

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Burnout is prevalent in various human service occupations and professional healthcare services [1]. It is particularly widespread among surgical trainees at the frontlines of clinical healthcare. A United States national survey showed that surgical trainees reported the following symptoms: 69%, burnout; 57%, emotional exhaustion; 50%, depersonalization; and 16%, reduced personal accomplishment [2]. According to research conducted in Korea [3], medical trainees reported emotional exhaustion (54.2%), depersonalization (62.5%), and reduced personal accomplishment (33.3%). A growing concern is that burnout in physicians is linked to negative consequences, including physical, psychological, and occupational problems.
Research is currently being conducted on the effects of burnout on physicians, examining variables such as stress-related health, anxiety, depression, alcohol abuse, suicidal thoughts, reduced productivity, absenteeism, high turnover, and increased medical errors [456]. Moreover, due to the coronavirus disease 2019 pandemic, healthcare professionals have suffered increased fatigue and consequent burnout symptoms [78]. These symptoms negatively affect the professionalism and well-being of physicians and the quality of their patient care.
Consequently, the prevention and alleviation of burnout is an urgent issue in the medical field. Studies have found that enhanced resilience is an important protective factor against burnout [9]. Resilience is defined as an individual’s ability to recover quickly from adverse or stressful situations [10]. It is characterized by mindfulness, coping skills, optimism, and empathy, and is inversely related to burnout risk [25]. Various strategies have been implemented to promote individual resilience in healthcare communities, including mindfulness-based interventions, professional resilience coaching, and enhanced stress resilience training [1112].
Self-compassion is a helpful resource among healthcare professionals to enhance resilience and coping skills when confronted with challenges and common stressors [13]. According to Neff and Germer [14], self-compassion is defined as treating one’s personal limitations and shortcomings with warmth and kindness; the acknowledgment of shared human experiences, including experiences of pain, imperfections, and difficulties (regarded in this study as common humanity); and a clear and balanced awareness of the experience of suffering in the present. Research has demonstrated that self-compassionate medical trainees and residents have the potential advantage of being confident in their ability to provide calm and compassionate care to themselves and others [15]. Furthermore, physicians with higher levels of self-compassion have reported better work engagement, reduced emotional exhaustion, and increased life satisfaction [16]. Therefore, a prerequisite for psychological well-being and compassionate care is that the healthcare professional acknowledges and accepts their difficulties and possesses self-compassion.
The Self-Compassion for Healthcare Communities (SCHC) program is a brief version of the Mindful Self-Compassion (MSC) program traditionally used in healthcare settings [13]. Due to the fatigue experienced by physicians, the SCHC program is useful as a practical self-compassion intervention. This study aims to investigate the feasibility and efficacy of the SCHC program in decreasing the prevalence of burnout and improving resilience in a sample of Korean surgical trainees.
Go to : 
METHODS
Setting and participants
The Institutional Review Board in Seoul National University Bundang Hospital approved the study (No. B-2007-624-304). Subsequently, surgical trainees were recruited from a tertiary referral academic hospital in Seongnam, Korea. The research team facilitated this through flyers, advertising the SCHC program from August 15 to 30, 2021. Inclusion criteria for participation were (1) being employed as a surgical trainee, doctor-resident, or fellow; (2) having no previous experience regarding meditation; and (3) having no known mental disorders. The preferred sample size was 20 students. All participants provided informed consent before completing the preintervention survey. The study protocol was registered as NCT04857567 on clinicaltrial.gov before participant enrollment.
Design
The study used a 1-group pretest–posttest design without a control group. The SCHC program was conducted every Thursday and Friday for 6 weeks between September and October 2021. A total of 10 participants were assigned to each session, and those who could not participate on their assigned day were allowed to participate on other available days. Three supplementary sessions were conducted on Saturdays for those unable to participate during the week. These sessions were held according to the trainees’ work, which often included unplanned overtime and late surgeries. Participants attended weekly live online sessions via Zoom for 1 hour from 7:30 to 8:30 PM. The participation rate for all the sessions was 87.8% (session 1, 86.7%; session 2, 93.3%; session 3, 86.7%; session 4, 100%; session 5, 66.7%; and session 6, 93.3%). A certified MSC teacher trainer, Y.S., and an MSC-trained teacher, H.S, led the intervention.
At the beginning of each session, participants were allocated time to share the contents of the last session’s practice as an informal meditation exercise. This was followed by the instructors presenting a daily topic and guiding participants through 1 or 2 targeted exercises. Thereafter, the research team sent a reminder e-mail to encourage the participants to practice the sessions’ learnings in their daily lives.
Each session of the SCHC program concentrated on a specific topic: In session 1, participants were provided an overview of the program, and concepts such as self-compassion and the misunderstandings thereof (e.g., self-compassion as a form of self-pity) were presented. Session 2 introduced self-compassion exercises, such as supportive touch, and mindfulness practices, including mindful breathing and being aware of physical sensations. Session 3 focused on how to change unwanted behavior using kindness instead of self-criticism. Session 4 taught methods to manage intractable emotions, such as labeling emotions and being aware of them throughout the day. Session 5 explored caregiving fatigue and burnout and highlighted the importance of understanding one’s limitations in resolving others’ pain through “compassion with equanimity.” Session 6 encouraged the participants to know their core values as caregivers and instructed them on how to continue the practices included throughout the course [17].
Measures
Participants completed the baseline and first posttest online, 1 week before and after the program, respectively. A second posttest was conducted as a 1-month follow-up. In these assessments, burnout was measured using the 22-item Maslach Burnout Inventory-Human Services Scale [18], which contains 3 subscales: emotional exhaustion, depersonalization, and reduced personal accomplishment. Responses were provided on a seven-point scale ranging from 0 (almost never) to 6 (almost always). The total burnout scores on each of the 3 subscales were divided into high, moderate, or low levels based on the cutoffs for the 3 subscales of burnout (emotional exhaustion: low, ≤18; moderate, 19–26; and high, ≥27 / depersonalization: low, ≤5; moderate, 6–9; and high: ≥10 / reduced personal accomplishment: low, ≥34; moderate, 29–33; and high, 28) [2], and presented in the results section.
Self-compassion was measured using the 26-item Self-Compassion Scale [19], which contains 6 subscales: self-kindness, self-judgment, common humanity, isolation, mindfulness, and over-identification. Responses were provided on a 5-point scale ranging from 1 (almost never) to 5 (almost always).
Life satisfaction was measured using the 5-item Satisfaction with Life Scale [20]. Responses were provided on a seven-point scale ranging from 1 (almost never) to 7 (almost always).
Depression, anxiety, and stress were measured using the short version of the Depression Anxiety Stress Scale (DASS-21) [21]. This tool examines the respondent’s symptoms experienced over the past week on a scale of 0 (never) to 3 (almost always). Subscale items were summated for a total score in each category. The total depression, anxiety, and stress scores were stratified into normal, mild, moderate, severe, and extremely severe levels per the standards of the DASS-21. Total depression, anxiety, and stress scores were categorized into normal, mild, moderate, severe, and extremely severe levels according to the standard of the DASS scale (depression: normal, 0–9; mild, 10–13; moderate: 14–20; and severe, 21–27; extremely severe, ≥28 / anxiety: normal, 0–7; mild, 8–9; moderate, 10–14; severe, 15–19; and extremely severe, ≥20 / stress: normal, 0–14; mild, 15–18; moderate, 19–25; severe, 26–33; and extremely severe, ≥34), and presented in the results section.
Resilience was measured using the 27-item Resilience Scale, which contains 3 subscales: control, positivity, and sociality [22]. Responses were provided using a 5-point rating scale, ranging from 1 (almost never) to 5 (almost always).
Data analysis
Participants who attended at least 4 of the 6 sessions and had completed all pre- and posttests were included in the final data analysis set (n = 15). The power of normality was satisfied for all variables except common humanity in the pretest and self-kindness in the first posttest as less than 30 samples were used to conduct the Shapiro-Wilk tests. The characteristics of the participants are presented as descriptive statistics. A series of repeated measures analysis of variances (RMANOVAs) were conducted under sphericity conditions to confirm any significant changes in the study variables between the pre- and posttests. Friedman tests, the nonparametric alternative to RMANOVA, were conducted for 2 study variables, common humanity and self-kindness, due to nonnormal distributions. The post hoc tests using Bonferroni correction were conducted to compare changes between the pretest and both posttests. The following analyses were conducted to examine whether changes in self-compassion predicted changes in the outcome variables: first, to create standardized difference scores, postscores were regressed on prescores, and B scores estimated from the regression were subtracted from postscores and standardized. Second, the standardized difference scores were used to conduct linear regressions.
All statistical tests were 2-sided; the P-value of <0.05 indicated a statistically significant difference. We used IBM SPSS Statistics ver. 23.0 (IBM Corp.) to analyze all the data.
Go to :
RESULTS
Participants
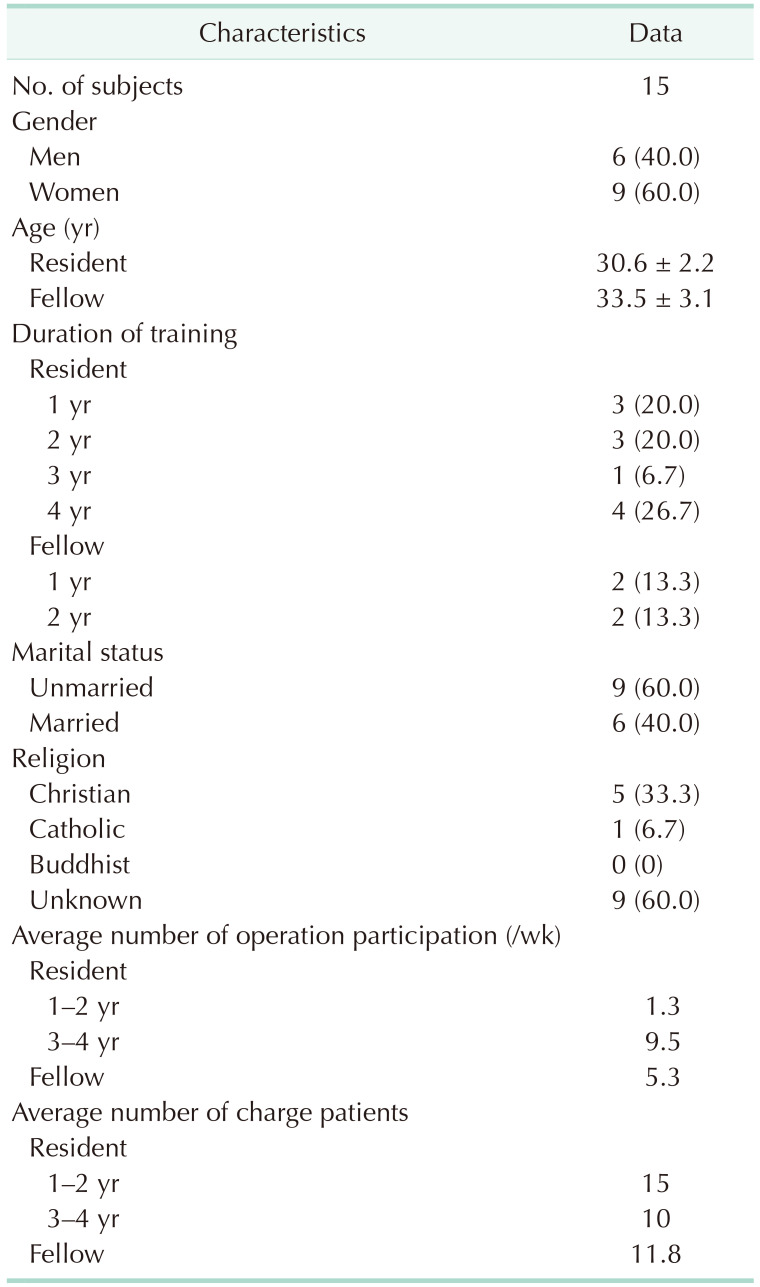
Among the 15 participants, there were 11 residents and 4 fellows. Participants’ response rate remained at 100% at the pre- and posttests and at the follow-up survey. The general characteristics of the participants are displayed in Table 1.
Burnout
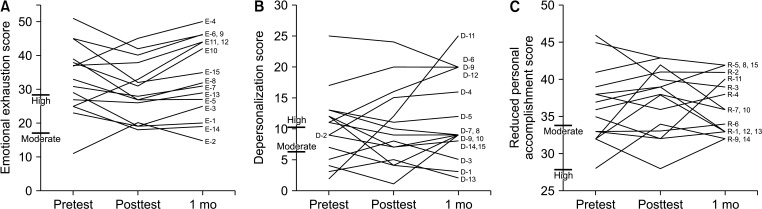
Burnout variables of the pretest were used to categorize participants into levels: 11 participants (73.3%), high emotional exhaustion level (score range, 27–51); 8 participants (53.3%), high depersonalization level (score range, 11–25); and 1 participant (6.7%), high reduced personal accomplishment level (score, ≥28). Fig. 1 presents the burnout pattern changes of all the participants before and after the SCHC program. In the posttest, high emotional exhaustion and depersonalization rates decreased by 6.6% (1 participant), while personal accomplishment rates increased by 6.7% (1 participant). In the 1-month follow-up test, high depersonalization and high reduced individual accomplishment rates decreased by 6.7% (1 participant) compared with the posttest.
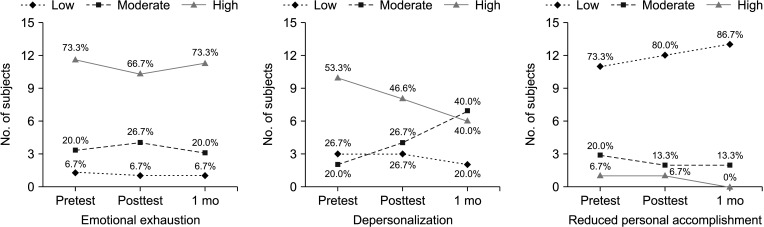 | Fig. 1Burnout rates of pretest, posttest, and 1-month follow-up: 3 dimensions. The cutoffs for 3 subscales of burnout are as follows: emotional exhaustion: low, 18; moderate: 19–26; and high, ≥27 / depersonalization: low, 5; moderate, 6–9; and high, ≥10 / reduced personal accomplishment: low, ≥34; moderate, 29–33; and high, 28. The total score of reduced personal accomplishment used the total score of personal accomplishment without reverse.
|
Depression, anxiety, and stress
In the pretest, all participants reported normal to moderate levels of depression (score range, 0–20); 12 experienced normal to moderate levels of anxiety (score range, 0–14), and 3 reported severe to extremely severe anxiety (score range, 16–20) (Fig. 2). Further, 10 participants experienced normal to moderate stress levels (score range, 0–18), and 5 reported severe to extremely severe stress (score range, 26–30). After participating in the SCHC program, 8 of 15 participants (53.3%) showed relief from anxiety or maintenance of anxiety levels, and 9 (60.0%) were relieved of stress or maintained their stress levels. Further, 3 participants (20.0%), who were categorized with extremely severe or severe anxiety, showed mild to moderate remission in anxiety levels in the posttest following the intervention, and 5 participants (33.3%) with extremely severe or severe stress levels were relieved in the posttest. Fig. 3 depicts changes in anxiety and stress in all participants following the SCHC program intervention.
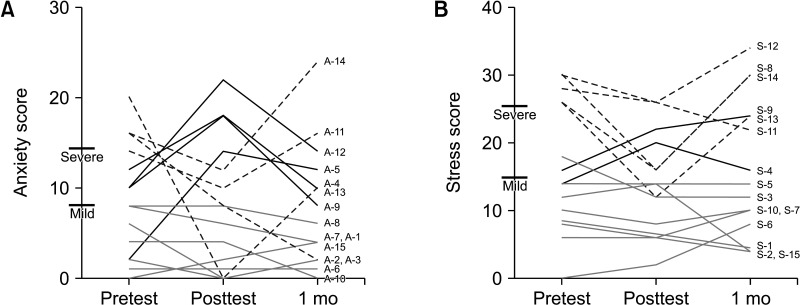 | Fig. 2Transition of anxiety (A) and stress (B). ‘A’ and ‘S’ indicate the same participants. The light lines represent participants who showed reduced and maintained anxiety or stress levels. The dotted lines represent participants with remarkably reduced anxiety or stress levels in the posttest. The bold lines show participants whose anxiety or stress levels increased in the posttest but decreased at the 1-month follow-up.
|
Resilience, life satisfaction, and self-compassion
Table 2 displays the means, standard deviations, and significant changes between the pretest, posttest, and 1-month follow-up. Based on the RMANOVA and Friedman tests, significant differences between the pretest, posttest, and 1-month follow-up scores were found in control (F2,28 = 4.3, P = 0.024), total resilience (F2,28 = 5.5, P = 0.010), life satisfaction (F2,28 = 3.8, P = 0.035), and common humanity (χ2[2, n = 15] = 9.7, P = 0.008). The post hoc tests using Bonferroni correction revealed that, compared with the pretest scores, posttest scores increased in control (mean difference, 0.3; P = 0.024), total resilience (mean difference, 0.2; P = 0.019), life satisfaction mean difference, 0.6; P = 0.028), and common humanity (mean difference, 0.9; P = 0.041). However, there were no significant differences between the posttest and 1-month follow-up. Therefore, changes were maintained postintervention.
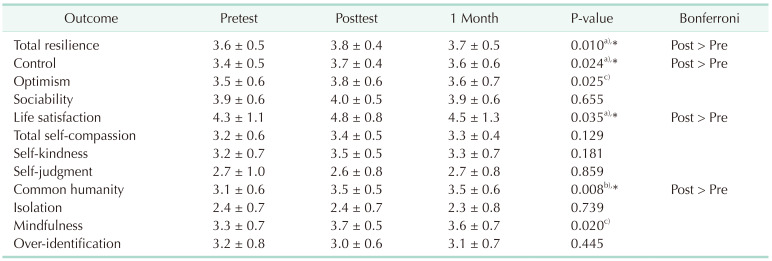
Table 2
Pretest, posttest, and 1-month follow-up scores (n = 15)
Values are presented as mean ± standard deviation.
a)By the Bonferroni adjustment for multiple comparisons. b)By the Friedman tests. c)No significant mean differences after using the Bonferroni adjustment for multiple comparisons.
*P < 0.05, mean difference compared with pretest, statistically significant at the 5% significance.
![]()
Comparison of variables between pre- and posttest
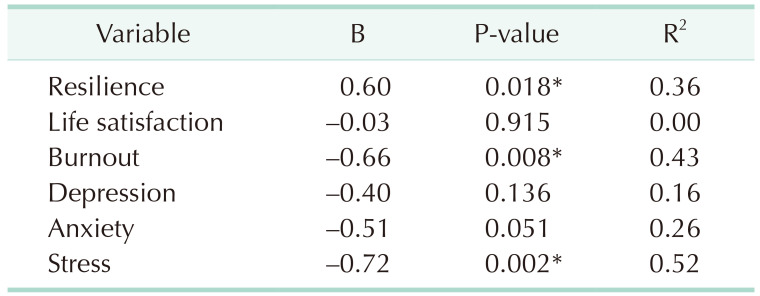
Table 3 shows that self-compassion gains significantly predicted changes in resilience, burnout, and stress. An increase in self-compassion significantly predicted greater gains in resilience (B = 0.60, R2 = 0.36, P = 0.018) and greater reductions in burnout (B = –0.66, R2 = 0.43, P = 0.008) and stress (B = –0.72, R2 = 0.52, P = 0.002).
Go to :
DISCUSSION
To the best of our knowledge, this is the first study to elucidate the feasibility and efficacy of an online SCHC program to improve resilience and decrease burnout symptoms in surgical trainees in Korea. The main results from the current study are as follows. First, we observed that after the SCHC program, the rates of high emotional exhaustion and depersonalization decreased to moderate levels, and the rate of personal accomplishment increased. Second, we found that 8 of 15 participants (53.3%) experienced relief from—or maintenance of—anxiety levels, and 9 (60.0%) were relieved of—or maintained their—stress levels. The SCHC program seemed effective for lowering mental pains, including burnout, anxiety, and stress. Third, significant differences were noted in control, 1 subscale of resilience, total resilience, life satisfaction, common humanity, and 1 subscale of self-compassion. Further, gains in self-compassion significantly predicted an increase in resilience and decrease in burnout and stress. The SCHC appeared to increase positive variables, such as resilience or life satisfaction, and decrease negative variables, such as stress.
Previous research showed that surgical trainees are directly exposed to patient pain and trauma and that 60% of trainees experience burnout. Therefore, it is important to promote surgical trainees’ mental health and well-being [23]. Studies have consistently suggested that interventions implemented to alleviate and prevent burnout in surgical trainees need to target the enhancement of their resilience [5]. This study addressed self-compassion, a coping mechanism related to personal challenges and stressors, which is known to improve resilience. Self-compassion and mindfulness of suffering are vital in treating oneself with warmth and kindness [14]. Acts of kindness by caring for oneself benefit both the giver and the receiver; although kindness is temporary, it is an appropriate strategy to increase personal well-being [23]. The most significant benefit of self-compassion training is to teach specific practices that individuals can apply in their daily lives [13]. Since stress is ongoing in healthcare work environments, the capacity to care for and support oneself in moments of anguish is a healthy coping strategy. Previous research has demonstrated that the SCHC program effectively teaches healthcare professionals to be more self-compassionate and manage occupational stress to increase their well-being and empathy and reduce fatigue and burnout [13].
Surgical trainees who participated in the SCHC program experienced burnout symptoms, such as emotional exhaustion and depersonalization, also previously reported to be high in surgery residents [2]. A longitudinal study of burnout revealed that its development progressed from emotional exhaustion to depersonalization and reduced personal accomplishment [24]. Furthermore, longitudinal results that explored the causal sequence between burnout and depression found that burnout induces depression [25]. These results suggest that the emotional exhaustion of surgical trainees is an important signal for early intervention. Moreover, the results reveal that mental health management using intervention strategies is necessary to address burnout experienced by surgical trainees. The SCHC program is particularly helpful for surgical trainees who are experiencing early burnout symptoms (e.g., emotional exhaustion or depersonalization) because it is an intervention that helps deactivate the threat defense system (fight-flight-freeze) induced in stressful situations and activate the system that instills a sense of safety. Stress and burnout conditions activate threat defense systems biologically, leading people to worry more, choose avoidance responses, and become critical of others externally, as well as become more self-judgmental and self-critical, and experience self-isolation internally, while the system activating a sense of safety helps evoke thoughts, emotions, and behaviors that promote positive links with others [26]. As a training that includes compassionate care, empathy, and warmth, the SCHC program helps activate a safety-seeking threat protection system when detecting signals that are perceived as external or internal psychological threats [13]. This self-compassionate attitude of being gentle, comforting, and tolerant suggests that emotional tension, physical exhaustion, and lack of self-affection can be alleviated. Thus, the system promoting a sense of safety can facilitate relaxed and self-calming conditions, thus helping improve resilience in the face of negative experiences, such as early emotional exhaustion and depersonalization due to burnout.
Similarly, research has reported that surgical trainees tend to be more stressed due to excessive workload and time pressure [27]. They may experience anxiety and depression due to uncertainty and pressure regarding their capacity to care for their patients’ well-being [228]. Self-compassion or mindfulness training programs can help exhausted health professionals recognize their own feelings and thoughts, accept their experiences as a universal human experiences, and be kind to themselves [1113]. These positive attitude changes lead to a clearer state of mind and to their adopting self-care strategies [19]. The SCHC relieves negative experiences, such as psychological distress, fear of failure, trauma, anxiety, and depression, and promotes positive outcomes, such as positive mental health, happiness, curiosity, optimism, resilience, and life satisfaction. Such evidence suggests that the SCHC program can be beneficial for preventing burnout and enhancing psychological well-being.
The findings of this study are significant because they demonstrate the effectiveness of the online SCHC program, unlike previous research. Prior studies of online smartphone applications or mindful training programs have not been able to verify their efficacy [2930]. In a recent study, self-compassion was found to increase through a smartphone application intervention; however, it was difficult to expect decreased burnout and perceived stress [11]. In the current study, the online SCHC program reduced burnout and increased resilience.
Despite the novel findings, some limitations of this study must be acknowledged. First, after the SCHC program intervention, significant changes were found in common humanity, a subscale of self-compassion. However, there were no significant improvements in the other subscales of self-compassion, namely self-kindness and mindfulness. These results suggest that the short-term MSC program improved skills to be cognitively aware of one’s suffering; however, it was challenging to demonstrate mindfulness and self-kindness. Continuous daily practices are required to internalize self-kindness and mindfulness. Consequently, it is necessary to complement the SCHC program to encourage and guide daily practices. Second, we used a comparatively small sample size of 15 participants without a control group, and environmental factors may have affected the results. Therefore, this study’s findings should be interpreted with caution. Third, a follow-up evaluation of 1 month was a relatively short period for assessing the SCHC program’s benefits. In future research, it will be valuable to evaluate program effects with larger number of participants based on follow-up evaluations over longer durations. In addition, the chosen setting was an environment where most surgical trainees had to manage their workload and the SCHC program due to work pressure. This intervention should be temporally supported to ensure that environmentally sound program participation is possible. However, this study provides valuable insights into the mechanism through which the online SCHC program decreases burnout and stress and promotes resilience in surgical trainees.
This study aimed to elucidate the SCHC program’s effectiveness for surgical trainees using an online platform. The online SCHC intervention was suitable for reducing anxiety, stress, and burnout in surgical trainees. Additionally, it also helped improve resilience, self-compassion, and life satisfaction. MSC is a contributing factor in strengthening resilience and alleviating or preventing burnout. Thus, it is an important resource for surgical trainees to cope with stress. Therefore, it is recommended that specific mental health programs should be included in surgical training to improve the well-being of surgical trainees.
Go to :
 XML Download
XML Download