-age rose from 46% to 62% during delta and omicron, respectively, although the trend may have influenced by vaccination in older age group.20 Although we did not directly compare the incidence and severity of MIS-C with those of previous studies, characterizing the clinical course of MIS-C in different countries may assist in understanding the potential impact of future variants of concern.
Consistent with the severity of MIS-C, median titer of ELISA was lower during omicron period compared to pre-delta and delta periods. Multiple previous studies suggested correlation between antibody level and disease severity.212223 Further investigating the trends of antibody titers may provide biologic insight to the MIS-C or may serve as potential predictors of MIS-C outcomes.
Despite the difference in clinical manifestation between the variant-strain dominant periods, we also found that all MIS-C patients have survived with no clinical disability reported, despite the variability in treatment regimen (85.7% have received steroid treatment). This finding is consistent with previous report stating that the clinical course was less severe and outcome was generally better in Asian population compared to other geographical regions.24 In an U.S. study, MIS-C was less frequent among non-Hispanic White and Asian children.25 These findings can also help raise awareness on what manifestations are more common with the different variant to aide in rapid clinical decision making.
Our study had several limitations. Firstly, we used data obtained from passive surveillance, which may have influenced the results. Those with mild MIS-C might be less likely to be reported if the healthcare providers were unaware, making data on the MIS-C during omicron period more likely to be underreported. Secondly, we did not have individual-level variant sequencing data available, which may have resulted in misclassification in individual MIS-C cases. Thirdly, geographic distribution of reported cases represents metropolitan area-dominant children, therefore, our results may not be generalizable to the whole country. Uneven distribution of pediatric specialties, including infectious diseases, cardiology, and intensive care, across the nation may have influenced the different likelihood of reporting a suspected MIS-C case.
Despite these limitations, our data indicate that the omicron variant is associated with less severe MIS-C in Korean children, however, the number of cases can increase due to increased number of SARS-CoV-2 infection. COVID-19 vaccination is an effective preventive measure against the SARS-CoV-2 infection and the occurrence of MIS-C. These findings support recommendations in for mRNA vaccines for both immunocompetent and immunocompromised children as a key approach to protecting the omicron variant.26
In this national surveillance of MIS-C in South Korea, omicron period were associated with less severe clinical manifestation compared to pre-delta and delta periods. Although the number of patients reported with MIS-C has increased, the risk and severity of individual cases has decreased, which highlights the public health need to revisit the treatment strategy of MIS-C patients.
Go to :
 XML Download
XML Download