

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer is a common disease among older adults; more than 50% of colorectal cancer patients are aged over 65 years [12]. Major morbidity and mortality is seen in 8.7% of patients undergoing surgery for colorectal cancer, and 31.6% have minor complications [3]. This high complication rate is due to the high proportion of older patients [45]. Additionally, frailty is also common in older patients and is associated with adverse perioperative outcomes [6]; such patients undergoing colorectal surgery show worse postoperative morbidity and mortality and prolonged length of stay (LOS) in hospitals than non-frail patients [7].
Although frailty results from an inevitable age-related decline in function and retention across multiple physiological systems, several attempts have been made to improve frailty in patients undergoing colorectal cancer surgery and, consequently, improve postoperative outcomes [8]. Prehabilitation is one such attempt to improve physical activity and postoperative outcomes in patients with frailty undergoing colorectal cancer surgery [910].
Several clinical trials have been conducted to determine whether prehabilitation positively affects prognosis, including physical function, in patients with frailty undergoing colorectal surgery [11121314151617]. However, the results of these studies were conflicting. Therefore, we conducted a meta-analysis to investigate the impact of preoperative prehabilitation on the functional outcomes and postoperative complications in patients with frailty undergoing surgery for colorectal cancer.
METHODS
This study was approved by the Institutional Review Board of Yeungnam University Medical Center (No. 2022-12-028).
Search strategy
This meta-analysis was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The meta-analysis protocol was registered on the International Platform for Registered Systematic Reviews and Meta-analysis Protocols (registration No. INPLASY2022110105). Relevant articles published until November 9, 2022, were systematically retrieved using PubMed, EMBASE, Cochrane Library, and Scopus databases. The following “PICO (Population/Patient, Intervention, Comparison, and Outcome)” question guided the search strategy: “In patients with frailty who received colorectal cancer surgery, compared with no prehabilitation, does prehabilitation positively improve physical function and reduce postoperative complications and LOS in the hospital?” The search was conducted in each database using established search terms (Supplementary Material 1).
Study selection
The selection criteria for this meta-analysis were as follows: studies on patients of age 18 years or above, with a diagnosis of colorectal cancer, with frailty, and with receipt of colorectal cancer surgery; with data on 6-minute walk test (6MWT), the incidence of complications (Clavien-Dindo classification [CD] IIIa or above) after surgery, comprehensive complication index (CCI), or LOS in the hospital to measure the hospitalization outcomes; randomized and non-randomized trials comparing the effects of prehabilitation with no prehabilitation; and studies written in English. The 6MWT measures the 6-minute walking distance in meters [18]. This test is used to assess functional exercise capacity [1819]. The CCI is a continuous scale that measures surgical morbidity according to the sum of all complications weighted for their severity [20]. Review articles, case reports, letters, and studies with insufficient data or results were excluded. Two independent reviewers excluded articles after reading the titles and abstracts. Full-text assessments were conducted to exclude articles not fulfilling the inclusion criteria. The reviewers resolved any disagreements through consensus. If necessary, a third reviewer assisted in resolving disagreements.
Data extraction
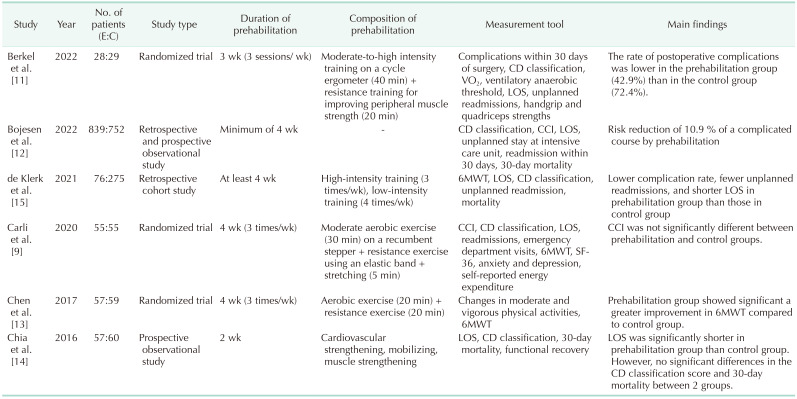
Three reviewers (MCC, YJC, and SK) independently extracted all the data using a standard data collection form. To perform a meta-analysis, if the specified outcome variables were unavailable or incomplete in the selected articles, the corresponding authors were contacted to verify the original data. The following data were collected from each eligible article: name of the first author, year of publication, number of patients, composition of prehabilitation, duration of prehabilitation, follow-up period, clinical evaluation tools, and results (6MWT, incidence of complications [CD IIIa or above], CCI, and LOS in a hospital).
Quality assessment
The quality assessment and level of evidence for each study were established according to the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) methodology. Bias evaluation for each randomized controlled trial (RCT) was performed using version 2 of the Cochrane risk-of-bias tool for randomized trials, which consists of 7 categories: random sequence generation, allocation sequence concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other biases. The assessed bias was defined as “low risk,” “high risk,” or “unclear risk.” To evaluate the methodological quality of the non-randomized trials, the Newcastle-Ottawa Quality Assessment Scale was used with the following categories: selection of subjects, comparability of groups, and assessment of outcomes. The quality of each non-randomized trial was graded as low (0–3 points), moderate (4–6 points), or high (7–9 points). These assessments were performed by 3 independent reviewers (MCC, YJC, and SK), and all disagreements were resolved through discussion.
Statistical analyses
All statistical analyses of the pooled data were performed using RevMan software (version 5.3; http://tech.cochrane.org/revman). I2 statistics were used to assess the heterogeneity between studies by measuring the extent of inconsistency among the results. Significant heterogeneity was present if I2 was greater than or equal to 50%, and a random-effects model was used for data analysis. Pooled data were considered homogenous if I2 was less than 50%, and a fixed-effects model was used for data analysis. Three RCTs and 3 non-RCTs were included in this meta-analysis. Structural differences exist between RCTs and non-RCTs, and because these differences can cause heterogeneity in the meta-analysis, this problem was resolved through subgroup analysis.
Continuous variables, including the 6MWT, CCI, and LOS in the hospital, were analyzed, and the outcomes are presented as standard mean differences (SMDs) and 95% confidence intervals (CIs). For the meta-analysis of 6MWT, the changes in the results of this test, from the values prior to prehabilitation to the values on follow-up after surgery, were used. Follow-up time points were classified as before and 1–4 weeks after surgery. If there were several measurements of the 6MWT within the same timeframe, the outcomes recorded during the last follow-up were used in the meta-analysis. To evaluate the differences in the incidence of complications between the prehabilitation and non-prehabilitation groups, we classified complications according to CD. A CD grade greater than or equal to IIIa was considered a complication. The incidence of complications was analyzed using odds ratios (OR) and 95% CI. In our meta-analysis, statistical significance was set at P < 0.05.
A funnel plot was visually assessed to evaluate publication bias, and Egger test was performed using R software ver. 4.1.2 (R Foundation for Statistical Computing). The funnel plot determined the publication bias of individual studies based on pooled estimates. Egger test determined whether the funnel plot was symmetrical, and a P-value of less than 0.05 indicated the possibility of publication bias.
RESULTS
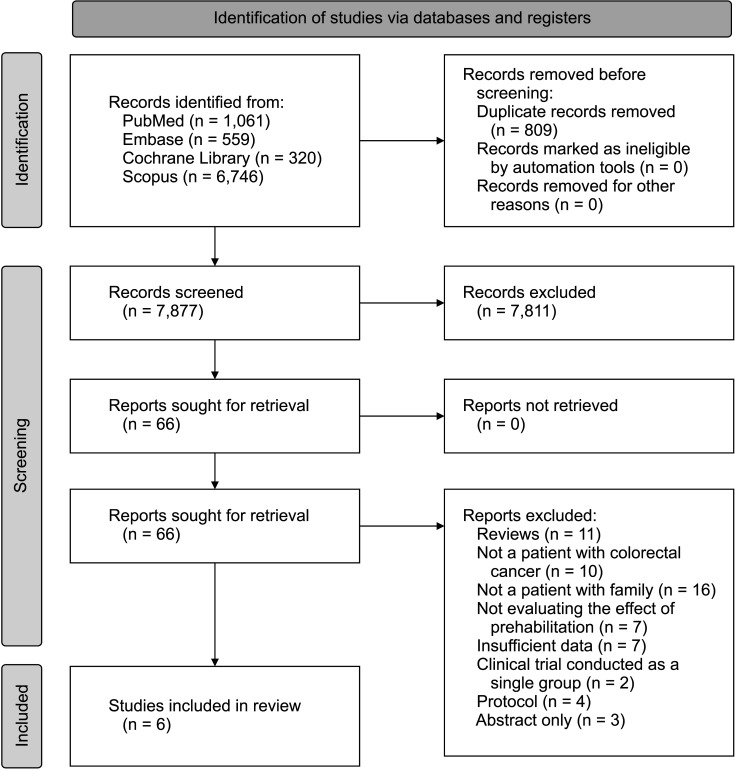
A total of 8,686 articles were identified using the search terms. Of these, 809 duplicates were excluded from further analysis. After reading the titles and abstracts, 7,811 articles were excluded because they did not meet the inclusion criteria. The remaining 66 articles were then assessed for eligibility. Sixty articles were excluded for the following reasons: 11 were reviews, 10 did not involve patients with colorectal cancer, 16 did not involve patients with frailty, 7 did not evaluate the effect of prehabilitation, 7 had insufficient data, 2 were conducted with a single group, 4 were protocols, and 3 were only abstracts. Finally, 6 studies (3 randomized and 3 non-randomized trials) were included in this meta-analysis (Fig. 1). The characteristics of the included studies are summarized in Table 1 [91112131415].
Results of the meta-analysis
In the pooled analysis for changes in the results of the 6MWT before and 1–4 weeks after surgery, compared with those of the control group, there were no significant improvements in the prehabilitation group at either point in time (before surgery: I2 of 99%, random-effects model, SMD of 2.25, 95% CI of –1.96 to 6.47, P = 0.29; 1–4 weeks after surgery: fixed-effects model, SMD of 0.36, 95% CI of –0.12 to 0.84, P = 0.15) (Fig. 2A, B).
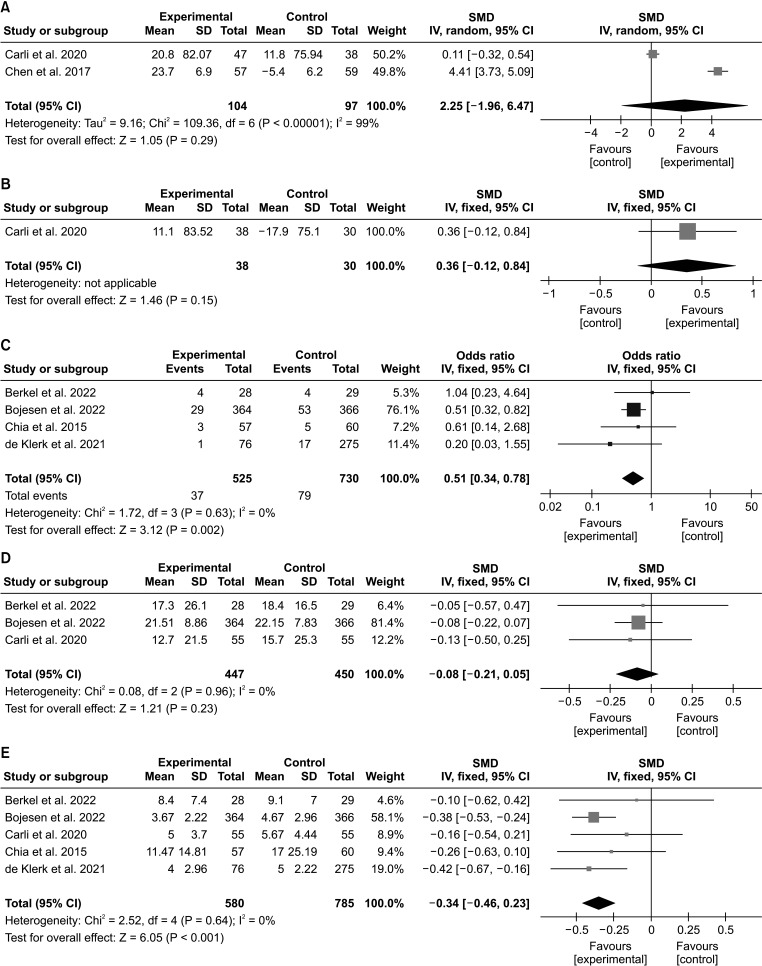
Fig. 2
Forest plot showing the results of meta-analysis combining randomized and non-randomized controlled trials. Results of (A) 6-minute walk test (6MWT) before surgery, (B) 6 MWT 1–4 weeks after surgery, (C) postoperative incidence of complications (Clavien-Dindo grade ≥IIIa), (D) comprehensive complication index, and (E) length of hospital stay. SD, standard deviation; CI, confidence interval; SMD, standard mean difference.
![]()
A fixed-effects model was used for the pooled analysis of the postoperative incidence of complications (I2 of 0%). The incidence of complications was significantly lower in the prehabilitation group than that in the control group (OR, 0.51; 95% CI, 0.34–0.78; P = 0.002) (Fig. 2C). In addition, the fixed-effects model was used for the pooled analysis of CCI because the I2 value was 0%. CCI results were not significantly different between the 2 groups (SMD, –0.08; 95% CI, –0.21 to 0.05; P = 0.23) (Fig. 2D).
The fixed-effects model was also used for the pooled analysis of LOS in a hospital because the I2 value was 0%. Our meta-analysis showed that LOS in a hospital was shorter in the prehabilitation group than that in the control group (SMD, –0.34; 95% CI, –0.46 to 0.26; P < 0.001) (Fig. 2E).
Results of meta-analysis for randomized control trials
In the pooled analysis for changes in the results of 6 MWT at follow-up before and at 1–4 weeks after surgery, compared with those of the control group, there were no significant improvements in the prehabilitation group at either point in time (before surgery: I2 of 99%, random-effects model, SMD of 2.25, 95% CI of –1.96 to 6.47, P = 0.29; 1–4 weeks after surgery: fixed-effects model, SMD of 0.36, 95% CI of –0.12 to 0.84, P = 0.15) (Fig. 3A, B).
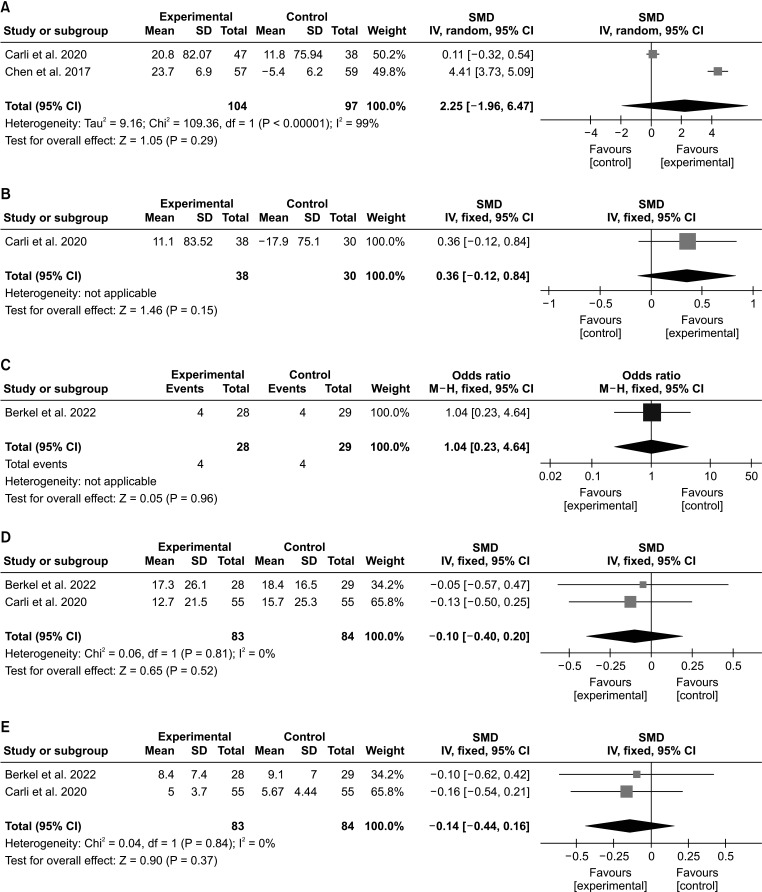
Fig. 3
Forest plot presenting the results of the meta-analysis for randomized controlled trials. Results of (A) 6-minute walk test (6MWT) before surgery, (B) 6MWT 1–4 weeks after surgery, (C) postoperative incidence of complication (Clavien-Dindo grade ≥IIIa), (D) comprehensive complication index, and (E) length of hospital stay. SD, standard deviation; CI, confidence interval; SMD, standard mean difference.
![]()
A fixed-effects model was used for the pooled analysis of the postoperative incidence of complications (I2, not applicable). The incidence of complications was not significantly lower in the prehabilitation group compared with that in the control group (OR, 1.04; 95% CI, 0.23–4.64; P = 0.96) (Fig. 3C). In addition, a fixed-effects model was used for the pooled analysis of CCI because the I2 value was 0%. CCI results were not significantly different between the 2 groups (SMD, –0.10; 95% CI, –0.40 to 0.20; P = 0.52) (Fig. 3D).
A fixed-effects model was also used for the pooled analysis of LOS in a hospital because the I2 value was 0%. The LOS in a hospital was not significantly different between the prehabilitation group and the control group (SMD, –0.14; 95% CI, –0.44 to 0.16; P = 0.37) (Fig. 3E).
Results of meta-analysis for non-randomized control trials
A fixed-effects model was used for the pooled analysis of the postoperative incidence of complications because the I2 value was 0%. The incidence of complications was significantly lower in the prehabilitation group than that in the control group (OR, 0.48; 95% CI, 0.31–0.75; P = 0.001) (Fig. 4A). In addition, a fixed-effects model was used for the pooled analysis of CCI (I2, not applicable). CCI results were not significantly different between the 2 groups (SMD, –0.08; 95% CI, –0.22 to 0.07; P = 0.30) (Fig. 4B).
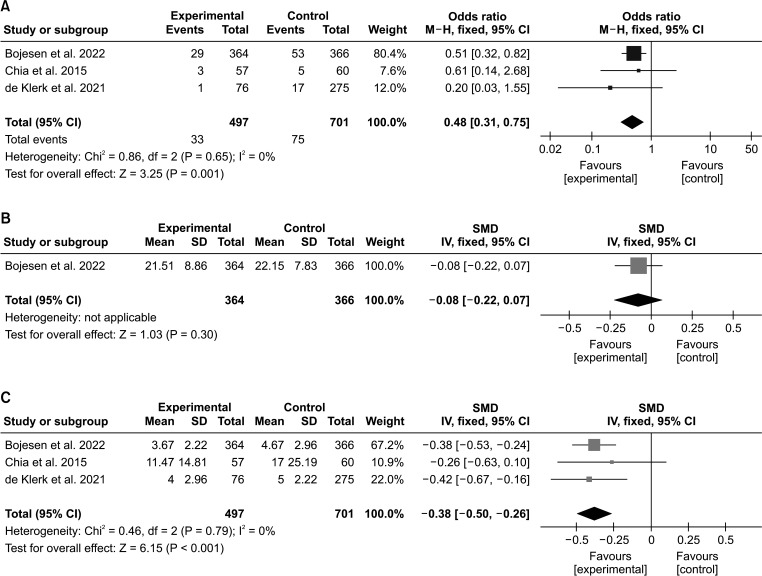
Fig. 4
Forest plot showing the results of the meta-analysis for non-randomized controlled trials. (A) Postoperative incidence of complication (Clavien-Dindo classification ≥IIIa), (B) comprehensive complication index, and (C) length of hospital stay. CI, confidence interval; SD, standard deviation; SMD, standard mean difference.
![]()
Since the I2 value was 0%, a fixed-effects model was used for the pooled analysis of LOS in a hospital. The meta-analysis showed that LOS in a hospital was shorter in the prehabilitation group than that in the control group (SMD, –0.38; 95% CI, –0.50 to 0.26; P < 0.001) (Fig. 4C).
Assessment of study quality
The risk of bias for all selected studies is shown in Tables 2 and 3. Of the 3 randomized trials, none had a low risk of bias in the blinding of participants and personnel. Chen et al.’s study [13] had an unclear risk of bias in random sequence generation, allocation concealment, and blinding of outcome assessment and a low risk of bias in incomplete outcome data, selective reporting, and other biases. In the studies by Carli et al. [9] and Berkel et al. [11], other than the blinding of participants and personnel, all other domains were assessed to have a low risk of bias. Of the 21 domains across all the randomized trials, 15 had a low risk of bias. All 3 non-RCTs [121415] were rated as 8-star studies and considered high quality.


Publication bias
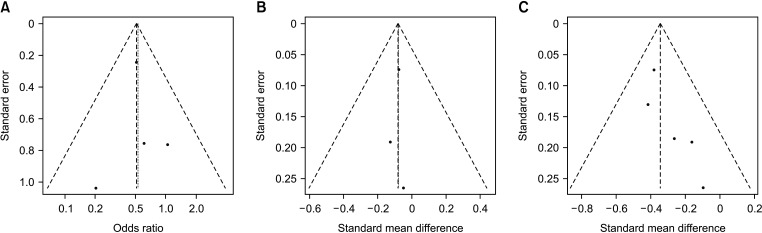
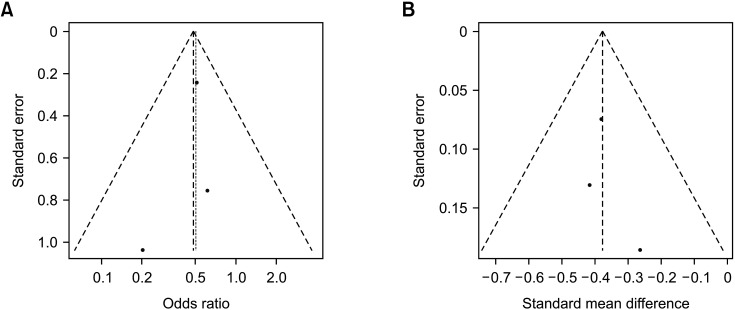
Funnel plots did not show significant asymmetry in intergroup comparisons of the OR for the incidence of complications, CCI, and LOS in the hospital (Fig. 5). Furthermore, the P-values of Egger test were greater than 0.05, indicating the incidence of complications (incidence of complications [CD ≥IIIa], P = 0.652; CCI, P = 0.828; and LOS, P = 0.079). The funnel plots did not show significant asymmetry in the intergroup comparisons of the OR for the incidence of complications and LOS in non-RCT studies (Fig. 6). Furthermore, the P-value of Egger test was >0.05, indicating the incidence of complications (incidence of complications [CD ≥IIIa], P = 0.828; LOS, P = 0.628).
DISCUSSION
In our meta-analysis, we investigated the effect of prehabilitation on improving physical activity and postoperative outcomes in patients with frailty undergoing colorectal cancer surgery. The incidence of postoperative complications (CD ≥IIIa) and LOS in a hospital were significantly less and shorter, respectively, in patients who received prehabilitation, compared to those in patients in the control group. However, no significant differences were observed between the prehabilitation and control groups in the 6MWT and CCI scores.
Frailty is associated with poor postoperative outcomes. Patients with frailty who underwent colorectal surgery showed a higher overall incidence of complications, postoperative mortality, longer LOS in hospitals, and higher numbers of admissions to nursing homes or rehabilitation centers [616]. Frailty was an independent risk factor for a higher overall incidence of complications and admission to nursing homes and rehabilitation centers [16]. In our meta-analysis, we found that prehabilitation may reduce the incidence of postoperative complications and LOS in hospitals after surgery for colorectal cancer in patients with frailty. Accordingly, clinicians should consider conducting or recommending prehabilitation in patients with frailty who have colorectal cancer before they undergo colorectal surgery for better clinical outcomes. Based on the prehabilitation programs implemented in the studies included in this meta-analysis, it is suggested that following a prehabilitation program can significantly improve postoperative outcomes for colorectal cancer. The prehabilitation program may consist of a customized exercise program supervised by experts, such as exercise kinesiologists and physiotherapists, or home-based aerobic and resistance training programs. Exercise performed for 30–40 minutes per session at least 2–3 times per week can lead to favorable outcomes. Nutritional guidelines to ensure adequate protein and energy intake may also be considered. Other components of prehabilitation can include correction of anemia, pharmacotherapy, smoking and alcohol cessation support, and physical fitness testing to evaluate progress. The components and goals of prehabilitation can vary depending on the patient’s condition but generally include education, cardiovascular strengthening, muscle strengthening, and attention to nutrition. The prehabilitation period should be at least 4 weeks, depending on the surgery date.
Furthermore, the effectiveness of prehabilitation has been demonstrated in several previous studies. These studies have reported that preoperative exercise training in patients undergoing major surgery improves their physical fitness and reduces postoperative pulmonary complications [17]. The group that experienced prehabilitation had significantly fewer postoperative complications compared with control group [1115]. Additionally, postoperative medical complications were significantly lower; 13.2% in the prehabilitation group and 26.5% in the control group [15]. These positive effects of preoperative exercise training may have contributed to fewer complications and shorter LOS in hospitals in the prehabilitation group.
The 6MWT is useful for evaluating physical capacity. This test is performed by walking as far as possible in 6 minutes over a flat distance of at least 30 meters [21]. The standardized 6MWT yields reproducible and reliable results about physical capacity [22]. The 6WMT is primarily used for functional capacity in patients with pulmonary disease, but it can also be used in non-pulmonary conditions. It was useful for measuring the physical capacity of patients undergoing abdominal surgery [23] and was a valuable predictor of postoperative complications and LOS in patients undergoing major surgery [24]. Some studies showed improvements in the 6MWT by prehabilitation in the form of exercise in patients who underwent cancer surgery [25].
CD and CCI are formal scales used to objectively assess postoperative complications [2026]. CD is a simple and widely used method for assessing postoperative complications in several surgeries [2728]. CD comprises several grades. However, the reclassification of the results was different for each included study; therefore, only CD grades IIIa or above were considered in our study.
CCI expresses postoperative complications on a continuous scale by summing all complications and weighting their severity [20]. CCI sensitively reflects the effect of treatment and shows strong associations with either single or multiple complications [2029]. CD was more likely to have minor complications masked by a higher CD grade, whereas CCI was a better predictor of postoperative outcomes [30]. In our study, considering these differences, CD and CCI were analyzed to determine the effect of prehabilitation on postoperative complications.
However, our meta-analysis found that the functional capacity measured by 6MWT and CCI was not improved after prehabilitation. We believe that the intensity or degree of prehabilitation conducted in previous studies was insufficient to improve physical performance in patients with frailty who have colorectal cancer. To confirm whether prehabilitation helps improve the functional capacity of such patients, the effect of prehabilitation should be evaluated with various exercise intensities and durations. CCI is the sum of all complications weighted by severity [18]. We believe that CCI might not be a sensitive enough indicator to reflect the differences between the prehabilitation and control groups.
Additionally, when we analyzed the pooled data by separating RCTs and non-RCTs, meta-analysis for RCTs showed that prehabilitation had no significant positive effect on physical activity and the incidence of postoperative complications (CD ≥IIIa), CCI, and LOS in the hospital. However, meta-analysis for RCTs revealed that postoperative complications and LOS in the hospital were significantly reduced in patients who received prehabilitation. Because RCTs have a higher level of evidence than non-RCTs, the reliability of our results may be considered low. However, since the number of RCTs used in our meta-analysis was low, caution is required in the interpretation of our results. Our study had some limitations. First, a relatively small number of studies was included in the meta-analysis. Second, the definition of frailty was heterogeneous. Third, each study used different prehabilitation protocols. Additionally, there is no consensus on the diagnostic criteria for frailty in patients with cancer nor a standardized prehabilitation protocol. The most appropriate diagnostic and prehabilitation protocols for patients with frailty who have colorectal cancer should be elucidated through further research. Therefore, well-designed clinical trials are required to overcome these limitations.
In conclusion, we found that prehabilitation can be helpful in reducing postoperative complications and shortening LOS in hospitals for patients with frailty who underwent colorectal cancer surgery. Therefore, our results suggest that clinicians should consider conducting or recommending prehabilitation exercises prior to colorectal surgery in patients with frailty.
 XML Download
XML Download