

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of end-stage renal disease (ESRD) in the United States was 2,242 cases per million people in 2018, the highest prevalence in the world. Kidney transplantation (KT) has been the treatment of choice for a minority of patients with ESRD since the 1960s, and at the end of 2018, there were 229,887 patients with a functioning KT in the United States.1 The prevalence of anemia in people with chronic kidney disease and that in patients with ESRD was 15.4% and 53.4%, respectively, in the United States.2 Therefore, red blood cell (RBC) transfusion is considered unavoidable during the peri-transplant period due to the high prevalence of anemia and blood loss during surgery.34 Sensitization to human leukocyte antigens (HLAs) expressed on the surface of leukocytes and platelets in blood units can be caused by factors including previous transplant, pregnancy, or blood transfusion.56 Several studies have shown that RBC transfusion is an important cause of alloimmunization and is associated with increased rejection and graft loss.789101112
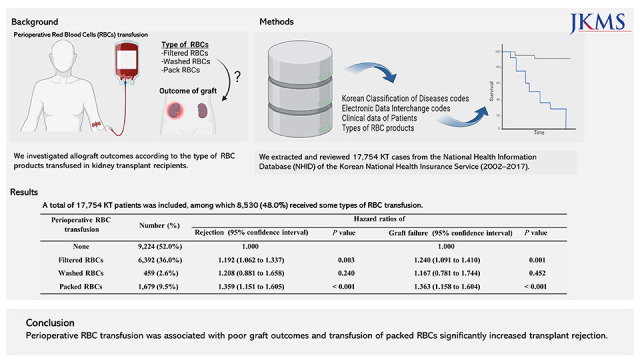
Based on these results, it has been suggested that active efforts to minimize blood transfusion are required to prevent HLA sensitization and to improve kidney allograft outcomes. Appropriate management of perioperative RBC transfusion is a critical factor in KT patient outcomes as more than half of all kidney recipients receive transfusions. The consequences of perioperative transfusion on graft outcomes have been continuously evaluated.131415 however, there remain unexplored factors that are potentially relevant to patient prognosis. With respect of the type of RBC unit preparation, the risk of allosensitization in patients with chronic kidney diseases is considered to be lower with leuko-reduced RBCs.9 Methods for leukocyte depletion from RBC products include centrifugal precipitation, filtration, and red cell washing. In the past, centrifugal precipitation and red cell washing were generally used. In these days, the filtering method is used to reduce leukocytes conveniently and effectively in blood components and achieves residual leucocyte counts of < 5 × 106.1617 However, in practice, packed RBCs (pRBCs), filtered RBCs, and washed RBCs have been heterogeneously transfused into KT recipients.14 Moreover, the impact of transfusion of different types of RBC preparations on transplant outcomes is unclear, and to our knowledge, the clinical significance of the type of RBC unit preparation and graft outcome has not been evaluated in existing studies. Therefore, to better answer this practical question about which type of RBC products are suitable for patients, we investigated the associations between the transfusion of different types of RBC preparations and kidney allograft outcome using a nationwide database linked to the Korean National Health Insurance Service (KNHIS).18 Thus, the current study aimed to investigate the outcomes of KT in South Korea over a 16-year period using a KNHIS nationwide database and to evaluate the association with poor prognosis after transplantation according to the type of RBC product transfused.
METHODS
Data source and study subjects
The KNHIS was implemented in 1988 and controls all medical costs among individuals, health care providers, and the government in South Korea. Medical data, including personal information, diagnosis, medical treatment, and demographics of patients, are centralized in the National Health Information Database (NHID) of the KNHIS.18 The NHID provides de-identified data for research purposes, and we collected detailed patient characteristics of all transplant recipients within this registry. The KNHIS-NHID includes the diagnosis of patients according to the Korean Classification of Diseases codes, which is the Korean version of the International Classification of Diseases (ICD). All insurance claims are classified based on Electronic Data Interchange (EDI) codes.
We extracted data on patients who underwent KT between 2002 and 2017 from the KNHIS-NHID using the specific EDI code (R3280) for KT. Among 18,331 KT patients, we excluded patients who received transfusions of two or more types of RBCs. Finally, we analyzed 17,754 KT cases.
Variable definitions
We investigated the sex, age, type of donor (living or deceased), income level, type of hospital, year of surgery, length of hospital stay, regimen of induction treatment, types of initial immunosuppressant and steroid regimens, and occurrence of acute kidney allograft rejection or graft failure. Since the characteristics of the KNHIS claim data make it difficult to specify the exact time of kidney allograft rejection, acute rejection was defined as any case in which a diagnosis of kidney allograft rejection, as identified by ICD-10 codes T86 and/or T86.1, was recorded during the KT-related hospitalization period. Graft failure was defined as a KT recipient undergoing repeated dialysis for three months or longer during the post-KT follow-up period.19 The Organ Transplantation Act of South Korea requires a recipient to pay for the cost of donor nephrectomy in the case of living-donor KT, while the government covers the primary cost for organ donation in the case of a deceased donor. Therefore, the donor type was able to be classified as a living donor when the EDI code for donor nephrectomy ‘R3272’ was charged to a recipient. In addition, among living-donor KT recipients, ABO-incompatible KT was defined as a transplant procedure where ABO antibody tests (EDI code B2080) were performed two or more times during the KT-related hospitalization, and plasma exchange (EDI code X2505) was performed concurrently. The proportions of deceased- or living-donor KT recipients in this study were consistent with the statistics from the Korean Network for Organ Sharing (KONOS). The codes or criteria for defining variables in building a database have been described in previous studies.1920 Because death certificates are automatically reported to the KNHIS, mortality was detected when healthcare coverage by the KNHIS was terminated.
The number and types of RBC products used in the subjects during hospitalization were analyzed. However, the NHID did not provide pre- and post-transplant information separately. Therefore, we investigated the associations between the type of perioperative RBC product received and short- and long-term transplant outcomes. We divided the subjects into four groups based on whether they had undergone RBC transfusion and the type of RBC product transfused. The four groups consisted of patients without RBC transfusion and patients transfused respectively with filtered RBCs, washed RBCs, or pRBCs. One unit of pRBCs contains approximately 200 or 250 mL of blood products separated from 320 or 400 mL, respectively, of donor whole blood. The types of RBCs were identified based on the KNHIS EDI codes for medical procedures regarding the types of RBC products; X2021, X2022, X2031, X2032, X2111, and X2112.
Statistical analyses
The Mann-Whitney U and Kruskal-Wallis tests were used to compare continuous variables among subject groups, and the χ2 test was used to compare categorical variables. Graft survival and rejection-free survival were calculated using Kaplan-Meier survival analyses. Data were censored at the time of death or at the last available follow-up. Cox’s proportional hazard regression was conducted to construct multivariate models for identifying factors associated with occurrence of acute kidney allograft rejection or chronic kidney allograft failure, and hazard ratios (HRs) for risk factors with 95% confidence intervals were calculated. All statistical analyses were performed using SAS 7.15 (SAS Institute Inc., Cary, NC, USA) and RStudio v1.1.463 (RStudio Inc., Boston, MA, USA), and P values less than 0.05 were considered to be statistically significant.
Ethics statement
This was a retrospective cohort study, and the protocol was implemented after approval from the Institutional Review Board (IRB) of National Health Insurance Service Ilsan Hospital (Approval No. NHIMC 2021-09-020). Informed consent was waived by the IRB. The administration number of the National Health Insurance Sharing Service was NHIS-2022-1-101 (REQ202104307-004).
RESULTS
Patients and baseline characteristics
We reviewed a total of 17,754 KT recipients included in the KNHIS-NHID between 2002 and 2017. The median post-KT follow-up period was 66 months (mean 73.1 months; range, 0 to 194 months; 1st to 3rd quartiles, 28 to 109 months). The proportion of males was greater in the group without RBC transfusion. The most common age group among KT recipients was 40–59 years old, representing 56.9% to 64.5% of patients depending on the type of RBC product received (Table 1).
Table 1
Kidney transplant patient characteristics according to the type of perioperative RBC transfusion
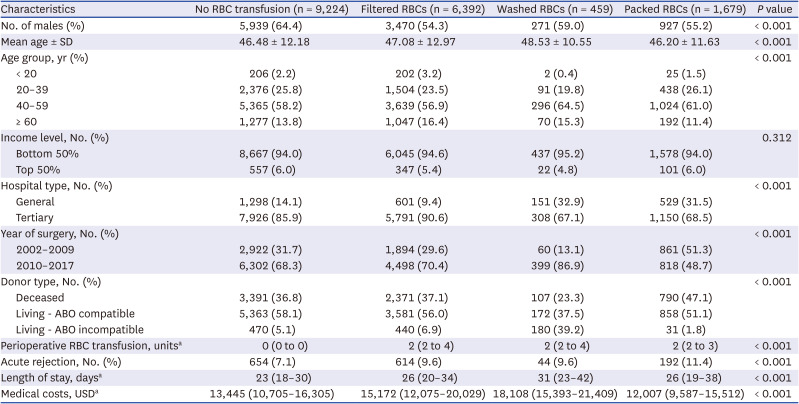
Significant differences among the four groups according to the types of RBC product administered to KT recipients were found for sex, age group, hospital type, year of surgery, donor type, history of acute rejection, length of hospital stay, and medical costs for hospitalization (P < 0.001). Compared to general hospitals, tertiary hospitals more frequently did not transfuse any RBC products and, when needed, tended to use filtered RBCs rather than other types. Washed RBCs were more frequently transfused in cases of ABO-incompatible living-donor KT. Acute rejection was more frequently diagnosed in KT recipients transfused with pRBCs, whereas it occurred less frequently in patients without RBC transfusion. In addition, patients who did not receive RBC transfusion had shorter length of hospital stay (Table 1).
RBC transfusion depended on the type of preparation
All patients were divided into four groups depending on the type of RBC preparation received. A total of 9,224 patients did not receive RBC transfusion during the perioperative period, and 8,530 (48.0%) of 17,754 KT recipients were transfused with some type of RBC product during the perioperative period. Among these 8,530 patients, 74.9% (n = 6,392) received filtered RBCs, 19.7% (n = 1,679) received pRBCs, and 5.4% (n = 459) received washed RBCs. Transfused patients received a median of 2 RBC units during the perioperative period, regardless of type of RBC preparation (Table 1).
A total of 30,889 RBC units was transfused into patients perioperatively in 77 hospitals between 2002 and 2017. Filtered RBCs were most frequently used, followed by pRBCs. Washed RBCs were used in 27 of the 77 institutions from 2002 to 2017. Regardless of the type of RBC preparation transfused, the average amount of RBCs used per patient and that of RBCs used per hospital were 3.6 and 406.4 units, respectively. The median transfusion incidence among hospitals was 50.6% (1st to 3rd: 37.7% to 72.0%; Table 2).
Table 2
Perioperative RBC use according to the type of transfused units

Acute rejection and rejection-free survival after KT
The incidence rate of acute rejection in KT patients during hospitalization over the study period was 8.5% in this study. The proportion of patients with acute rejection was significantly greater in women; in the 20–39 and 40–59 age groups; in patents with an earlier year of transplantation, receiving an allograft from a deceased donor, or treated with anti-thymocyte globulin (ATG); and in those receiving cyclosporine rather than tacrolimus or dexa/betamethasone or fludro/hydrocortisone as initial immunosuppressants (Supplementary Table 1). Types of RBC preparations were transfused inconsistently to KT recipients depending on the institution. We investigated the association between transfusion of different types of RBC preparations and acute rejection. Regardless of RBC product (filtered RBCs, washed RBCs, or pRBCs), the proportion of patients with acute rejection was significantly greater among patients receiving transfusion (P < 0.001) (Supplementary Table 1).
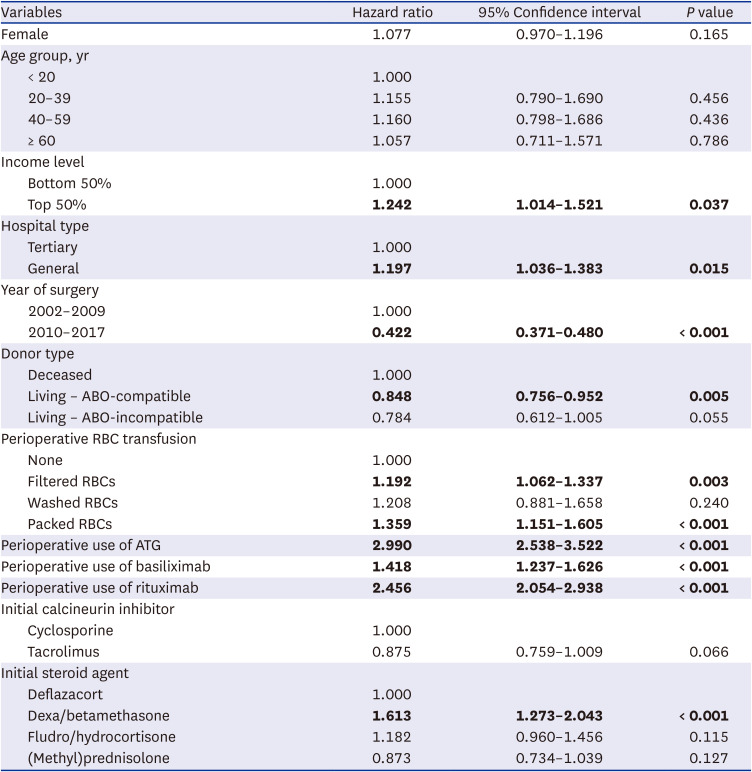
Multivariate analyses indicated that the HRs for rejection after KT in patients with incomes exceeding the median, KT at general hospitals or in more recent year of transplantation, and KT received from living ABO-compatible donors were independently significant at HRs of 1.242, 1.197, 0.422, and 0.848, respectively. The HRs in the patients receiving ATG, basiliximab, rituximab, and dexa/betamethasone compared to deflazacort were also statistically significant at 2.990, 1.418, 2.456, and 1.613, respectively (Table 3). The HRs for rejection in the filtered RBC and pRBC groups compared to the KT recipients without RBC transfusion were 1.192 and 1.359, respectively. Although it was not statistically significant, the washed RBC group also had an increased HR of 1.208 compared with the no RBC transfusion group (Table 3).
Table 3
Multivariate Cox proportional hazard model of risk factors of rejection during post-kidney-transplantation follow-up
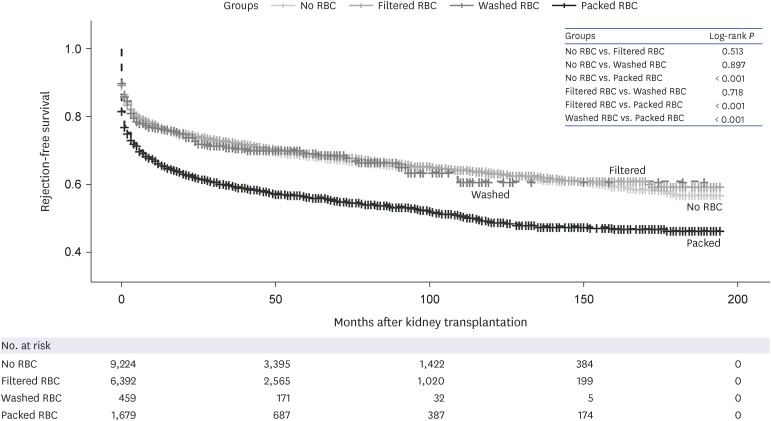
In Kaplan-Meier analyses of the four groups (no transfusion, filtered RBCs, washed RBCs, and pRBCs), the log-rank test indicated poorer rejection-free survival of the KT patients being transfused with pRBCs than other groups (no transfusion, filtered RBCs, and washed RBCs) during the post-KT follow-up period (P < 0.001) (Fig. 1).
Graft failure
Graft failure occurred in 7.2% of kidney transplant recipients during the follow-up period. The proportion of patients with graft failure was significantly greater in males; in the 20–39 age group; and in patients with an early year of transplantation, receiving an allograft from a deceased donor, or receiving cyclosporine treatment. Patients who developed cytomegalovirus (CMV) infection within 1 year after KT and those with a history of acute rejection comprised significantly larger proportions of the graft failure group (Supplementary Table 2).
In the Cox regression model, an inverse association with graft failure was found for females, with an HR of 0.816, and for patients who received a KT from a living ABO-compatible donor (HR, 0.820). The most important risk factor for graft failure was a recent year of transplantation, with an HR of 9.393. The HRs for acute rejection history; CMV infection within 1 year after KT; and perioperative treatments such as ATG, basiliximab, and rituximab ranged from 1.357 to 1.957 (Table 4).
Table 4
Multivariate Cox proportional hazard model for risk factors of graft failure among kidney transplant recipients
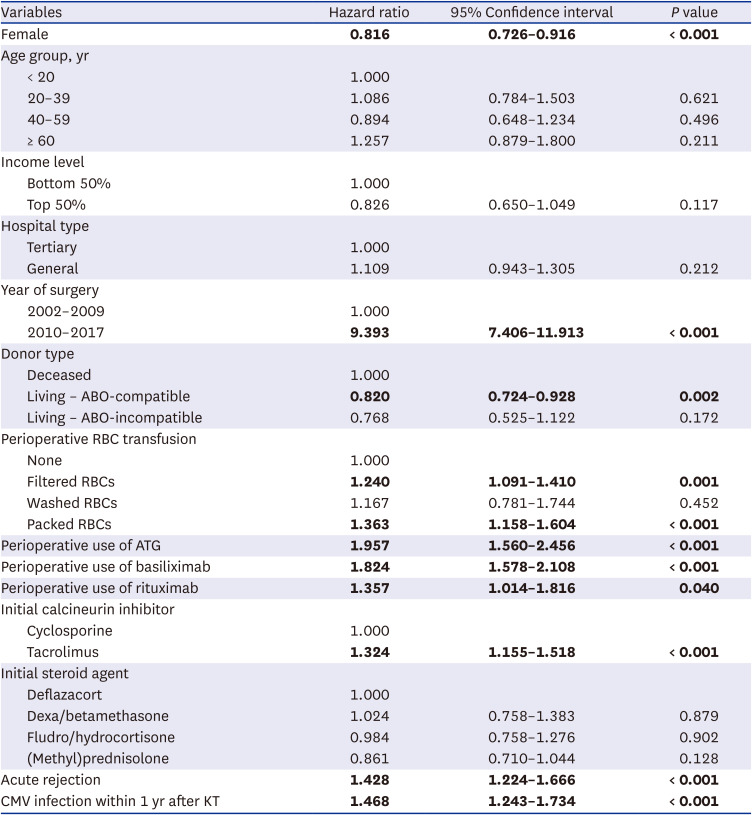
The proportion of patients with graft failure was significantly greater in those receiving transfusion (P < 0.001) (Supplementary Table 2). The HRs for graft failure in filtered RBC and pRBC groups compared with those without RBC transfusion were 1.240 and 1.363, respectively. The washed RBC group showed an HR of 1.167 for graft failure, but this finding was not statistically significant (P = 0.452; Table 4).
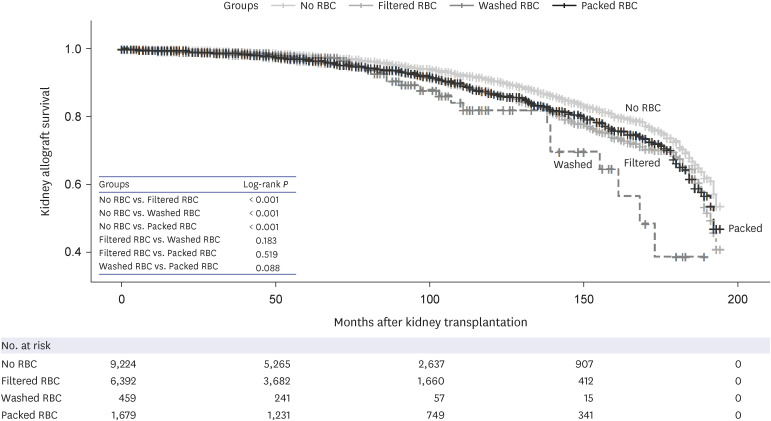
Patients who did not receive perioperative RBC transfusion had significantly greater overall graft survival than the patients transfused with filtered RBCs, washed RBCs, or pRBCs (P < 0.001 for each comparison) according to Kaplan-Meier analysis. Graft survival was not significantly different among the groups transfused with different RBC products (Fig. 2).
Fig. 2
Kidney allograft survival according to the type of RBCs transfused perioperatively at kidney transplantation. The patients who did not receive any RBC product perioperatively showed longer overall graft survival than the groups being transfused with filtered RBCs, washed RBCs, or packed RBCs (P < 0.001 for each comparison). Graft survival was not significantly different among the groups transfused with different types of RBC preparations.
RBC = red blood cell.
DISCUSSION
The results of this study using nationwide data from the KNHIS-NHID (2002-2017) indicate differences in transplant outcomes among Korean KT recipients according to the type of RBC product transfused during the perioperative period. Given the high prevalence of intraoperative anemia and bleeding during the peri-transplant period, RBC transfusion is often unavoidable.34 The reported percentage of KT patients receiving post-transplant transfusion has ranged from 28.0% to 37.2% in Canada and France,1521 and 49.7% of KT recipients received RBC transfusion during the perioperative period in Korea.19 When we excluded patients who received transfusions of two or more types of RBCs, 48.0% of 17,754 KT recipients received RBC transfusion during the perioperative period between 2002 and 2017.
Generally, in order to reduce the risk of allosensitization, leuko-reduced RBCs are preferable for KT recipients9; however, in practice, several additional types of RBC preparations including pRBCs, filtered RBCs, and washed RBCs have been transfused into Korean patients.19 Of the 8,530 patients who received RBC transfusion, 74.9% received filtered RBCs, 19.7% received pRBCs, and 5.4% received washed RBCs. Among the 77 institutions included in this study, 64 and/or 27 respectively used pRBCs and/or washed RBCs (Table 2). In this study, the percentage of patients with both acute rejection and graft failure was significantly greater among those receiving RBC transfusion (P < 0.001). Also, regardless of perioperatively transfused RBC product, similar patterns of association were found in patients with rejection or graft failure. The filtered RBC and pRBC groups were significantly associated with both rejection during follow-up after KT and graft failure in the long term. The washed RBC group showed HRs of 1.208 and 1.167 for rejection and graft failure, respectively, although these were not statistically significant (Tables 3 and 4); this finding may have been due to insufficient statistical power, since the washed RBC group accounted for only a small fraction (2.6%) of the total cases in this study. Cox’s multivariate models indicated that transfusion of pRBCs was associated with the worst transplant outcomes among the four groups in this study.
The impact of transfusion of different types of RBC preparations on long-term transplant outcomes is uncertain. However, a few previous studies have evaluated the potential adverse outcomes associated with transfusion regardless of RBC product type.1521222324 We assessed the association between the type of transfused RBC products and acute rejection using a nationwide population-based database. In the survival analyses, rejection-free survival was significantly lower in the pRBC group than in the no RBC transfusion or filtered or washed RBC groups (Fig. 1). The use of pRBCs is declining, as they have been increasingly replaced by filtered RBCs, but pRBCs were still used in 6.7% of KT recipients between the 2014 and 2017 in Korea.14 Therefore, when perioperative RBC transfusion is necessary in KT recipients, transfusion of leuko-reduced RBCs should be recommended to lower the risk of kidney allograft rejection.
We also found graft survival to be significantly better in patients without RBC transfusion than in the cases transfused with any type of RBCs. Few prior studies have reported the effects of perioperative blood transfusions on transplantation outcomes.152124 In a study using data from the national database of the French transfusion service, Gaiffe et al.15 reported that both pre- and early post-transplant transfusions were associated with increased transplant failure. Our data also showed that KT recipients without RBC transfusion in the perioperative period had better graft survival. Although perioperative RBC transfusion was significantly associated with poor outcomes, it cannot be concluded that transfusion of RBCs is the direct cause of graft failure, since patients who were in poorer clinical condition at the time of KT are more likely to receive RBC transfusion.
On the other hand, there was no clear associations between a specific type of RBCs and graft survival. Exposure to non-self HLA through RBC transfusions may lead to the development of donor-specific HLA antibodies (DSAs) against the kidney allograft donor. Avoiding transfusions or using HLA-matched blood could reduce graft failure.2223 Therefore, further evaluation of additional data, such as utilization of HLA-matched blood and DSA results, is required to more thoroughly assess the associations between transfusion with specific types of RBCs and long-term KT outcomes, including graft failure.
Washed RBCs have been considered for reducing exogenous anti-A or anti-B antibodies and HLA sensitization in ABO-incompatible transplantation.2526 Washed RBCs were transfused into KT recipients at 27 of the 77 institutions in our nationwide cohort. However, there was insufficient evidence to support the effectiveness of the use of washed RBCs in KT recipients. In addition, Aston et al. reported that washed RBCs did not further reduce patient HLA sensitization over the use of filtered RBCs,27 and our findings showed that transfusion with washed RBCs did not lead to better graft outcomes than that with filtered RBCs, although this finding was not statistically significant (Fig. 2). Therefore, in consideration of the clinical efficacy, risk of infection due to contamination, and labor and time required to manufacture washed RBCs, our findings do not support the use of washed RBCs for KT recipients.
This study analyzed KNHIS-NHID data from a 16-year period to determine the associations between the type of RBC preparation transfused and KT outcomes among 17,754 patients who underwent KT for the first time. Due to the limitations of the data related to health insurance claims, we were not able to distinguish between pre- and post-operative RBC transfusions, and we were also unable to obtain detailed clinical information about the KT patients, such as the exact timing of acute rejection occurrence and results of laboratory tests which are not included in the national database. Many factors would influence KT outcomes in the pre- and post-transplantation period, such as renal function, hemoglobin level, allosensitization, pre-existing diseases, and case volume of centers.132829303132 Unfortunately, these data could not be analyzed in this study because they have not been collected and organized in the KNHIS-NHID. The impact of post-transplantation anemia and the clinical significance of de novo DSA on KT outcomes were also studied.12293334 However, the relationship between these factors and types of transfused RBCs has not been sufficiently studied. Further researches with comprehensive clinical data from each medical institution would be necessary.
In addition, we used an operational definition to determine whether the KT recipient and donor were ABO-compatible and whether the donor type was living or deceased. Despite these shortcomings, our data have identified an association between RBC transfusion and short- and long-term graft outcomes among Korean patients who underwent KT during a recent 16-year period.
Perioperative RBC transfusion was associated with an increased risk of kidney allograft rejection and long-term chronic graft failure. Notably, the transfusion of pRBC preparations increased the likelihood of rejection. Therefore, careful consideration of indications for RBC transfusion and selection of the appropriate type of RBC is necessary, especially for patients at high risk of rejection or graft failure. In addition, our data may support future revision of guidelines for clinicians regarding RBC transfusion of KT recipients and the development of computerized order entry system alerts when ordering pRBCs for KT recipients.
 XML Download
XML Download