

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hepatitis B virus (HBV) reactivation is a major complication in patients who have a history of HBV infection and receive immunosuppressive therapy or chemotherapy. HBV reactivation has a variety of clinical manifestations from asymptomatic to life-threatening liver failure caused by fulminant hepatitis.1 Patients with chronic hepatitis B (CHB) who receive immunosuppressive therapy or chemotherapy are at risk for HBV reactivation.2 Patients with resolved HBV, which is characterized by negative hepatitis B surface antigen (HBsAg) and positive immunoglobulin G subclass of antibody to hepatitis B core antigen (anti-HBc) on blood tests, may have a low level of HBV genome in their hepatocytes.34 Therefore, patients with resolved HBV may also experience HBV reactivation if their immune function decreases due to immunosuppressive therapy or chemotherapy.567
Since the activity of HBV is determined by an interaction between viral replication and the host immune response, the possibility of HBV reactivation varies depending on the type of immunosuppressive therapy or chemotherapy.8 Among patients using immunosuppressive therapy or chemotherapy, the risk of HBV reactivation is high in those on B lymphocyte-depleting agents such as rituximab.91011 Rituximab is a monoclonal antibody against cluster of differentiation 20 (CD20) on the surface of the B lymphocytes. B lymphocyte count decreases by 90% within 3 days of rituximab administration and recovers after 6 to 12 months.12 Rituximab is the basis of combination chemotherapy in the treatment of non-Hodgkin lymphoma.13 A recent meta-analysis showed that non-Hodgkin lymphoma patients treated with rituximab had a higher risk of HBV reactivation than those treated with anticancer drugs other than rituximab.14 Previous studies have suggested that HBsAg-positive patients (i.e., patients with CHB) should receive prophylactic antiviral therapy to reduce the risk of HBV reactivation when being treated with rituximab.15161718192021 Patients who have achieved seroclearance of HBsAg (HBsAg-negative) are less likely to develop HBV reactivation than HBsAg-positive patients; for HBsAg-negative and anti-HBc-positive patients (i.e., patients with resolved HBV), some guidelines recommend prophylactic antiviral therapy for 6 months or 12 months, while some guidelines recommend close monitoring rather than prophylactic antiviral therapy.22232425 Prolonged antiviral therapy leads to a variety of side effects and a decrease in adherence, consequently lowering its benefits compared to its risks.262728 However, there has been insufficient evidence for the optimal duration of prophylactic antiviral treatment when rituximab is administrated in HBsAg-negative and anti-HBc-positive patients.
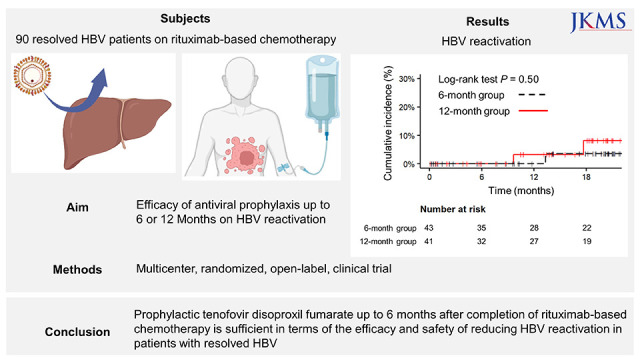
We aimed to compare the efficacy and safety of tenofovir disoproxil fumarate (TDF) in preventing HBV reactivation between 6-month and 12-month duration of prophylactic treatment in HBsAg-negative and anti-HBc-positive non-Hodgkin’s lymphoma patients treated with rituximab-based chemotherapy.
METHODS
Study design
This study was designed as a multicenter, randomized, open-label, prospective study. Participants in the study were randomized at a 1:1 ratio and assigned to the 6-month group or the 12-month group by the Medical Research Collaborating Center (MRCC) at Seoul National University Hospital, a center independent from researchers. For the generation of randomization codes and the operation of randomization procedures, Interactive Web Response System was used, which was operated by MRCC.
Patients and interventions
Patients aged 18 to 80 years who were diagnosed with CD20 positive non-Hodgkin's lymphoma and who received rituximab-based chemotherapy were enrolled in this study. Participants had Eastern Cooperative Oncology Group performance status between 0 and 2, were HBsAg-negative, anti-HBc-positive, and anti-hepatitis C virus antibody (anti-HCV) negative, and had a serum creatinine level of < 2 mg/dL, hemoglobin ≥ 9 g/dL, absolute neutrophil counts ≥ 1,500 /μL, platelet counts ≥ 75,000 /μL (unless abnormalities were due to bone marrow involvement by lymphoma), a serum alanine aminotransferase (ALT) level of < 80 IU/mL, and a serum total bilirubin level of < 3.0 mg/dL (unless abnormalities were due to liver involvement by lymphoma or tumor lysis syndrome). Patients with Child-Pugh class C, autoimmune hepatitis, Wilson’s disease, other chronic liver diseases, galactose intolerance, Lapp lactase deficiency, glucose-galactose malabsorption, pregnancy, lactation, or hypersensitivity to TDF were excluded.
The 6-month group received oral TDF 300 mg (Gilead, Foster City, CA, USA) daily during the period of rituximab treatment and for an additional 6 months after the completion of rituximab treatment. The 12-month group received oral TDF 300 mg daily during the period of rituximab treatment and for an additional 12 months after the completion of rituximab treatment.
During the planning of the study, there was limited evidence concerning the efficacy of prophylactic TDF in patients with resolved HBV infection and treated with rituximab. A clinical trial reported that rituximab has an immunosuppressive effect that lasts for up to six months after treatment, at which point the immune system slowly recovers over the next three to six months.29 One study found that resolved HBV patients treated with rituximab had a risk of HBV reactivation of about 23% in the first 6 months and up to 19% thereafter.10 Another study reported that resolved HBV patients treated with rituximab did not experience HBV reactivation while maintaining prophylactic TDF.30 Based on the previous studies, we assumed that the HBV reactivation rate in the 6-month group is 9%, approximately half of 19%, because the group is at risk of HBV reactivation since prophylactic TDF is discontinued during the period when immune function is slowly regaining but not yet fully recovered. On the other hand, we hypothesized that the HBV reactivation rate in the 12-month group is 0.01% since prophylactic TDF is used adequately during the period of rituximab-induced immunosuppression. To test the null hypothesis by power of 80% and type I error of 0.05 on both sides, assuming that the reactivation rate of HBV is 9% for the 6-month group and 0.01% for the 12-month group, each group required 41 participants.3132 In consideration of the 10% dropout rate, a total of 90 participants were needed.
Assessments and outcomes
Blood tests including ALT, albumin, total bilirubin, creatinine, platelet, HBsAg, anti-hepatitis B surface antibody (anti-HBs), hepatitis B e antigen (HBeAg), anti-HCV, anti-human immunodeficiency virus antigen (anti-HIV), and quantitative HBV DNA were performed at the screening visit. Liver function tests and HBV DNA tests were performed 4 times during chemotherapy: the first day of chemotherapy, 4 and 12 weeks from the start of chemotherapy, and the last day of chemotherapy. After the completion of rituximab-based chemotherapy, liver function tests and HBV DNA tests were performed 6 times: every 12 weeks up to 72 weeks from the end of chemotherapy. HBsAg and anti-HBs were tested every 24 weeks after the discontinuation of TDF. If hepatitis flare occurred, liver function tests were performed every week regardless of the chemotherapy schedule.
The primary outcome was the development of HBV reactivation. HBV reactivation was defined as HBV DNA rising by more than 2,000 IU/mL compared to baseline and/or HBsAg seroreversion to HBsAg positive during the period of participation in this study.2333 The secondary outcomes were the development of hepatitis flare and adverse events. Hepatitis flare was defined as ALT of ≥ 100 IU/L with HBV reactivation.
The outcomes were analyzed by modified intention to treat (ITT) and per protocol (PP) approaches. The ITT population was composed of patients who received at least one dose of rituximab and TDF. The PP population was composed of patients who completed 72 weeks of follow-up after the completion of chemotherapy with rituximab.
Statistical analyses
Continuous data were described as median with interquartile range. Categorical data were described as the frequency with percentage. Student’s t-test or Mann-Whitney U test was performed on continuous variables. The χ2 test or Fisher’s exact test was performed on categorical variables. The cumulative incidence of HBV DNA reactivation and hepatitis flare were compared between the 6- and 12-month groups using the Kaplan-Meier model and log-rank test. The rates of HBV reactivation and 95% confidence intervals (CI) were calculated in the 6-month group and 12-month group. In addition, it was also examined whether the groups differed in terms of the HBV reactivation rates and 95% CIs.34 The odds ratio and 95% CI were calculated for the 12-month group compared to the 6-month group. The primary outcome was further analyzed using the missing equals failure method.35
All statistical analyses were done by a two-sided test. A P value lower than 0.05 was considered statistically significant. R version 3.6.3 (http://www.r-project.org/; R Foundation, Vienna, Austria) was used for all statistical analyses.
Ethics statement
This study was approved by the Institutional Review Boards of Seoul National Hospital (H-1506-020-678) and Konkuk University Medical Center (KUH1010712). The study was conducted in compliance with the ethical principles in the Declaration of Helsinki (revised in 2013) and registered at ClinicalTrials.gov (NCT02585947). All participants provided written informed consent prior to enrolling in the study.
RESULTS
Baseline characteristics
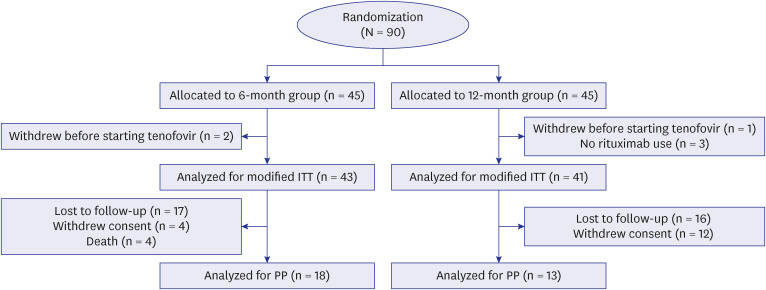
A total of 90 non-Hodgkin lymphoma patients from November 2015 to October 2017 were enrolled and randomized. After randomization, three patients decided to receive chemotherapy without rituximab, and three other patients withdrew consent before starting prophylactic TDF treatment. Consequently, 43 patients were assigned to the 6-month group and 41 patients were assigned to the 12-month group for ITT analysis (Fig. 1). During the study period, 33 patients were lost to follow-up, 16 patients withdrew consent, and 4 patients died. Finally, PP analysis was performed with 18 patients in the 6-month group and 13 patients in the 12-month group (Fig. 1).
Fig. 1
Consolidated Standards of Reporting Trials diagram.
ITT = intention to treat, PP = per protocol.
HBV DNA was undetectable, HBeAg was negative, and anti-HIV was negative at baseline in all patients included in the ITT or PP analysis. There were no significant differences in age, sex, anti-HBs positivity, anti-HBs titer, ALT, albumin, total bilirubin, creatinine, platelet count, fibrosis-4 score at baseline, type of lymphoma, cycles of chemotherapy, cumulative dose of rituximab, and regimen of chemotherapy between the 6-month group and the 12-month group in ITT analysis (all P > 0.05; Table 1). There was no significant difference in all baseline characteristics except age (median 62.5 years in the 6-month group, median 57.0 months in the 12-month group; P = 0.021; all other P > 0.05; Supplementary Table 1) in PP analysis.
Table 1
Baseline characteristics in the population for intention to treat analysis
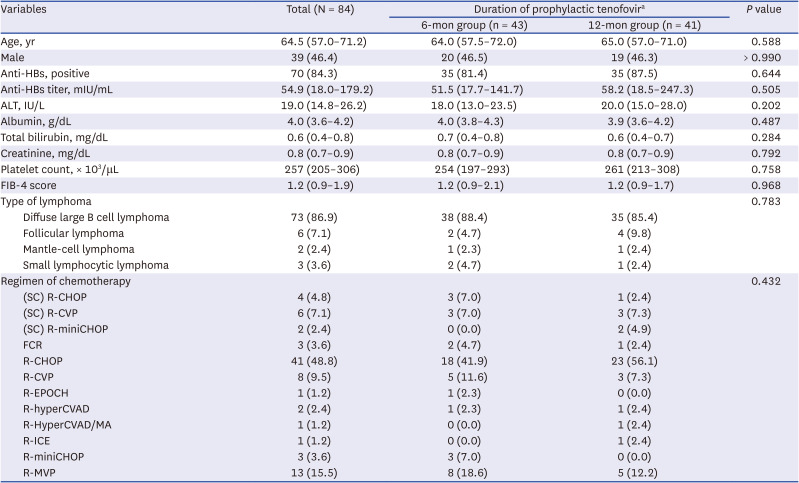
Data are expressed as number (%) or median with interquartile range.
Anti-HBs = anti-hepatitis B surface antibody, ALT = alanine transaminase, FIB-4 = fibrosis-4, SC = subcutaneous, R-CHOP = rituximab with cyclophosphamide, doxorubicin, vincristine, and prednisone, R-CVP = rituximab with cyclophosphamide, vincristine and prednisolone, R-miniCHOP = rituximab and reduced dose cyclophosphamide, doxorubicin, vincristine, and prednisone, FCR = fludarabine, cyclophosphamide and rituximab, R-EPOCH = rituximab, etoposide phosphate, prednisone, vincristine sulfate, cyclophosphamide and doxorubicin hydrochloride, R-hyperCVAD = rituximab plus fractionated cyclophosphamide, vincristine, doxorubicin and dexamethasone, R-hyperCVAD/MA = rituximab plus fractionated cyclophosphamide, vincristine sulfate, doxorubicin and dexamethasone alternating with high-dose methotrexate and cytarabine, R-ICE = rituximab, ifosfamide, carboplatin and etoposide, R-MVP = rituximab, methotrexate, vincristine, procarbazine.
aReceived prophylactic tenofovir disoproxil fumarate 300 mg daily from the start of rituximab for 6 months (6-month group) or 12 months (12-month group) after completion of rituximab.
Primary outcome
In ITT analysis, HBV reactivation occurred in 1 of 43 patients (2.3%; 95% CI, 0.41–12%) in the 6-month group and 2 of 41 patients (4.9%; 95% CI, 1.4–16%) in the 12-month group during the study period (P = 0.966; Table 2). The difference in HBV reactivation rate between the groups was 2.6% (95% CI, −5.4–11%). The time from the initial administration of rituximab to HBV reactivation was 13.3 months in the 6-month group and a median of 13.7 months in the 12-month group (P > 0.999; Table 2). There was no significant difference in the cumulative incidence of HBV reactivation between the two groups (log-rank test P = 0.502; Fig. 2A). HBsAg seroreversion occurred at 17.6 months of enrollment in 1 patient in the 12-month group who self-discontinued prophylactic TDF and changed to entecavir 1 month after starting the drug. Elevations of HBV DNA levels above 2,000 IU/mL were observed at 9.7 months from enrollment in 1 patient in the 12-month group who missed 9 days of prophylactic TDF administration and at 13.3 months from enrollment in 1 patient in the 6-month group who completed prophylactic TDF administration. In both patients described above, AST and ALT levels were normal, and HBV DNA was not detected at the next visit. Compared to the 6-month group, the 12-month group had an odds ratio of 2.0 and a 95% CI of 0.16 to 65 in HBV reactivation. Additionally, there was no difference in HBV reactivation between the 6-month group and the 12-month group in ITT using the missing equals failure method. (P = 0.692; Supplementary Table 2).
Table 2
HBV reactivation according to the duration of prophylactic tenofovir administration after rituximab-based chemotherapy
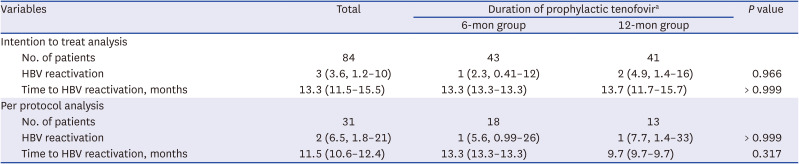
Data with parentheses are expressed as number (%, 95% confidence interval) or median (interquartile range). HBV reactivation was defined as HBV DNA rising by more than 2,000 IU/mL compared to baseline and/or HBsAg seroreversion to HBsAg positive during the period of participation in this study.
HBV = hepatitis B virus, HBsAg = hepatitis B surface antigen.
aReceived prophylactic tenofovir disoproxil fumarate 300 mg daily from the start of rituximab up to 6 months (6-month group) or 12 months (12-month group) after completion of rituximab.
Fig. 2
Cumulative incidence of hepatitis B virus reactivation according to the duration of prophylactic tenofovir administration after rituximab-based chemotherapy in (A) intention to treat analysis and (B) per protocol analysis.
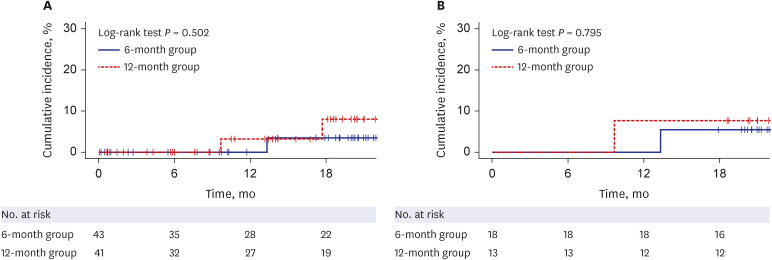
In PP analysis, HBV reactivation occurred in 1 of 18 patients (5.6%; 95% CI, 0.99–26%) in the 6-month group and 1 of 13 patients (7.7%; 95% CI, 1.4–33%) in the 12-month group during the follow-up (P > 0.999; Table 2). The difference in HBV reactivation rate between the groups was 2.1% (95% CI, −16–20%). The time from the initial administration of rituximab to HBV reactivation was 13.3 months in the 6-month group and 9.7 months in the 12-month group (P = 0.317; Table 2). There was no significant difference in the cumulative incidence of HBV reactivation between the two groups (log-rank test P = 0.795; Fig. 2B). The 12-month group had an odds ratio of 1.4 and a 95% CI of 0.03 to 58 in terms of HBV reactivation compared to the 6-month group.
Secondary outcomes
Neither the ITT analysis nor the PP analysis group experienced hepatitis flare during the participation period.
In ITT analysis, the frequency of adverse events was not significantly different between the two groups (4 of 43, 9.3% in the 6-month group; 9 of 41, 22.0% in the 12-month group; P = 0.193; Supplementary Table 3). There were no significant differences in severity and type of adverse events between the two groups (all P > 0.05; Supplementary Table 3).
In PP analysis, the number of adverse events was not significantly different between the two groups (1 of 18, 5.6% in the 6-month group; 1 of 13, 7.7% in the 12-month group; P > 0.999; Supplementary Table 4). There were no significant differences in severity and type of adverse events between the two groups (all P > 0.05; Supplementary Table 4).
DISCUSSION
This study was designed as a multicenter, randomized, open-label, prospective study to investigate the optimal duration of TDF to prevent HBV reactivation in patients with HBsAg-negative and anti-HBc-positive non-Hodgkin’s lymphoma using rituximab-based chemotherapy. Based on the report that 6 to 12 months is needed for the recovery of B cell function after administration of rituximab and the guidelines that recommend 6 or 12 months of prophylactic antiviral therapy in patients with resolved or occult HBV undergoing chemotherapy,1223 we compared 6 months to 12 months of prophylactic antiviral therapy to determine the optimal treatment duration. The 6-month group and the 12-month group received TDF during the same period as the rituximab treatment, but the durations of additional prophylactic TDF after completion of rituximab treatment were 6 and 12 months, respectively. This study found no significant difference in HBV reactivation and adverse events between the 6-month group and the 12-month group.
HBV reactivation has been variously defined, such as elevation of HBV DNA or reappearance of HBV DNA, HBsAg, HBeAg, or anti-HBc IgM in previous studies.910333637 In a randomized controlled trial evaluating the efficacy of prophylactic entecavir in patients with resolved HBV and lymphoma using rituximab, Huang et al.33 defined HBV reactivation as when the HBV viral load is increased by 2,000 IU/mL for two consecutive times. In a randomized prospective investigation evaluating the efficacy of prophylactic TDF in anti-HBc-positive hematologic malignancy patients using rituximab-based chemotherapy, Buti et al.38 defined HBV reactivation as HBsAg detection, HBV DNA detection, or HBV DNA level increased by 1 log10 IU/mL or more compared to baseline. The definition of HBV reactivation in a recent guideline of the American Association for the Study of Liver Diseases (AASLD) is loss of immune control against HBV when receiving immunosuppressive treatment in anti-HBc-positive and HBsAg-positive or -negative patients, which means either the HBV DNA level rises above the basal level or seroreversion of HBsAg (transition from negative to positive).23 We defined HBV reactivation as an increase in HBV DNA levels of more than 2,000 IU/mL and/or HBsAg seroreversion compared to baseline, which was in line with the definitions in the literature.2333
Various strategies to prevent HBV reactivation have been proposed in HBsAg-negative and anti-HBc-positive patients receiving rituximab. AASLD recommends that HBsAg-negative and anti-HBc-positive patients undergo anti-HBV prophylaxis during immunosuppression treatment and for up to 12 months after completion of immunosuppression when receiving anti-CD20 antibodies such as rituximab.23 The European Association for the Study of the Liver recommends that HBsAg-negative and anti-HBc-positive patients receiving rituximab undergo HBV prophylaxis for at least 18 months after discontinuation of rituximab.22 The Asian Pacific Association for the Study of the Liver noted that while HBsAg-negative and anti-HBc-positive patients receiving rituximab are at risk for HBV reactivation, further study is needed on the comparison of prophylactic antiviral agents and HBV DNA monitoring.24 Some reports in HBsAg-negative and anti-HBc-positive lymphoma patients receiving rituximab showed that the strategy of close monitoring without prophylactic antiviral agents and on-demand antiviral administration was also successful.103339
At least 3 months of prophylactic antiviral treatment after completion of rituximab is required to reduce HBV reactivation in resolved HBV patients receiving rituximab.333840 Huang et al.33 reported that HBV reactivation was significantly lower in the group treated with prophylactic entecavir for up to 3 months from completion of the chemotherapy compared to the control group in CD20+ lymphoma patients with resolved HBV. In addition, the effect was maintained up to 18 months; the cumulative HBV reactivation rates were 4.3% in the prophylactic entecavir group and 25.9% in the control group at 18 months from completion of chemotherapy. Buti et al.38 reported that HBV reactivation at 18 months was 0% (0 out of 33 patients) when prophylactic TDF was administered for 18 months from the start of chemotherapy in resolved HBV patients with hematologic cancer treated with rituximab, whereas HBV reactivation at 18 months in the close monitoring group was 10.7% (3 out of 28 patients). Another study by Kusumoto et al.40 in HBsAg-negative and anti-HBc-positive non-Hodgkin B-cell lymphoma patients receiving rituximab or obinutuzumab showed that the HBV reactivation rate was 10.8% (25 out of 232 patients) without prophylactic antiviral drugs and 2.1% (2 out of 94 patients) with prophylactic antiviral drugs, all of which were prophylactic lamivudine, while patients on prophylactic entecavir or tenofovir did not develop HBV reactivation.
Antiviral drugs with a high genetic barrier may effectively prevent HBV reactivation for a period shorter than 12 months in resolved HBV patients receiving rituximab. Entecavir, an antiviral drug with a high genetic barrier, for only 3 months of prophylaxis maintained the effect of preventing HBV reactivation for up to 18 months in resolved HBV patients treated with rituximab.33 TDF, another antiviral drug with a high genetic barrier, did not differ in the effectiveness and safety of preventing HBV reactivation between the 6-month group and the 12-month group in our study. Furthermore, none of the patients with resolved HBV using rituximab developed HBV-related hepatitis, even though they used prophylactic TDF for up to 6 months after completion of chemotherapy in our study. Since prolonged prophylactic antiviral treatment may result in decreased adherence and increased side effects (e.g., decrease in renal function and bone mineral density) and costs, evaluation of the appropriate administration period is crucial.26272841 Our results suggested that prophylactic TDF up to 6 months after completion of chemotherapy is adequately effective in reducing HBV reactivation in resolved HBV patients using rituximab.
Recently, novel biomarkers have been proposed for hepatitis B patients, and some of these biomarkers, such as Hepatitis B core-related antigen(HBcrAg), may be useful in evaluating the prognosis of resolved HBV patients. When HBV infects hepatocytes, the HBV genome forms covalently closed circular DNA (cccDNA) from relaxed circular DNA or integrates into the genome of the host hepatocyte.4243 Even though HBsAg clearance is achieved by the host’s immune response, some of the HBV genomes that have formed cccDNA or integrated into the host genome may remain.34 There are some reports that HBV DNA remains in the host's liver for years to decades and leads to HBV reactivation if the host’s immune system is compromised in serologically resolved HBV patients.32244 The level of HBcrAg is related to the level of intrahepatic cccDNA. Therefore, in resolved HBV patients for whom HBV DNA cannot be measured in serum, the level of HBcrAg may indicate the burden of HBV.45 Furthermore, high levels of HBcrAg have been associated with a greater risk of hepatocellular carcinoma.46 A recent study investigated the risk of hepatocellular carcinoma by assessing where HBV DNA is integrated into the host genome.47
To our best knowledge, this is the first multicenter, randomized, open-label, prospective clinical trial to investigate the difference in HBV reactivation according to the duration of prophylactic TDF in HBsAg-negative and anti-HBc-positive patients using rituximab-based chemotherapy. Previous studies in resolved HBV patients using rituximab investigated the difference in HBV reactivation by focusing on the use vs. nonuse of prophylactic antiviral agents, but our study is the first randomized controlled clinical trial to focus on the difference in the effect of HBV reactivation according to the duration of prophylactic antiviral drug use.
There are several limitations in this study. First, a large proportion of enrolled patients in this study were lost to follow-up and so the power to see statistical differences in outcomes was lost. Poor adherence to antiviral prophylaxis may be explained by the patients not being aware that they are at risk for hepatitis. Patients’ chemotherapy schedules, disease progression, and experience of adverse effects to medication may also be factors in discontinuing treatment. Greater non-adherence in patients on long-term prophylactic therapy underscores the result in our study that short-term prophylactic antiviral treatment was sufficient in terms of efficacy and safety. Second, since this study was designed as a superiority test, the interpretation of the results is limited. To validate the results of this study, a non-inferiority-designed study is needed to compare the efficacy of 6- and 12-month use of prophylactic TDF in patients with resolved HBV using rituximab.
In conclusion, prophylactic TDF up to 6 months after completion of rituximab-based chemotherapy is sufficient in terms of the efficacy and safety of reducing HBV reactivation in HBsAg-negative and anti-HBc-positive non-Hodgkin lymphoma patients treated with rituximab-based chemotherapy.
 XML Download
XML Download