

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer (CRC) is the third most common cancer (10%) with the second highest mortality rate (9.4%) worldwide [1]. In 2019, CRC was indicated as the fourth most common cancer in Korean men and women [2]. The incidence of early-stage CRC increased from 5.8% in the late 1990s to 8.9% in the early 2000s [34]. Increased diagnosis of early-stage CRC may also be attributed to medical screening, such as colonoscopy [23]. The 5-year cancer-specific survival for TNM stage I CRC is over 90% [5]. As TNM stage I CRC has a low recurrence rate, few studies have evaluated the risk factors for its recurrence.
According to the National Comprehensive Cancer Network (NCCN) guidelines, surgical resection is the primary treatment for TNM stage I CRC. In most cases, a segmental resection of the colon or rectum is performed to achieve negative surgical margins. Adjuvant chemotherapy is not typically recommended for stage I CRC due to the low risk of recurrence [6]. However, subgroups of patients with stage I CRC at higher risk of recurrence, such as those with lymphovascular invasion or poorly differentiated tumors [7], may benefit from adjuvant chemotherapy. Several studies have investigated the role of surveillance after surgical resection of stage I CRC. The NCCN recommends regular surveillance with colonoscopy every 3–5 years for patients with stage I CRC, as well as regular monitoring of CEA levels [6]. In addition to surgical resection, lifestyle modifications, such as maintaining a healthy weight, engaging in regular physical activity, and consuming a balanced diet rich in fruits, vegetables, and whole grains, may help reduce the risk of recurrence and improve overall survival in patients with early-stage CRC [8].
This study investigated the rate and risk factors of TNM stage I CRC recurrence following surgical resection. In addition, we evaluated the prognosis of patients with recurrent CRC.
Go to : 
METHODS
Patient database
This study was approved by the Institutional Review Board of Konkuk University Medical Center (No. 2022-08-041) and the need for informed consent was waived. We retrospectively reviewed the patient database to identify patients diagnosed with TNM stage I CRC following colon or rectal cancer surgery. In total, 841 patients underwent CRC resection between November 2008 and December 2014. Eleven patients treated with neoadjuvant therapy were excluded, thereby excluding most patients with lower rectal cancer. Nine patients underwent transanal excision (TAE) for rectal cancer were excluded. Risk factors for recurrence were compared between the colon cancer, rectal cancer, and CRC groups.
Surgical treatment
All patients underwent curative surgery, including right or left hemicolectomy or anterior resection for colon cancer, lower anterior resection or abdominoperineal resection (APR) for rectal cancer. Colon surgery was performed via open surgery or hand-assisted laparoscopic surgery. If there were positive or transected margins, or unfavorable histologic features after endoscopic resection of the malignant polyp, additional surgery was performed. Tumor lesions were classified as colon or rectal cancer based on operation record descriptions.
Surveillance
All patients were followed up at 6-month intervals during the first 2 years after surgery, and at 12-month intervals for up to 5 years after surgery. Follow-up evaluations included a physical examination, serum CEA, abdominopelvic and chest CT, and colonoscopy within 12 months after surgery. The mean follow-up was 65 months (median, 66 months; range, 1–121 months).
Statistical analyses
Disease-free survival (DFS) was defined as the time from surgery until diagnosed recurrence by imaging or death. DFS for patients who survived with no recurrence until the end of the follow-up period was defined as the time from surgery until the last follow-up visit. Data were analyzed using the IBM SPSS Statistics ver. 28.0 (IBM Corp.). The Student t-test and the chi-square test were used to compare recurrent and nonrecurrent groups. DFS rates were calculated using the Kaplan-Meier curve and compared using the log-rank test. We could not use Cox analysis for overall survival as the coefficients did not converge due to low death rates. A P-value of <0.05 was considered statistically significant.
Go to :
RESULTS
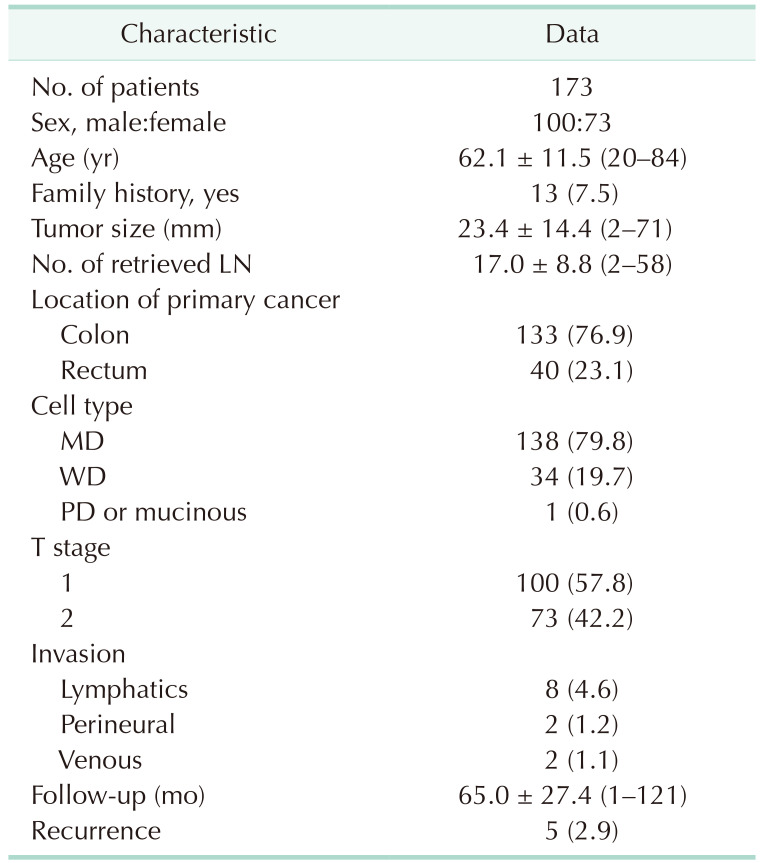
Of the 841 patients who underwent CRC resection, 193 patients were diagnosed with pathologic TNM stage I colon or rectal cancer between November 2008 and December 2014. Eleven patients received preoperative chemoradiotherapy and 9 patients underwent TAE for rectal cancer and were therefore excluded from this study. The remaining 173 patients were included in this study, of which 133 had colon cancer and 40 had rectal cancer; 100 were male and 73 were female, with a mean age of 62 years (range, 20–84 years). The 173 patients underwent curative resection, including 28 laparoscopic surgeries, and 145 open surgeries with D2 lymph node dissection as they exhibited early-stage cancer lesions. In 128 cases, primary curative resection was achieved, whereas 45 cases required additional curative resection after primary endoscopic resection. Tumor diameters in patients requiring additional curative resection were smaller than those in patients who achieved primary curative resection (mean diameter 12.0 mm and 27.4 mm, respectively; P < 0.001).
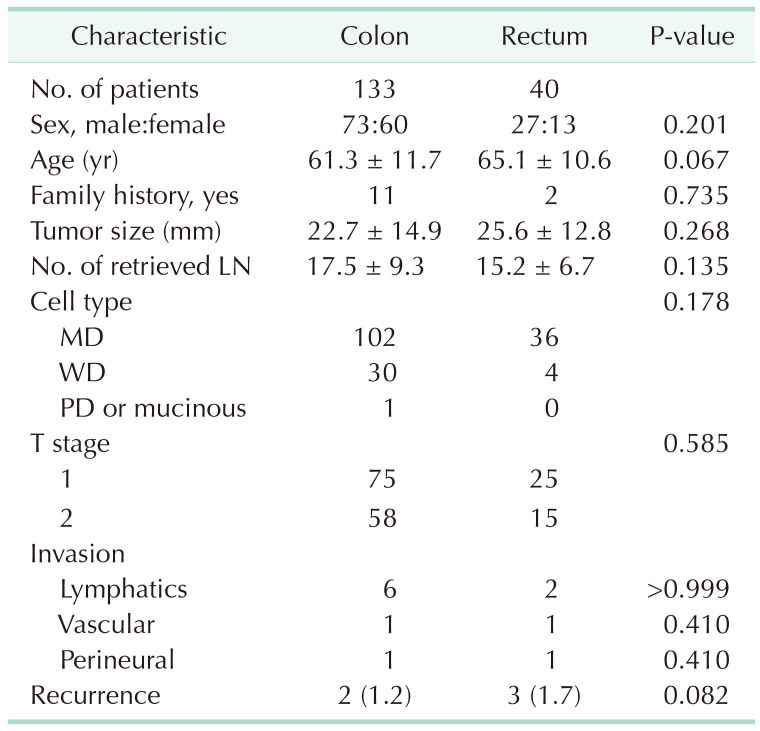
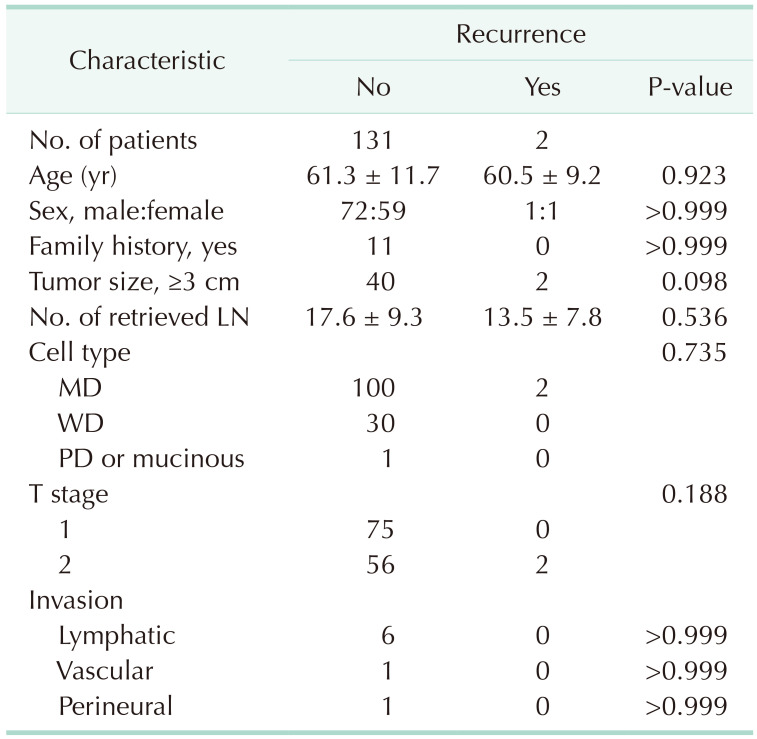
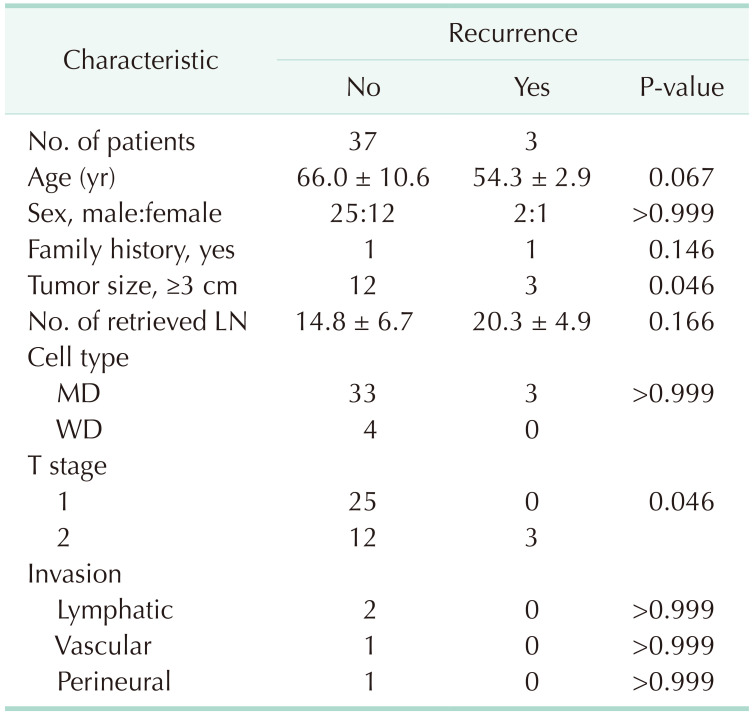
The median follow-up period was 66 months. The recurrence rate for CRC was 2.9% (Table 1). Based on clinical characteristics, tumor size (P = 0.030) and T stage (P = 0.012) were related to CRC recurrence (Table 2). Tumor size (≥3 cm vs. <3 cm) and T stage were identified as prognostic factors for DFS (P < 0.001 and P = 0.007, respectively) (Fig. 1). Evaluation of the clinical characteristics of the CRC, colon, and rectal cancer groups revealed no significant risk factors for recurrence (Tables 3, 4). However, for patients with colon cancer, evaluation of the DFS curve revealed that tumor size (≥3 cm vs. <3 cm) is a risk factor for recurrence (P = 0.035), whereas T stage is not a recurrence risk factor (P = 0.102) (Fig. 2). In patients with rectal cancer, evaluation of the DFS curve revealed that both tumor size (P= 0.014) and T stage (P = 0.014) are risk factors for recurrence (Table 5; Fig. 3).
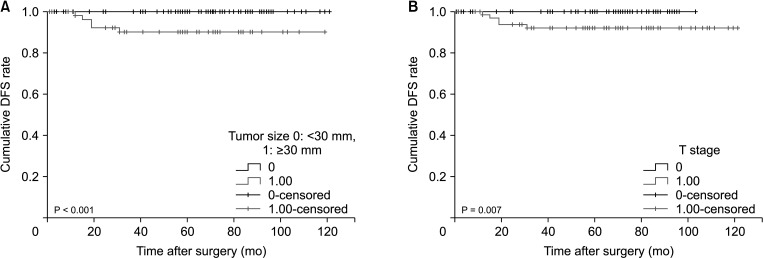 | Fig. 1The disease-free survival (DFS) rate in colorectal cancer according to the tumor size (A) and T stage (B).
|
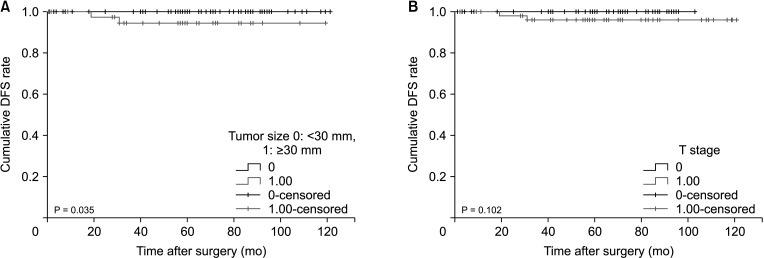 | Fig. 2The disease-free survival (DFS) rate in colon cancer according to the tumor size (A) and T stage (B).
|
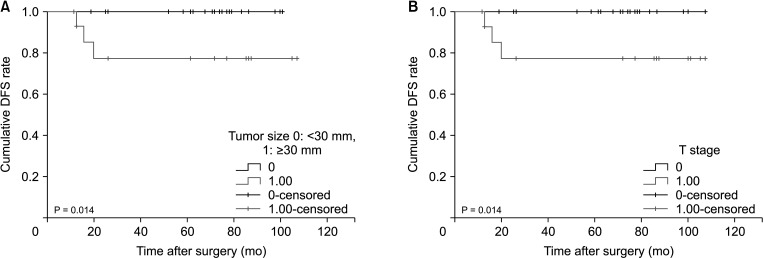 | Fig. 3The disease-free survival (DFS) rate in rectal cancer according to the tumor size (A) and T stage (B).
|
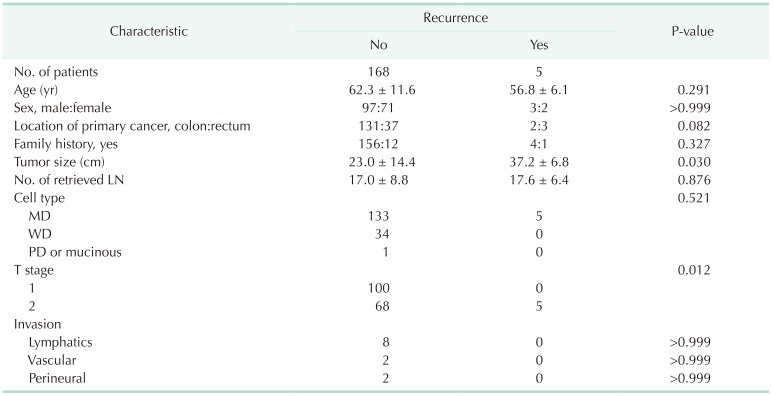
Of the 173 patients, CRC recurred in 5 patients. Three patients were diagnosed with rectal cancer, while 2 were diagnosed with rectosigmoid junction cancer. One systemic lymph node recurrence, 1 local recurrence, and 3 pulmonary metastases occurred within 3 years. These patients underwent total mesorectal excision. All patients with recurrence exhibited T2 stage and a tumor size of ≥3 cm. The distance from the anal verge to the primary tumor site was at least 9 cm (Table 6).

Two patients with rectal cancer recurrence underwent received chemoradiotherapy and 1 underwent APR. The 3 patients with pulmonary metastases without metastasis to other organs underwent pulmonary wedge resection and received chemotherapy. Disease progression was observed in only 1 patients. Three patients exhibited no evidence of disease during the follow-up period of this study. One patient with systemic lymph node metastasis maintained stable disease status during the follow-up period of this study.
Go to :
DISCUSSION
Early CRC recurrence is rare, with reported recurrence rates of 2.4%–4.6% in early-stage CRC [9101112]. Leijssen et al. [13] reported recurrence rates of 2.3% and 4.7% for TNM stage I colon and rectal cancer, respectively. Without preoperative combined chemotherapy and radiation therapy (CCRT), the recurrence rate for rectal cancer was 7% [14]. Rectal cancer recurrence rates following TAE range from 1.8% to 14.1%. In this study, the recurrence rates for CRC, colon cancer, and rectal cancer were 2.9%, 1.2%, and 1.7%, respectively.
In this study, we found that tumor size and T stage are risk factors for TNM stage I colorectal and rectal cancer recurrence, but not for colon cancer recurrence. Previous studies also reported T stage as a risk factor for colorectal [91115] and rectal cancer recurrence [131617]. Peng et al. [18] reported that in patients with rectal cancer, radical resection is recommended to prevent local recurrence if the tumor diameter is greater than 2.5 cm. Although several studies reported lymphovascular and perineural invasion as risk factors for CRC recurrence [121315192021], we did not observe an association between lymphovascular and perineural invasion and CRC recurrence.
Patients with early rectal cancer located on the lower rectum were not included in this study as patients who received neoadjuvant therapy for lower rectal cancer were excluded. All patients included in this study therefore had a tumor location of at least 9 cm from the anal verge. Of the relapsed patients, 1 patient had a primary tumor located 15 cm from the anal verge and 4 patients had primary tumors located 9 cm from the anal verge (Table 6).
Of the relapsed patients, 3 developed pulmonary metastases and 2 developed local recurrence. The 3 patients who had pulmonary metastases underwent pulmonary wedge resection for metastatic lung lesions and chemotherapy and exhibited a stable disease status after aggressive treatment. Of the 2 patients with local recurrence, 1 underwent CCRT and was subsequently stable. The other patient received APR and palliative chemotherapy but died due to progressive disease with pulmonary metastasis, suggesting that aggressive treatment should be recommended for patients with recurrent stage I CRC. The interval for recurrence in this study was 3 years, which corresponds to previous reports [2223].
This study had some limitations, including the potential for selection bias in the patient recruitment process as the study relied on data from a single center, and a small size, which may limit the generalizability of the results. In addition, the study was conducted retrospectively, which may have resulted in incomplete or inconsistent data collection. Furthermore, as the study only evaluated patients who underwent surgery for TNM stage I CRC, the findings may not apply to patients with different disease stages or who receive different treatment modalities. Additionally, the study was unable to compare overall survival and cancer-specific survival, which may be important outcomes to evaluate in future studies.
In conclusion, although the recurrence rate of TNM stage I CRC is low, tumor size and T stage are risk factor for recurrence, and patients with recurrent disease may benefit from aggressive therapy.
Go to :
 XML Download
XML Download