

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Significant advancements in large language model (LLM) technology have recently revolutionized the field of artificial intelligence (AI), with ChatGPT released by OpenAI in November 2022 standing out as a prime example [1]. ChatGPT has exhibited exceptional performance in evaluating knowledge related to fields such as medicine, law, and management, which have traditionally been considered to be the domain of experts. Notably, the system achieved high accuracy on the United States Medical Licensing Examination, the Bar exam, and the Wharton MBA final exam, even without fine-tuning the pretrained model [2345].
Surgical education and training demand a significant investment of time, with the process involving a combination of didactic learning, hands-on training, and supervised clinical experience [6]. During residency, surgical trainees work alongside experienced surgeons, gaining practical experience in patient care, surgery, and clinical decision-making. Additionally, trainees engage in a series of didactic courses and conferences covering the principles of surgery, medical knowledge, and surgical techniques. Due to the comprehensive nature of surgical education and training, it can take more than a decade to become a skilled and competent surgeon. Given the time-intensive nature of surgical education and training, it is important to explore how emerging technologies, such as AI and LLMs, can augment the learning process [7].
This study aims to employ ChatGPT to evaluate the general surgery board exam in Korea and assess whether LLMs possess expert-level knowledge. Moreover, the study compared the performance of GPT-3.5 and GPT-4. By exploring the potential of LLMs in the context of surgical education and training, this study seeks to provide a foundation for future research on how these advancements can be effectively integrated into clinical education and practice, ultimately benefiting surgical residents, and practicing surgeons.
Go to : 
METHODS
The study did not involve human subjects and did not require Institutional Review Board approval.
General surgery board exam of Korea
The goal of surgical education and training is to develop the ability to actively evaluate the pathological conditions of surgical diseases and to acquire the surgical skills to treat traumatic, congenital, acquired, neoplastic, and infectious surgical diseases. To quantitatively evaluate this knowledge and skill set of surgical residents, a board certification exam is required after completion of their training, in order to become a board-certified general surgeon in Korea. The exam is composed of 2 parts: the first part is a 200-question multiple-choice test, and those who pass the first part are eligible to take the second part. The second part consists of questions based on high-resolution clinical images and surgical video clips. The questions are created and supervised by the Korean Surgical Society and the Korean Academy of Medical Science (KAMS).
Dataset for model testing
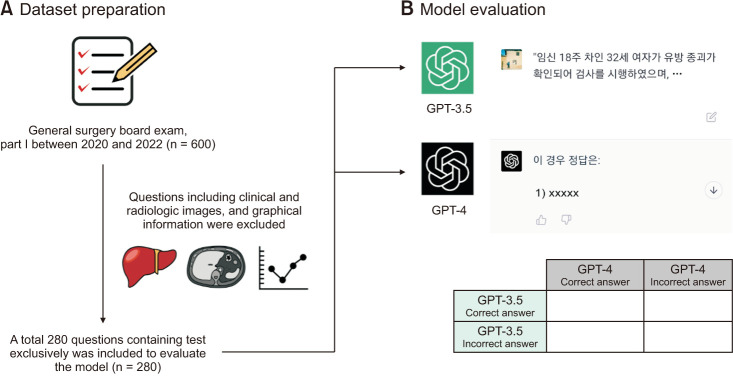
The actual board exam questions are held by KAMS, but due to limited access to the usage of these questions, we constructed our dataset by gathering questions recalled by examinees who took the actual exam. As the LLM cannot process visual information such as clinical images, radiology, and graphs, questions that included visual information were excluded from our dataset. All problems were manually inputted in their original Korean text. Finally, our dataset included a total of 280 questions from the first stage of the board exam in 2020, 2021, and 2022 (Fig. 1A).
Large language model and performance evaluation
In this study, we utilized the ChatGPT generative pretrained transformer (GPT) language model developed by OpenAI to evaluate its performance on a dataset of questions. We performed model testing using both GPT-3.5 and GPT-4, with the former conducted from March 1 to March 3, 2023, and the latter scheduled for March 15, 2023. To evaluate the model’s performance, we manually entered the questions into the ChatGPT website and compared the answers provided by the model to those provided by examinees (Fig. 1B).
Statistical analysis
This study compared the performance of the GPT-3.5 and GPT-4 models with the McNemar test. A P-value less than 0.05 would indicate a statistically significant difference between the performance of the GPT-3.5 and GPT-4 (IBM SPSS Statistics ver. 27; IBM Corp.).
Go to :
RESULTS
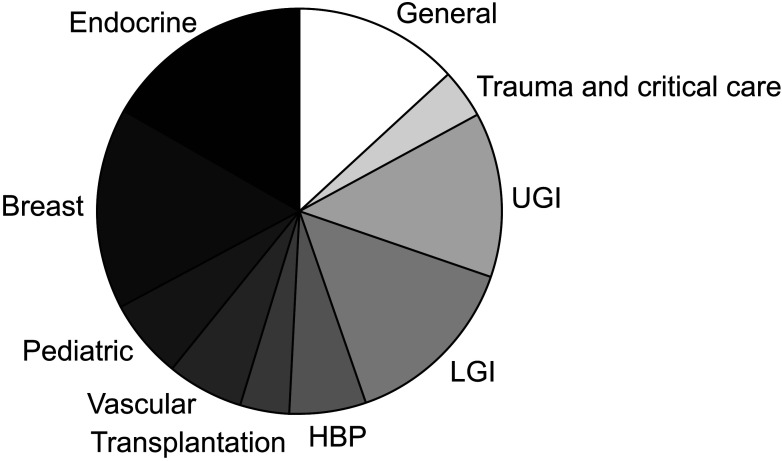
The dataset used for model evaluation consisted of a total of 280 questions, which were classified into subspecialties and listed in order of frequency as follows: endocrine (16.8%), breast (16.1%), lower gastrointestinal (LGI, 14.3%), upper gastrointestinal (UGI, 13.2%), general (13.2%), pediatric (6.4%), hepatobiliary and pancreas (HBP, 6.1%), vascular (6.1%), transplantation (4.0%), and trauma and critical care (4.0%) (Fig. 2).
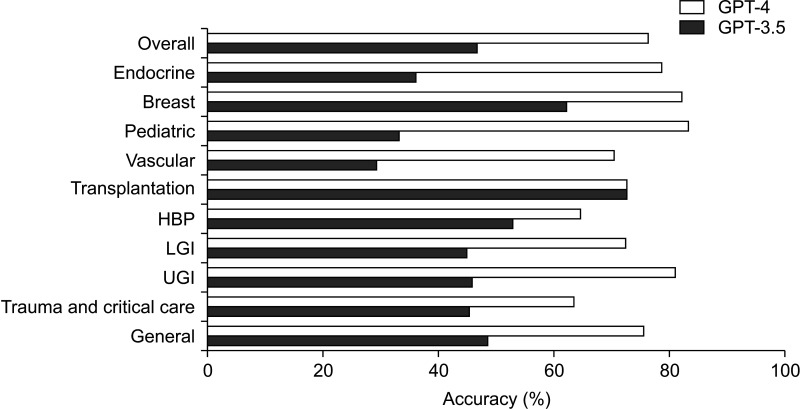
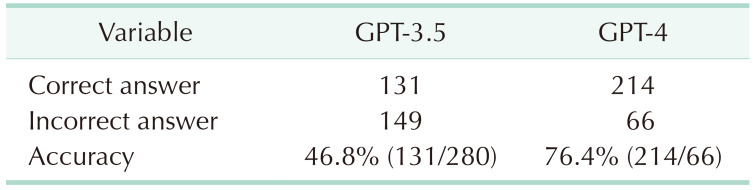
A significant difference in performance was observed between the GPT-3.5 and GPT-4 models (P < 0.001). The GPT-3.5 model achieved an overall accuracy of 46.8%, providing correct answers for 131 out of the 280 questions (Table 1). In terms of individual subspecialties, the model's accuracy rates were as follows (sorted from highest to lowest): transplantation (72.7%), breast (62.2%), HBP (52.9%), general (48.6%), UGI (45.9%), trauma and critical care (45.5%), LGI (45.0%), endocrine (36.2%), pediatric (33.3%), and vascular (29.4%). In contrast, the GPT-4 model demonstrated a substantial improvement in overall accuracy, attaining a rate of 76.4% by providing correct answers for 214 out of the 280 questions. The accuracy rates for each subspecialty were as follows: pediatric (83.3%), breast (82.2%), UGI (81.1%), endocrine (78.7%), general (75.7%), transplantation (72.7%), LGI (72.5%), vascular (70.6%), HBP (64.7%), and trauma and critical care (63.6%) (Fig. 3).
Go to :
DISCUSSION
The primary objective of this study was to conduct a quantitative assessment of ChatGPT's ability to comprehend complex surgical clinical information and to explore the potential implications of LLM technology for surgical education and training. Specifically, we tested the performance of ChatGPT using questions from the Korean general surgery board exam and observed that the model achieved an accuracy of 76.4% with GPT-4 and 46.8% with GPT-3.5. Remarkably, this accuracy was achieved without fine-tuning the model and by using prompts in the Korean language exclusively, thus highlighting the significance of our findings.
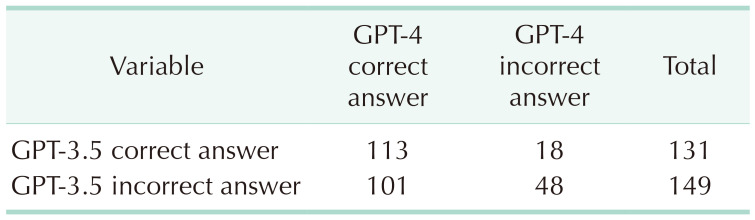
The comparative analysis revealed a notable improvement in GPT-4’s performance compared to GPT-3.5 model across all subspecialties. GPT-4 not only exhibited a higher overall accuracy rate but also demonstrated more consistent performance in each subspecialty, with accuracy rates ranging from 63.6% to 83.3%. However, for 18 questions, GPT-3.5 provided the correct answer while GPT-4 did not (Table 2). It is unclear why GPT-4 gave incorrect answers for these questions despite the overall increase in accuracy. Pinpointing the exact reason for this discrepancy is challenging. Differences in training data, model architecture, or other factors could have contributed to the variation in the performance between the 2 versions.
The authors kindly recommend that the surgeon’s society proactively adapts and utilizes these technological advancements to enhance patient safety and improve the quality of surgical care. In the context of surgical education, it is crucial to transition from the traditional rote learning approach to a method that emphasizes problem definition in specific clinical situations and the acquisition of relevant clinical information for problem resolution. LLMs serve as generative AI models, providing answers to given problems. Consequently, the quality of the answers relies on the questions posed [8]. Surgeons must conduct thorough history-taking and physical examinations to accurately define the problems they face. By providing LLMs with comprehensive summaries of patients' chief complaints, present illnesses, and physical examinations, the models have the potential to assist in decision-making regarding diagnostic tests and treatment options in certain clinical situations. However, it is essential for medical professionals to remember that LLMs should not replace the fundamentals of patient care, which include maintaining close connections with patients and actively listening to their concerns [9].
Moreover, active surgeons who completed their training over a decade ago may find LLMs helpful for continuous medical education (CME). Accessing new knowledge may be challenging for them due to the time elapsed since their training, potentially leading to outdated management practices. While numerous surgical societies offer CME programs, altering ingrained routines in clinical practice can be difficult. By utilizing an up-to-date LLM as a supplementary resource in their decision-making process, surgeons may have additional means to stay informed and strive for evidence-based care in their patient management [10].
In medicine, decision-making has a profound impact on patient safety, demanding a higher level of accuracy and a conservative approach to change compared to other fields. Although GPT-4 achieved a 76.4% accuracy rate on the Korean surgical board exam, it is important to remember that LLMs are generative models, often referred to as “stochastic parrots” [11]. Instead of providing strictly accurate information, they generate responses based on the probability of the most appropriate words given the data they have been trained on. Consequently, the current level of accuracy is not yet sufficient for immediate clinical application in patient care.
However, it is noteworthy that a service released less than 6 months ago exhibits such remarkable performance, and ChatGPT is only one example of LLMs. Recently, Microsoft released BioGPT, an LLM trained on PubMed literature, and Meta introduced LLaMA, an LLM with an accessible application programming interface (API) for open innovation and fine-tuning [1213]. Based on these trends, we can anticipate future LLMs to be trained on an even larger and more diverse set of medical information, providing specialized knowledge in the medical field. In addition, the GPT-4 framework itself is capable of processing and analyzing visual information, including images and videos [14]. This capability raises the possibility that, in the future, the performance of GPT-4 could be evaluated on datasets containing clinical photos and surgical videos. Such advancements would further enhance the applicability of GPT-4 in surgical fields, broadening its utility beyond text-based tasks and offering a more comprehensive understanding of complex clinical scenarios assisting professionals in their decision-making processes and contributing to improved patient care.
The limitations of this study include the fact that the dataset was compiled using questions recalled by examinees, which may not accurately represent the full set of actual board exam questions due to restricted access. Another limitation is the exclusion of visual information. Since the models used in the study are unable to process visual information, such as clinical images, radiology, and graphs, questions containing visual components were excluded from the dataset. As a result, we cannot determine whether ChatGPT would pass or fail the board exam based on these limitations. Despite these constraints, this study holds significance as it confirms the ability of LLMs to analyze surgical clinical information and make appropriate clinical decisions.
In conclusion, ChatGPT, particularly GPT-4, demonstrates a remarkable ability to understand complex surgical clinical information, achieving an accuracy rate of 76.4% on the Korean general surgery board exam. However, it is important to recognize the limitations of LLMs and ensure that they are used in conjunction with human expertise and judgment.
Go to :
 XML Download
XML Download