

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Abdominal aortic aneurysm (AAA) is an important vascular surgical condition, with AAA rupture being potentially life-threatening, with mortality rates as high as 80% [1]. Surgical methods have been found to improve patient care and survival. Endovascular aneurysm repair (EVAR) shows superior outcomes when compared to open surgical repair (OSR), including lower 30-day mortality rate, shorter operation times and length of hospital stay, decreased incidence of cardiac and pulmonary complications and blood transfusions, and higher cost-effectiveness [23].
Although EVAR has shown short-term survival benefits over OSR, especially during the perioperative period, these advantages were no longer observed during long-term follow-up, as EVAR is associated with high rates of complications and reinterventions [4]. These findings suggest a need for a different approach to patient care. To date, no large-scale studies have evaluated treatment outcomes in Korean patients with AAA, and little is known about the economic burden of this disease. A comprehensive, nationwide assessment of treatment outcomes in AAA may identify the need for additional approaches and provide insight into the expected healthcare costs associated with the treatment of this disease. The present study therefore utilized data from the National Health Insurance Service (NHIS) to determine the outcomes of EVAR and OSR and related costs in patients with AAA.
METHODS
In this retrospective cohort study, the NHIS database was searched to identify all Korean patients who underwent EVAR or OSR of an AAA between January 2008 and December 2019. Approval for data collection and publication was granted by Institutional Review Board of Asan Medical Center (No. 2020-1242), which waived the requirement for written informed consent because of the retrospective nature of the study. All methods were performed in accordance with relevant guidelines and regulations.
Data source
The demographic characteristics of each patient treated for AAA, along with their International Classification of Disease 10th revision (ICD-10) diagnosis codes, procedure codes, prescriptions, and survival, as both inpatients and outpatients were recorded. Also recorded were patients’ health screening data (e.g., health behaviors such as smoking or alcohol consumption) and the results of laboratory tests. Supplementary Table 1 shows the detailed definitions of comorbidities and procedures.
Study design and cohort definition
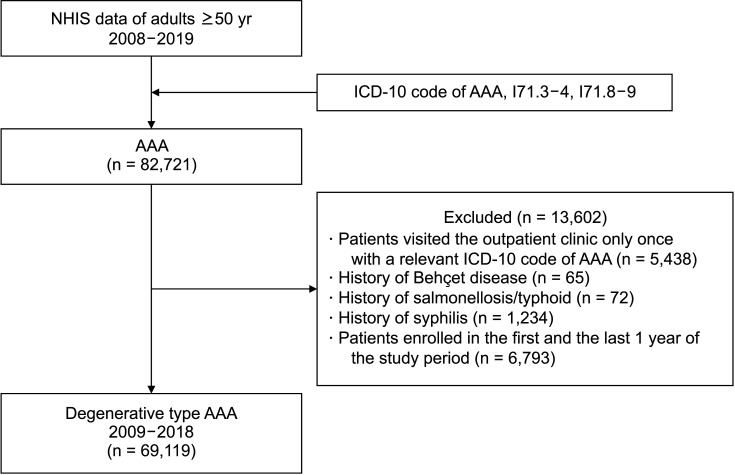
The study flow diagram is depicted in Fig. 1. Patients aged ≥50 years in the NHIS database who had been diagnosed with AAA (ICD-10 codes I71.3–4 and I71.8–9) between January 2008 and December 2019 were initially selected. Patients who had visited the outpatient clinic only once with a relevant ICD-10 code for AAA were excluded. To limit the study to patients with the degenerative type of AAA, patients with the AAA related to Behçet disease (ICD-10 code M35.2) or syphilis (ICD-10 code A50–53) were excluded, as were patients with a history of typhoid fever or salmonellosis (ICD-10 code A02, and procedure codes NHIS O2034, O2036, and O2039) within the 6 months prior to a diagnosis of AAA. Patients enrolled during the first 6 months and last 6 months of the study period were also excluded. The index date of AAA was defined as the first date of AAA diagnosis.
Study outcome
The primary outcomes were perioperative and long-term survival and complications. Perioperative complications or death were defined as complications or death within 30 days after the procedure. In-hospital death was defined as death during the index admission. Long-term all-cause mortality included all deaths during the follow-up period. The secondary outcomes were AAA-related reintervention rates and related costs. Complications were identified as primary or subsidiary, as determined by diagnosis and/or procedure codes. AAA-related reinterventions were defined using the relevant procedure codes, including percutaneous angioplasty, stenting, embolization, and thrombectomy or open thrombectomy. AAA-related costs included the index operation and associated hospitalization, follow-up imaging, and AAA-related reinterventions. Codes for complications and outcomes are summarized in Supplementary Table 1.
Statistical analysis
Categorical variables are presented as number (frequency) and compared by Pearson chi-square tests. Continuous variables are presented as mean and standard deviation and compared by Student t-tests as appropriate. Perioperative and long-term outcomes were compared, and odds ratio (OR) and corresponding 95% confidence intervals (CIs) were calculated with the EVAR group as a reference. For events such as mortality or reintervention, person-years (PY) at risk and events per 100 PY per group were calculated. Patient survival and reintervention related to AAA were determined by the Kaplan-Meier method and compared by log-rank tests. A Cox proportional hazard regression model was used to determine the adjusted hazard ratio (HR), with the EVAR group as a reference and corresponding 95% CIs for the association between EVAR and OSR. Reinterventions related to AAA and dialysis were calculated using a Fine and Gray subdistribution hazard model that considered death as a competing risk. All statistical analyses were performed using SAS Enterprise Guide software ver. 7.1 (SAS Institute) and R software ver. 4.0.3 (R Foundation for Statistical Computing), with the P-values of <0.05 considered statistically significant.
RESULTS
Demographic characteristics of patients who had undergone repair of AAA and annual incidence of AAA repair
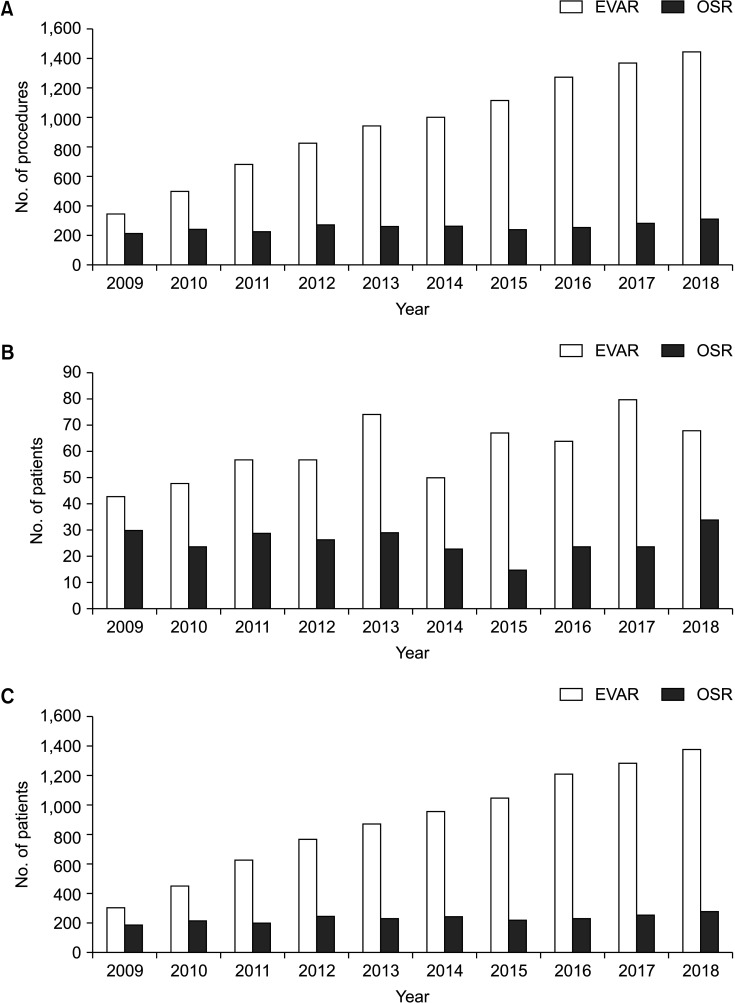
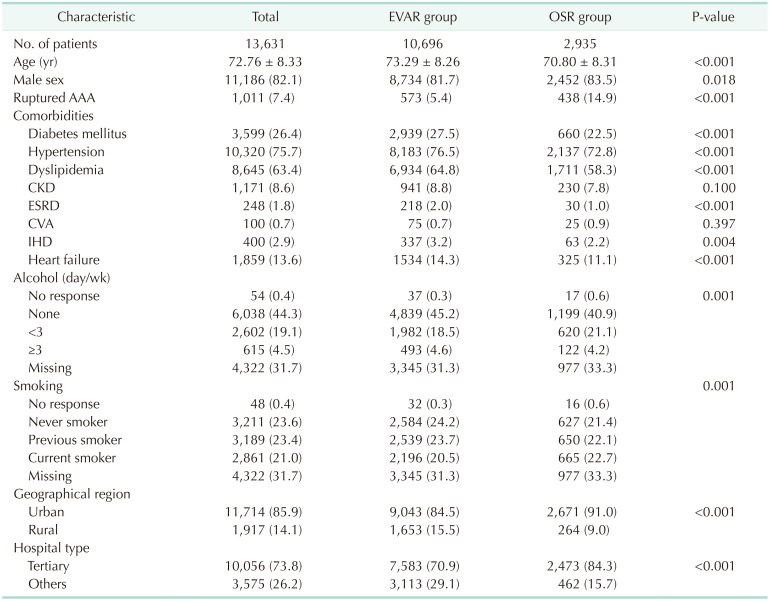
A review of the NHIS database identified 69,119 patients diagnosed with AAA patients from 2008 to 2019. Of these patients, 13,631 underwent repair of AAA, including 10,696 who underwent EVAR and 2,935 who underwent OSR. Their baseline demographic and clinical characteristics are shown in Table 1. Fig. 2 shows the number of procedures per year. The total number of procedures steadily increased during the study period, from 570 in 2009 to 1,767 in 2018 (Fig. 2A). While the number of patients aged 50–59 years who underwent procedures did not show a remarkable trend (Fig. 2B), the number of patients aged ≥60 years who underwent EVAR increased significantly, from 307 in 2009 to 1,371 in 2018 (Fig. 2C). There were no significant changes in the number of patients who underwent OSR throughout the study period (Fig. 2).
Perioperative outcomes
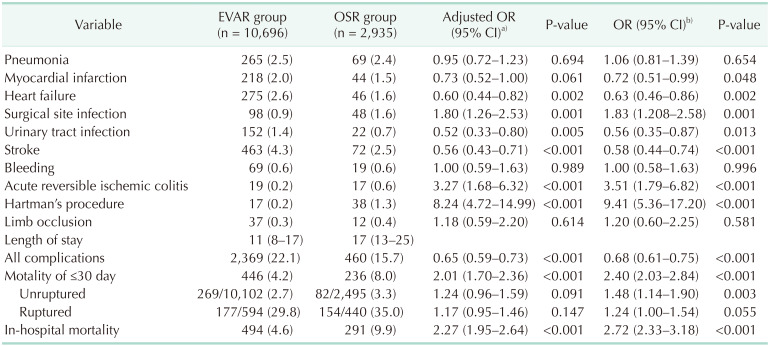
The overall perioperative complication rate was significantly higher in the EVAR than in the OSR group (22.1% vs. 15.74%, P < 0.001) (Table 2). Postoperative heart failure (P = 0.002) and stroke (P < 0.001) rates were significantly higher in the EVAR group, whereas the rate of surgical site infection was significantly higher in the OSR group (P = 0.001). The overall perioperative mortality rate was significantly lower in the EVAR than in the OSR group (4.2% vs. 8.0%; OR, 2.40; 95% CI, 2.03–2.84; P < 0.001), even after excluding patients with ruptured AAA (2.7% vs. 3.3%, P = 0.003). Since the age and sex distributions varied between the 2 groups of EVAR and OSR, and given their significant clinical impact on the risk of death, we selected them as adjusting variables. After adjusting for age and sex, the perioperative mortality rate of patients with unruptured AAA was significantly higher in the OSR than in the EVAR group (adjusted OR, 1.48; 95% CI, 1.14–1.90; P = 0.003).
Long-term outcomes
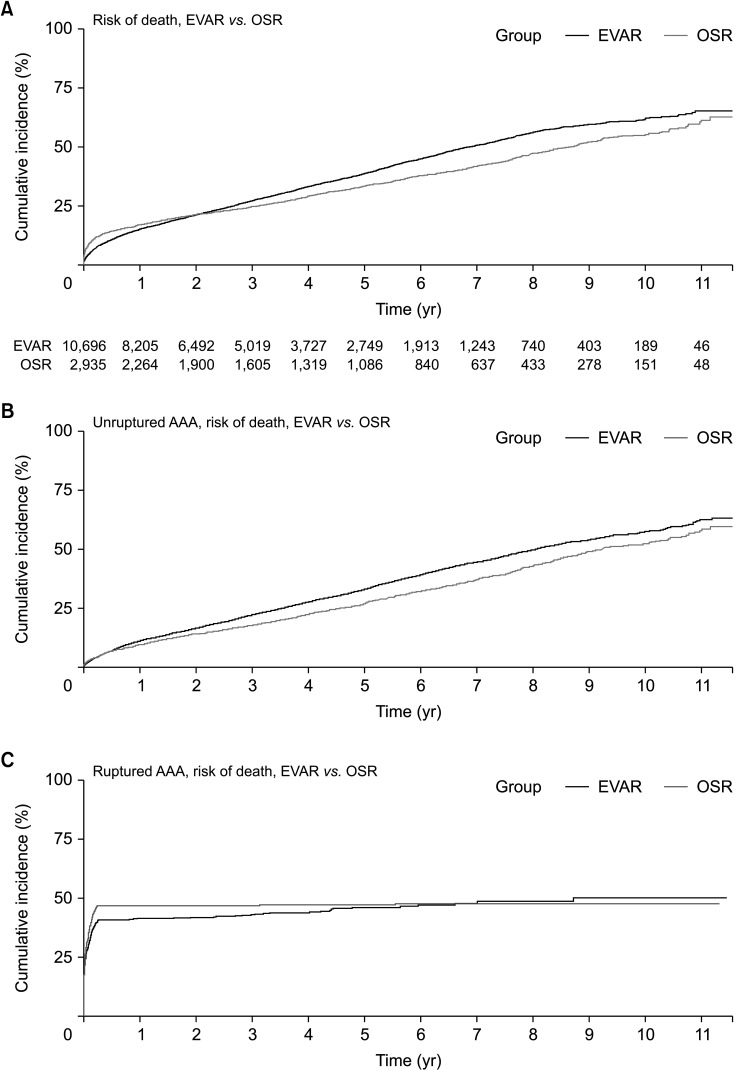
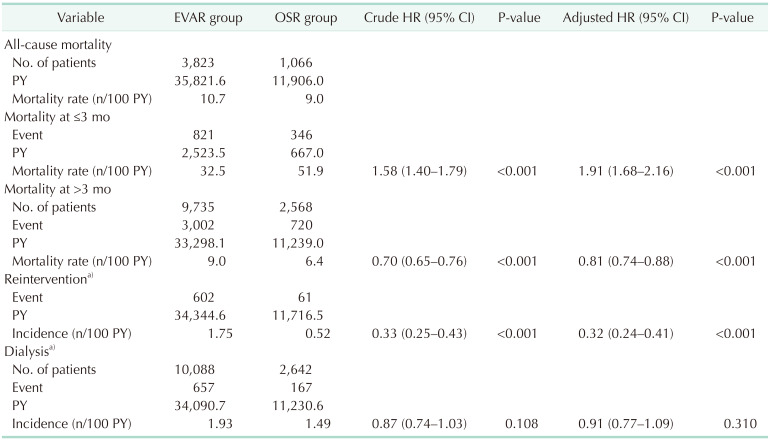
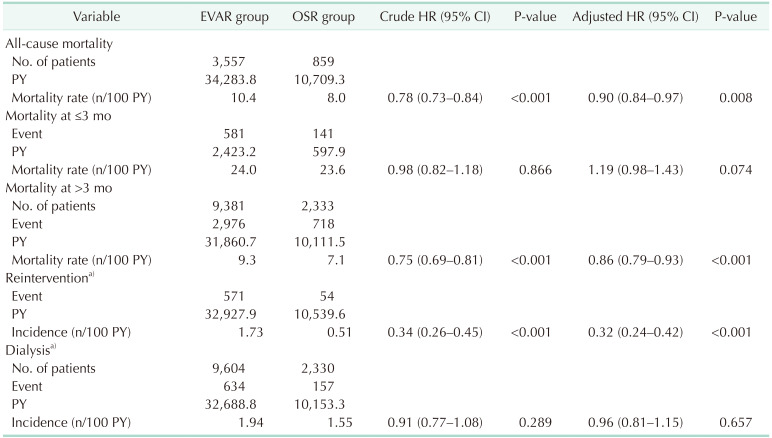
Median follow-up times after the initial procedure were 2.78 years in the EVAR group and 3.52 years in the OSR group. The survival rates in the 2 groups are shown in Fig. 3. In all patients, the early more favorable outcome of EVAR was reversed within approximately 2.5 years (Fig. 3A). In patients with unruptured AAA, OSR showed a lower all-cause mortality rate than EVAR, beginning shortly after the operation (Fig. 3B), with a lower long-term all-cause mortality rate in the OSR than in the EVAR group (Table 3). Postoperative mortality within 3 months in all patients was significantly higher in the OSR than in the EVAR group (adjusted HR, 1.91; 95% CI, 1.68–2.16; P < 0.001) (Table 3), but did not differ significantly in patients with unruptured AAA (adjusted HR, 1.19; 95% CI, 0.98–1.43; P = 0.074) (Table 4). Mortality after 3 months was significantly lower in the OSR than in the EVAR group, both in all patients (adjusted HR, 0.81; 95% CI, 0.74–0.88; P < 0.001) and in patients with unruptured AAA (adjusted HR, 0.86; 95% CI, 0.79–0.93; P < 0.001). The incidence rate of reintervention was 1.75 in the EVAR and 0.52 in the OSR group, with the risk of reintervention being significantly lower in the OSR group than in the EVAR group (adjusted HR, 0.33; 95% CI, 0.25–0.43; P < 0.001). In patients who did not undergo regular dialysis, the dialysis rate was 1.93 in the EVAR and 1.49 in the OSR group, with the risk of dialysis not differing significantly in the 2 groups (adjusted HR, 0.91; 95% CI, 0.77–1.09; P = 0.310). At later times, however, OSR showed more favorable outcomes (adjusted HR, 0.86; 95% CI, 0.79–0.93; P < 0.001) (Table 4). Long-term outcome in patients with ruptured AAA is summarized in Supplementary Table 2.
Procedural cost
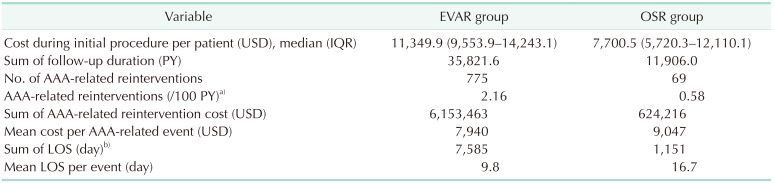
The median length of stay during the initial procedure was 11 days in the EVAR group and 17 days in the OSR group, and the median costs were US dollar (USD) 11,349.9 and USD 7,700.5, respectively (Table 5). Of the patients in the EVAR and OSR groups, the number of AAA-related events during the follow-up was 775 in the EVAR group and 69 in the OSR group, respectively. The rate of AAA-related reinterventions per 100 PY was higher in the EVAR group than in the OSR group (2.16 vs. 0.58). The mean payment for AAA-related reinterventions per event was lower (USD 7,940.0 vs. USD 9,046.6), whereas the total financial burden of AAA treatment was higher (USD 6,153,463 vs. USD 624,216), in the EVAR than in the OSR group.
DISCUSSION
Many studies to date have evaluated the socioeconomic burden of AAA, as determined by postoperative outcomes, mortality rates, and related costs, in Western countries. Less is known, however, about these burdens in Asian populations. The present study analyzed the perioperative and long-term outcomes of AAA treatments in Korean patients over a 10-year period using a national database. The main findings of this study were that the annual numbers of EVAR and OSR treatments for AAA have increased over time and that the early survival benefit of EVAR compared with OSR disappeared after approximately 2.5 years. In addition, the reintervention rate was significantly higher in the EVAR group, with the total cost in this group being 10 times higher than that in the OSR group, despite the cost per reintervention being higher in the OSR group.
Screening programs for AAA have not yet been implemented in Korea; thus, the precise prevalence of AAA has not been determined. Indirect evidence based on annual trends in the number of operations has shown that the number of patients undergoing EVAR and OSR in Korea has increased 3.1-fold from 2009 to 2018. Although it is unknown whether the actual prevalence is increasing or whether these numbers do not yet reflect a decrease in prevalence, findings showing that the number of procedures has decreased in countries with reduced incidence indicate that the prevalence of AAA is still increasing in Korea [5]. Interestingly, the number of OSR procedures remained relatively constant during the 10-year study period.
The present study found that the perioperative mortality rate was higher in the EVAR and lower in the OSR group than in previous studies [267]. This may have been due to a higher percentage of patients with high surgical risk undergoing EVAR in the present cohort. Several randomized controlled trials have suggested that, although EVAR is associated with higher short-term survival outcomes, it is not associated with greater long-term survival [489]. The short-term benefits of EVAR were found to disappear after 1 to 5 years [101112], with no significant differences in long-term mortality rates between the 2 treatments [813]. In our cohort, the benefits of EVAR disappeared in all patients at 2.5 years and in patients with unruptured AAA within 1 year. The EVAR group in the present study included a higher percentage of patients with underlying diseases, suggesting that selecting surgically higher-risk patients for EVAR mitigated its perioperative survival benefit. Therefore, outside of controlled trial settings, the surgical risk is also an important factor in determining treatment options, in addition to anatomical suitability, and it may obscure the advantages of EVAR.
The present study found that the cost of the initial procedure was much lower than in previous studies [1415], with the overall in-hospital costs for the initial procedure being similar in the EVAR and OSR groups. This was likely due to the provisions of the Korean insurance system, in which the cost of an open surgical procedure is unreasonably lower than that of endovascular treatment based on procedure time. The initial procedure costs of OSR and EVAR for AAA repair in Korea were USD 1,387 and USD 1,284, respectively. A previous study based on the Korean population reported, however, that the in-hospital cost of EVAR in patients aged <70 years was more than twice that of OSR [16], suggesting that the similar in-hospital cost in the 2 groups was likely due to the increased cost of treatment of patients aged >70 years. During the study period, AAA-related reinterventions per 100 PY were more than 3-fold higher in the EVAR group, even after adjusting for the reduction in reintervention rate due to the higher early mortality rate of the OSR group and between-group differences in follow-up periods. Thus, the total financial burden of reintervention was more than 9 times higher in the EVAR than in the OSR group. Although OSR was also associated with a lower reintervention rate, the mean payment for AAA-related reinterventions per event was higher in the OSR group than that in the EVAR group. Clinical situations requiring reinterventions in patients who underwent OSR were likely more serious or complex despite the lower reintervention rate. By contrast, previous studies showed no significant differences in disease-related expenditures between patients who underwent EVAR and OSR [1417].
The limitations of this study are associated with its observational nature based on administrative datasets, which are subject to potential coding errors and lack anatomical details. Nevertheless, the strength of this study is its use of the NHIS database. The NHIS is a national system with detailed clinical information; thus, the present study was a nationwide analysis that included a large pool of subjects. Furthermore, the follow-up duration was long. Additionally, as this study targeted only Korean patients, novel data were generated for this particular ethnic group, allowing comparisons with other groups. Data were properly adjusted, allowing comparisons of long-term outcomes by calculating the competing risks from periprocedural mortality and PY at risk.
While EVAR may offer certain advantages over OSR for AAA treatment, it is associated with higher long-term mortality rates and a significantly higher AAA-related reintervention rate and financial burden under the medical expense system in Korea. Therefore, the choice of treatment modality should be carefully considered based on individual patient factors and available resources.
 XML Download
XML Download