

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hepatocellular carcinoma (HCC) is the 7th-most common malignant neoplasm in the world and has a high cancer-related mortality rate [1]. HBV and HCV infections account for the major etiology of liver cirrhosis and HCC; however, vaccinations and antiviral agents have contributed to the decline of virus-associated HCC [2]. On the other hand, non-alcoholic fatty liver disease or alcoholic liver disease have come to the fore as major contributors to HCC globally [3]. Although surgical resection is recommended as curative treatment for patients with HCC, its indication is restricted due to underlying cirrhosis or remnant liver function [4]. Liver transplantation (LT) is another curative treatment option for patients with HCC, providing a cure for both malignancy and cirrhosis [5]. Since the Milan criteria were introduced to optimize the outcome of LT for patients with HCC, several studies have emerged to prevent the removal of patients from LT waitlists owing to tumor progression beyond the Milan criteria [6].
Recently, several LT centers have shifted their focus to tumor biology from tumor morphology as indicated by the Milan criteria, with different surrogate markers, such as α-FP, PET positivity, and the radiological response of HCC to locoregional treatment (LRT) [78]. In particular, the bridging treatment for HCC using LRT before LT has been widely achieved and is reportedly associated with favorable outcomes [910]. The results of many studies suggest that the outcome depends on the necrotic portion of the tumor; total necrosis of the HCC with a complete pathological response prior to LT has yielded the best results [1112]. In theory, when total necrosis of HCC is achieved via LRT, it has no malignant viability. Nonetheless, the induction of total necrosis of HCC may be difficult to achieve, especially for patients with large tumors. Hence, the aim of this study was to investigate the prognosis of totally necrotic nodules diagnosed via explant pathology after LT and to determine the rate of tumor recurrence even after achieving a theoretically tumor-free status.
METHODS
The Institutional Review Board of our hospital approved this study (No. 2207-137-1342), and the requirement for informed consent was waived owing to its retrospective nature.
Patients
A total of 175 patients were histologically confirmed to have totally necrotic nodules (100% necrosis) without viable HCC from their explanted liver after LT in our hospital from January 2000 to December 2020. Of these, 10 (5.7 %) were excluded from the analysis owing to the following reasons: 8 patients died within 1 month of LT due to cardiogenic or pulmonary complications; 1 patient had a primary non-functioning graft and underwent retransplantation, but died of sepsis after the second operation; and 1 patient was lost to follow-up after LT.
Finally, 165 patients were analyzed, among whom 5 exhibited HCC recurrence during follow-up. Variables included for analysis were age, sex, body mass index (BMI), underlying liver disease, laboratory data (including α-FP and protein induced by vitamin K absence or antagonist-II [PIVKA-II] with matched Model for End-Stage Liver Disease [MELD] score), imaging features (including fluorodeoxyglucose-PET positivity), explant pathological variables, the total number of pre-LT LRTs, and the time between the last LRT and LT. Modalities for LRT were transarterial chemoembolization (TACE), transarterial radioembolization, radiofrequency ablation (RFA) or microwave ablation, and percutaneous ethanol injection (PEI). Follow-up duration, overall survival, recurrence-free survival, and treatment management after recurrence were also included as variables. Explant pathological variables were total tumor number, maximum diameter of the tumor (the largest tumor in case of multiple tumors), and the existence of dysplastic nodules in the rest of the liver.
Statistical analysis
All analyses were performed using IBM SPSS Statistics for Windows (ver. 27.0, IBM Corp.). Continuous data are presented as mean ± standard deviation or median (range), and categorical data as frequency and percentage. Continuous variables were compared using the chi-square test or the Fisher exact test, whereas categorical data were compared using the Student t-test or Mann-Whitney test. Survival curves were constructed using the Kaplan-Meier method, and the differences between the curves were assessed using the log-rank test. Univariate and multivariate logistic regression analysis was used to assess the factors associated with recurrence. A P-value of <0.05 was considered statistically significant.
RESULTS
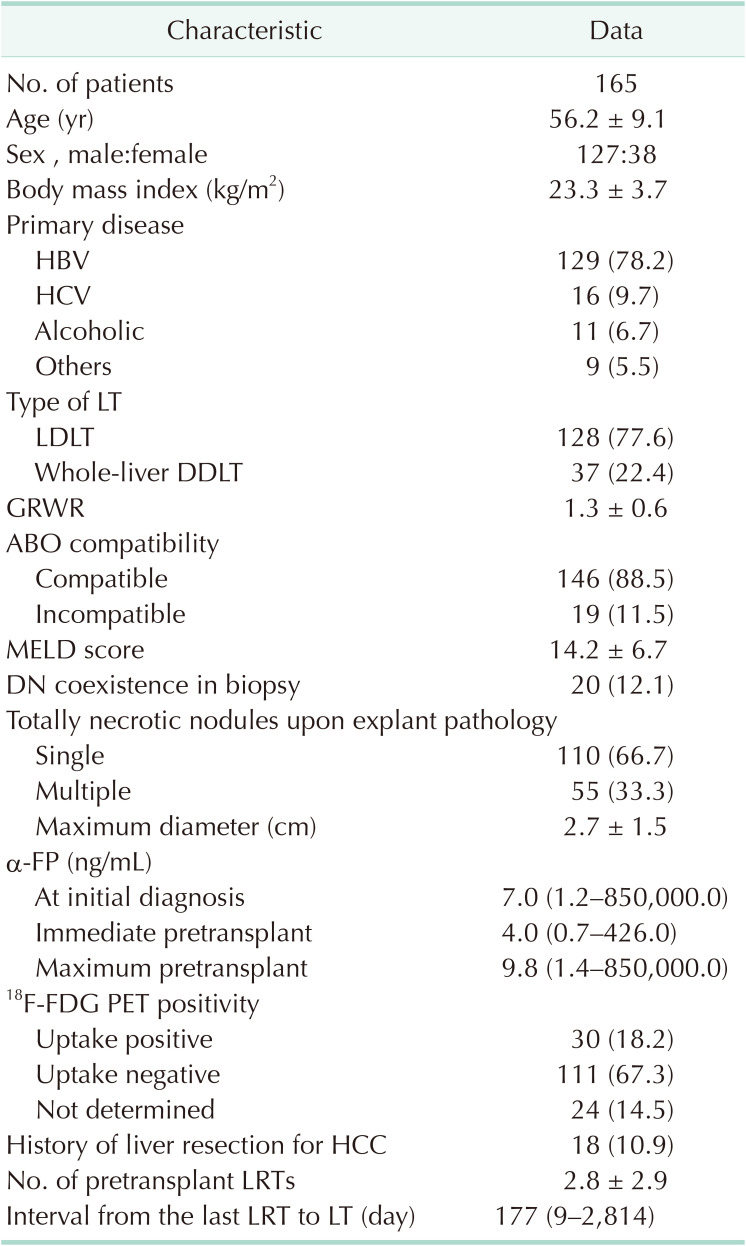
The baseline characteristics of the 165 patients (male, 77.0%) are summarized in Table 1. HBV infection was the main etiology of primary liver disease (78.2%) and 77.6% of patients underwent living-donor LT. The mean MELD score was 14.2. All the patients underwent pre-LT LRT (a median of 2.8 sessions), and the last LRT was performed a median of 177 days before LT. To determine the degree of agreement between the necrosis observed in the imaging study before transplantation and that found in the pathological results after transplantation, we reviewed all the results of the last imaging taken before transplantation. Of the 165 total patients, 160 patients underwent reexamination using CT or MRI before transplantation, and among these, 136 patients (85.0%) showed no marginal recurrence or viable tumor findings in the study. The remaining 24 patients showed T2 hyperintensity or subtle arterial enhancement that could be suspected to be viable tumor or marginal recurrence, although it was not definitively diagnosed.
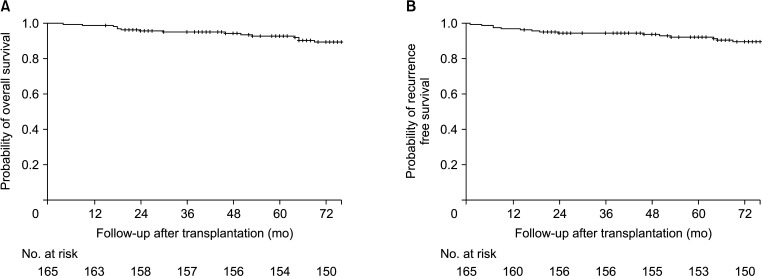
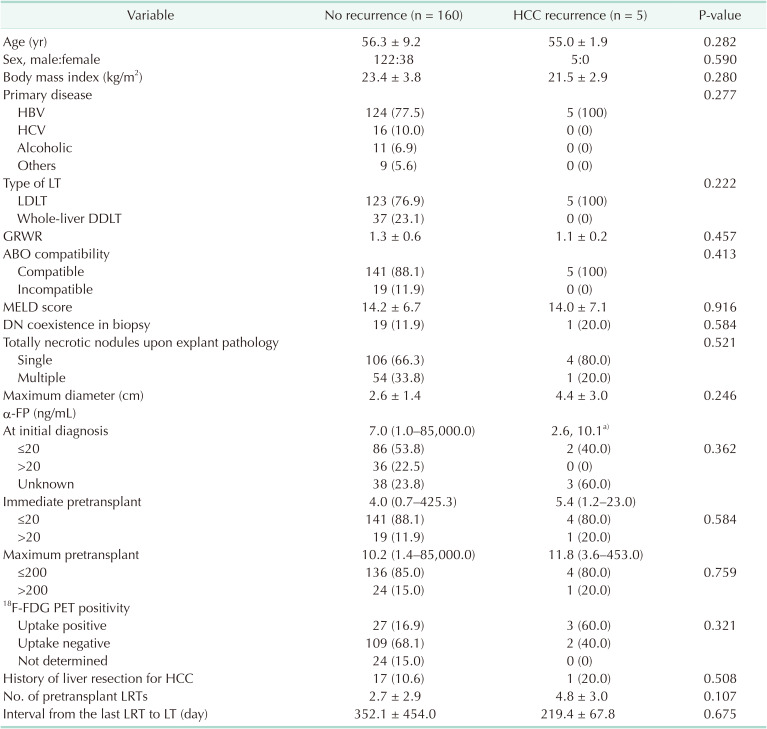
The median follow-up time after LT was 84 months (range, 4–243 months), with overall survival at 1, 3, and 5 years of 98.8%, 95.0%, and 92.8%, respectively. During follow-up, 5 patients (3.0%) developed HCC recurrence, and recurrence-free survival at 1, 3, and 5 years was 97.0%, 94.5%, and 92.2%, respectively (Fig. 1). We also performed a separate analysis comparing characteristics between the no-recurrence and HCC-recurrence groups (Table 2). Sex, age, and BMI did not significantly differ between the 2 groups. The underlying liver diseases in the no-recurrence group were HBV (n = 124, 77.5%), HCV (n = 16, 10.0%), alcoholic liver cirrhosis (n = 11, 6.9%), and others (n = 9, 5.6%), whereas all 5 patients (100%) with HCC recurrence had HBV-related HCC. In terms of explant histopathological characteristics, the total number and maximum diameter of the totally necrotic nodules did not significantly differ between the groups. α-FP values (≤20 and >20 ng/mL) at initial diagnosis and immediately pre-LT did not significantly differ between the groups. In terms of the maximum pre-LT α-FP, 85.0% in the no-recurrence group and 80.0% in the HCC-recurrence group had a concentration of ≤200 ng/mL.
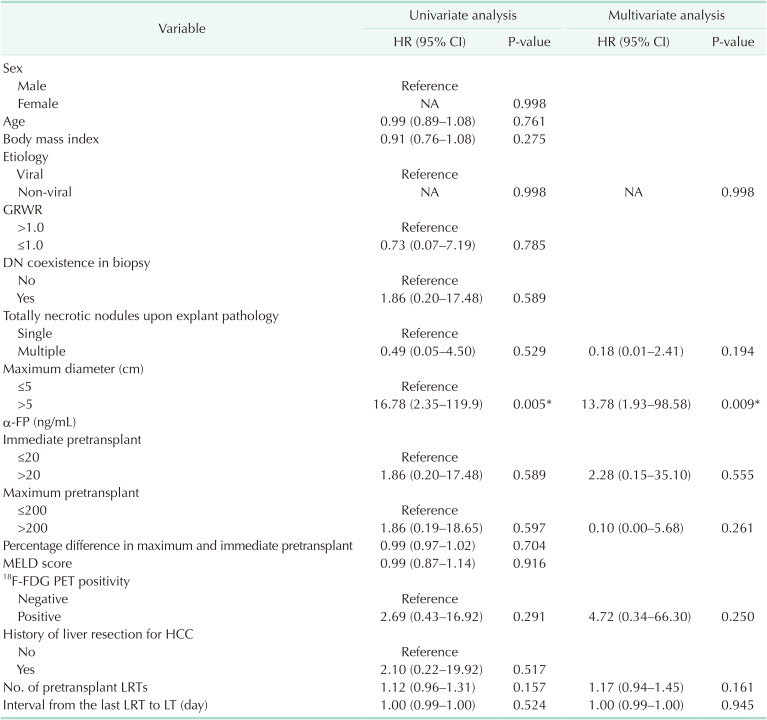
Univariate analysis of factors associated with HCC recurrence is described in Table 3. The only statistically significant predictor of recurrence was a totally necrotic nodules with maximum diameter of >5 cm (hazard ratio, 16.8; P = 0.005). Since only 1 significant factor was found in the univariate analysis, we analyzed in the multivariate analysis variables that are expected to be related to HCC recurrence. These variables included viral etiology, number of totally necrotic nodules, tumor size, number of pretransplant LRT, immediate pretransplant α-FP, maximum pretransplant α-FP, PET positivity, and days from last LRT to LT. The results showed that the risk of recurrence increased by 13.78 times when the tumor size was 5 cm or larger (P = 0.009).
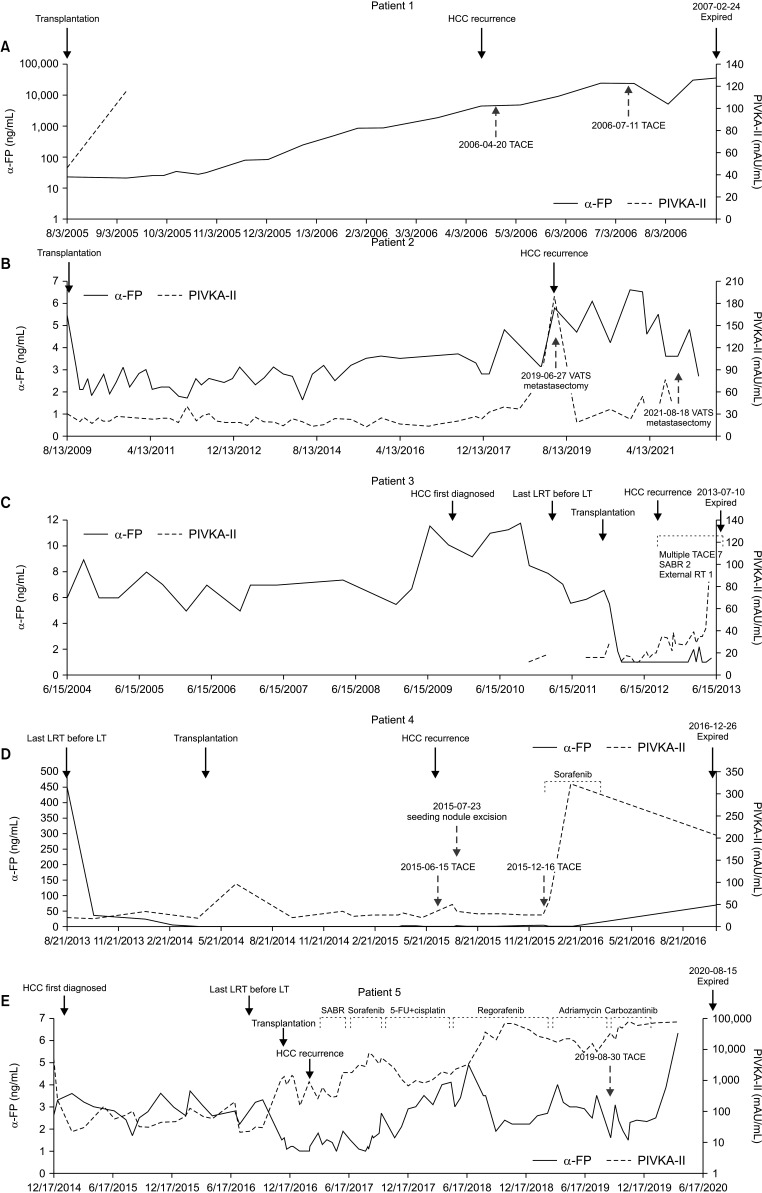
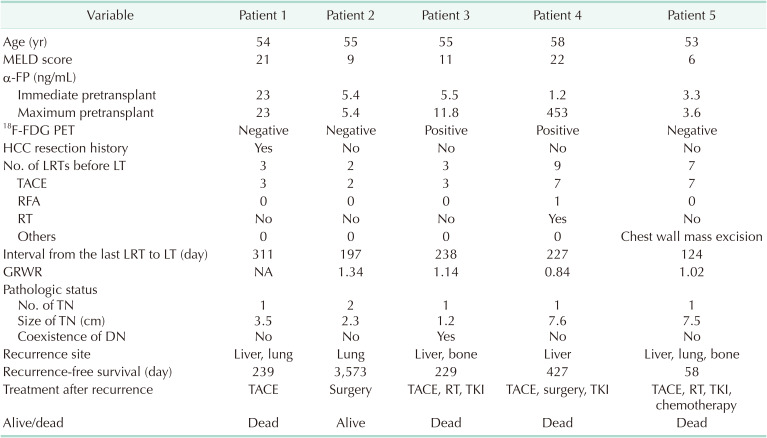
Table 4 summarizes preoperative data of each patient with HCC recurrence. They were all in their 50s and had HBV-related HCC. The size varied from 1.2 to 7.6 cm and each patient underwent multiple LRTs as shown in Table 4. Patient 4 had the highest maximum pre-LT α-FP concentration (453 ng/mL) and successfully responded to LRT (immediate pre-LT α-FP concentration, 1.2 ng/mL). Postoperative results and follow-up of these 5 patients are presented in Table 4, and tumor marker (α-FP, PIVKA-II) concentrations at various time points post-LT treatment are illustrated in Fig. 2. Patient 1 developed intrahepatic HCC recurrence 239 days after LT and underwent 2 rounds of TACE; however, he died of lung metastasis. As this patient had very poor compliance with immunosuppressant and antiviral drug use, HBV reactivation occurred, which may have affected the recurrence of HCC. Patient 2 developed a single metastatic pulmonary nodule; metastasectomy was successfully performed, and this patient was the only survivor in the HCC-recurrence group. Patient 3 had multiple bone metastases (in the right clavicle, L5 spinal vertebra, sacrum, and left ilium) in addition to intrahepatic recurrence. He underwent conventional radiotherapy and stereotactic ablative radiotherapy for bone metastases; however, the disease continued to progress. During the treatment period, his α-FP and PIVKA-II concentrations remained within normal limits. The patient’s PIVKA-II concentration increased to 117 mAU/mL just before he died, suggesting vitamin K deficiency due to poor oral intake. Patient 4 had a small-for-size graft and a large tumor. Nine months after LT, the patient had a biliary stricture and was admitted to the intensive care unit for biliary sepsis. When he developed HCC recurrence with peritoneal seeding, his tacrolimus regimen was reduced, and rapamycin was added. As the patient’s performance status was satisfactory and his tumor markers were maintained at a low level, peritoneal seeding nodules were excised to increase survival. In total, 9 peritoneal masses were excised, but recurrence was observed within 5 months. Patient 5 initially had a high PIVKA-II concentration rather than α-FP elevation at the time of HCC diagnosis. Before LT, he underwent chest wall resection and reconstruction owing to HCC metastasis. Four months later, with no evidence of tumor recurrence, LT was performed. When HCC recurred after LT, the patient’s α-FP concentration was still within the normal range, but his PIVKA-II concentration had increased to >100 mAU/mL. No definite intrahepatic HCC was observed, but a suspected tumor thrombus was discovered in the portal vein, along with multiple bone metastases. Even after multiple rounds of systemic therapy over 3 years, the disease progressed and the patient died.
DISCUSSION
Tumor recurrence after LT is a major concern and is caused by circulating tumor cells (CTCs) occurring before surgery [1314]. Several indications of HCC, such as the Milan or University of California-San Francisco criteria have been adopted by LT centers to predict the survival of patients with HCC undergoing LT; however, recent studies have demonstrated successful LT even for patients exceeding these criteria, with or without downstaging [1516]. Current decision-making for LT for patients with HCC highlights tumor biology rather than morphological characteristics, as implemented in Metroticket 2.0 and the Model of Recurrence After Liver Transplant score [1718]. Hence, the role of downstaging with LRT before LT is being emphasized even though the American Association for the Study of Liver Diseases and European Association for the Study of the Liver guidelines recommend bridging therapy with only a low level of evidence [1920]. Recent outcomes of downstaging for patients with HCC undergoing LT revealed a clear benefit of national downstaging policies, with a 10-year overall survival rate of 52.1% [2021]. Despite promising results, there has been lack of studies of recurrence even after achieving total necrosis of HCC before LT. This study details the fates of 165 patients with totally necrotic HCC who underwent LT.
In addition to the LT setting, tumor size of HCC has been shown to be associated with overall survival and recurrence after treatment in the hepatic resection setting [22]. According to our study, the only factor associated with tumor recurrence after LT was a tumor diameter of >5 cm. This corresponds to the Milan criteria. In patients beyond the Milan criteria, recurrence remains a possibility despite downstaging with LRT and total necrosis of HCC. CTCs in patients with HCC usually exhibit a downward trend after LT. However, CTCs remain detectable in patients’ serum even after hepatic resection or LT. Amado et al. [23] reported different concentrations of CTCs after LT depending on the presence of vascular invasion in the original tumors. Moreover, larger tumors are challenging to evaluate in terms of the exact pathological diagnosis; thus, caution is required owing to possibility of an unidentified remnant of viable tumor. In addition, it is typically challenging to achieve complete necrosis through LRT for large tumors, and such tumors have been identified as independent risk factors for intrahepatic metastasis, even after resection or LT [10]. While only 1 factor was found to be significant in univariate analysis, it is important to be cautious when interpreting the results of our multivariate analysis. Likewise, it was demonstrated that the risk of recurrence increases when tumor size is larger than 5 cm; however, since there were very few cases of recurrence, the correlation should be approached with care. Nonetheless, this result highlights the importance of active surveillance of cancer recurrence in patients beyond the Milan criteria who undergo LT, even with successful downstaging and complete pathological response.
Among the remaining variables in Table 3, neither PET positivity nor α-FP concentration, both of which are aspects of tumor biology, were significantly related to HCC recurrence. Rhu et al. [24] showed that the number of LRTs before LT is also associated with progressiveness of tumor biology. The number of recurrences increases the number of LRTs and indirectly indicates poor tumor biology. However, this variable was not significantly related to HCC recurrence in our study. The graft-to-recipient weight ratio, which represents the size of the graft, was positively related to the recurrence rate in a previous study [25], unlike in our study. However, our study is noteworthy in that we analyzed the post-LT recurrence factors in patients with totally necrotic HCC, which is considered to indicate no viability of malignancy.
The use of rapamycin, mammalian target of rapamycin (mTOR) pathway inhibitors, specifically reduces HCC tumor growth and simultaneously lowers the rejection rate of the graft [26]. However, no consensus on the point of initiation of administration of rapamycin has been established and its benefit in high-risk groups remains controversial [27]. Patient 4, who had the largest necrotic HCC (diameter, 7.6 cm) and highest maximum pre-LT α-FP concentration among the HCC-recurrence group, used a low dose of tacrolimus augmented with rapamycin for maintenance immunosuppression (Fig. 2). As the rapamycin administration was initiated after HCC recurrence, its antitumor effect is difficult to evaluate. However, in our previous study, mTOR inhibitor usage was associated with a better prognosis, especially in the late recurrence group (> 6 months), than no mTOR inhibitor usage [28].
Patient 2 was the only survivor in the recurrence group. He experienced lung metastasis twice without intrahepatic recurrence, which were both resectable. Most patients with lung metastasis exhibit a poor prognosis, with a 5-year overall survival rate of <5%, and aggressive management with repeated resection improves long-term survival [29]. The patient did not exhibit high α-FP or PIVKA-II concentrations after the first metastasectomy, demonstrating the importance of regular imaging studies in addition to tumor marker evaluation during follow-up in high-risk patients. Patient 5, who had a relatively large tumor (diameter, 7.5 cm), had the shortest time to recurrence. This patient had multiple metastases in his lungs and chest wall, which were surgically removed before LT. Distant metastasis at the time of LT is usually considered a contraindication; however, our center proceeds with transplantation if surgical removal is feasible and cure is expected, after informing the patient about the high possibility of recurrence and obtaining their consent. Even though he had a “tumor-free” status following LRT and metastasectomy, the tumor recurred shortly after LT.
Owing to its retrospective nature and small sample, this study lacked statistical power, and further analysis is needed. An absence of comparison between patients with total necrosis and those with partial necrosis of HCC after LRT may be considered a limitation of our study; however, the study by Agopian et al. [9] suggested improved recurrence-free and overall survival rates of patients within the Milan criteria with total necrosis compared with those with partial necrosis. Another limitation of this study is the failure to compare the prognosis of patients with total necrosis undergoing different LRT modalities, although TACE was the most frequently performed modality. Such a comparison was not feasible because many patients underwent LRT several times before undergoing LT, and many patients did not undergo only TACE but a combination of methods including RFA and PEI, depending on the tumor location. Bearing these limitations in mind, to the best of our knowledge, our study is the first to demonstrate the long-term fate of patients with HCC with a totally necrotic state at the time of LT. In connection with previously published research of 81.5% overall survival and 80.3% recurrence-free survival in the beyond Milan criteria group [30], this study shows far better outcomes of LT for HCC. These promising results suggest further methods to predict total necrosis before transplantation.
In conclusion, in our study, patients with total necrosis of HCC still exhibited a recurrence rate of about 3.0%, and the risk increased in patients with tumors sized >5 cm. Therefore, even if total necrosis is achieved through LRT before LT, thorough periodic testing of serum tumor markers and imaging studies should be performed in patients with large tumors (>5 cm) for timely detection of recurrence after LT.
 XML Download
XML Download