

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Liver transplantation (LT) is widely recognized as a curative treatment for end-stage liver disease and hepatocellular carcinoma (HCC) [12]. While the demand for LT continues to increase, the disparity between supply and demand of available grafts has likewise increased [3]. To overcome the shortage of deceased donors, the use of living donor LTs (LDLTs) has become increasingly common, especially in Asia. Simultaneously, LT using safe marginal grafts has increased [45]. To support these efforts, strategies have been established for the safe use of marginal grafts including small-for-size liver grafts, old-aged donor grafts, ABO-incompatible grafts, grafts with steatosis, and virus-infected grafts.
HBV-related end-stage liver disease and HCC are the main indications for LT in East Asian areas where HBV infection is endemic, including Korea (3% prevalence in 2016) [6]. In these areas, the high prevalence of donors with HBV carrier status has made using liver grafts with inactive HBV infection necessary [7]. However, the possibility of HBV transmission or reactivation, or HCC recurrence after LT from an HBV are major issues that must be addressed. Nevertheless, attempts to use these grafts, following strict selection criteria and perioperative management protocols have continued. The current criteria include appropriate graft allocation, such that the recipient’s prognosis is unaffected [89]; perioperative medication using hepatitis B immunoglobulin (HBIG) [10]; administration of antivirals to control HBV [11]; and regular surveillance for HBV reactivation or HCC occurrence.
Several previously published retrospective and prospective studies have approved the use of HBsAg (+) grafts with caution [61213]. However, most of them were short-term retrospective studies (<5 years). Although HBV reactivation is commonly reported within 2–3 years posttransplantation, HCC occurrence needs to be monitored over a longer period, as several publications have reported HCC recurrence >5 years posttransplantation [1415].
Therefore, this study investigated the long-term safety outcomes of LT with active and chronic HBV-infected liver grafts and the prevalence of HCC recurrence after LT.
METHODS
Study population and data collection
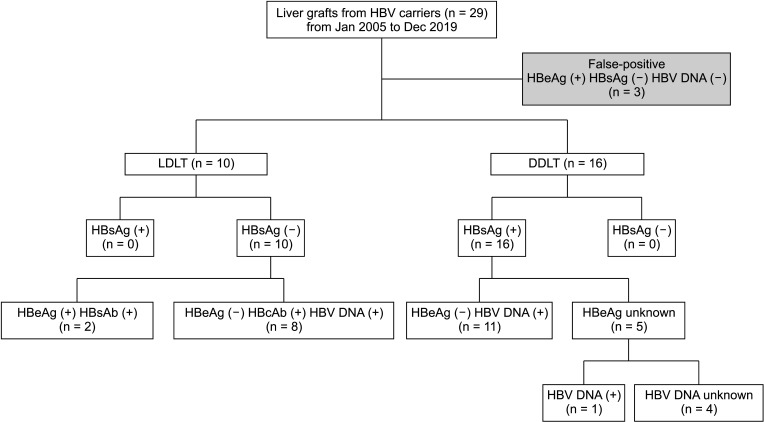
The electronic medical records of 2,260 patients who underwent LT at 3 major hospitals from January 2000 to April 2019 were retrospectively reviewed. Twenty-six patients (1.2%) who received liver grafts from donors positive for HBsAg, HBeAg, or HBV DNA were enrolled (Fig. 1). Demographics and other information about deceased donors were also collected from the Korean Network for Organ Sharing database. For LDLT donors, outpatient follow-up appointment records were reviewed to evaluate donor safety.
This study was approved by the Institutional Review Boards of each institution (No. H-2104-178-1214, No. 20-2021-17, and No. B-2108-705-403). The need for informed consent was waived by the review boards. This report complies with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) reporting guidelines for reporting observational studies.
HBV recurrence
The recurrence of HBV was defined as serum HBV DNA detection and increased HBV DNA levels after LT for HBsAg (+) recipients in whom HBsAg (+) grafts were transplanted. Positive seroconversion of HBsAg was determined in patients who underwent transplantation using HBsAg (–) grafts. We schematized the HBV infection state of recipients to investigate changes in liver graft properties after LT [16]. Donors and recipients were divided into resolved, inactive, or chronic hepatitis groups based on their serologic status (HBsAg/Ab, HBeAg/Ab, and HBV DNA titer) and serum liver enzyme levels, determined by consultation with our hepatologist [17].
Immunosuppressant regimen
Basiliximab (Simulect, Novartis) 40 mg was used on the day of the operation and postoperative day 4 as the immunosuppression induction agent. Triple therapy regimens of tacrolimus, mycophenolate mofetil, and corticosteroids were used as maintenance immunosuppressive therapy. The target serum concentration of tacrolimus was 8–12 ng/mL for the first 6 months posttransplantation, and 6–8 ng/mL beyond 6 months post-LT.
Prophylaxis for HBV recurrence
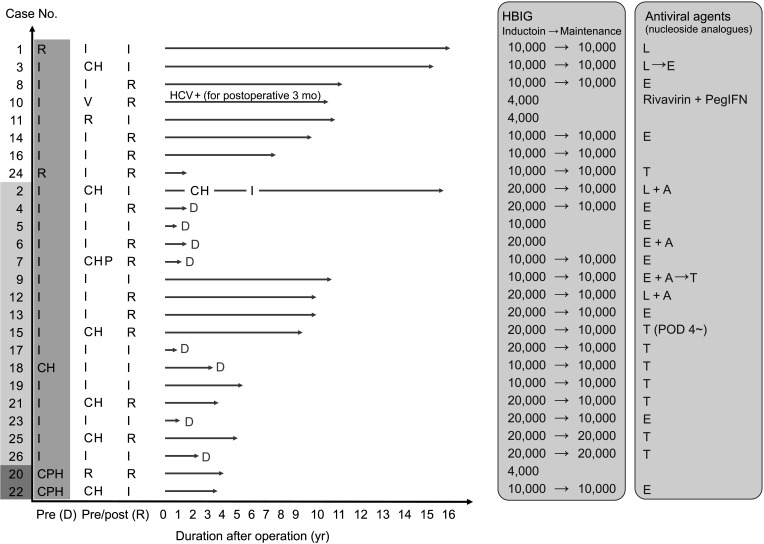
Prophylaxis for HBV reactivation using intravenous HBIG (Hepabig, Green Cross) was initiated intraoperatively during the anhepatic phase (induction dose) and maintained (maintenance dose) in most cases (Fig. 2). An induction dose of 10,000 or 20,000 IU and maintenance dose of 10,000 IU was administered to recipients transplanted with HBsAg (+) grafts. After discharge, approximately 10,000 IU of HBIG was administered according to the serum HBsAb levels, which were measured regularly at the outpatient clinic. Nucleoside/nucleotide analogues (NAs) were also routinely used after LT.
Statistical analyses
IBM SPSS Statistics ver. 27.0 (IBM Corp.) was used for statistical analyses. The Student t-test was used to analyze continuous variables, and categorical variables were analyzed using the chi-square or Fisher exact test. The Kaplan-Meier method was used to evaluate and compare patient survival, and the log-rank test was used to compare survival curves. Statistical significance was set at the P-values of <0.05.
RESULTS
Demographics
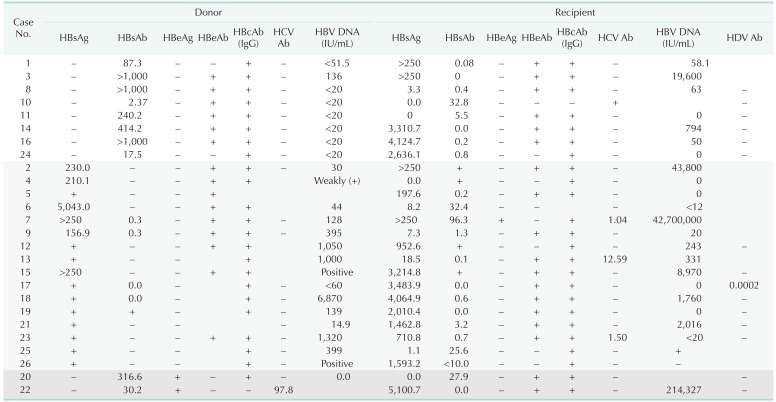
The study included 10 LDLTs and 16 deceased donor LTs (DDLTs). All HBsAg (+) grafts were from deceased donors and were transplanted into recipients who had a history of HBV infection. Among recipients who received grafts from living donors, 2 received HBsAb (+) and HBeAg (+) grafts, and 8 received HBcAb (IgG) (+) and HBV DNA (+) grafts. The 8 donors who were HBcAb (+) and HBV DNA (+) were determined to be in the HBV immune-inactive stage with low viral replication.
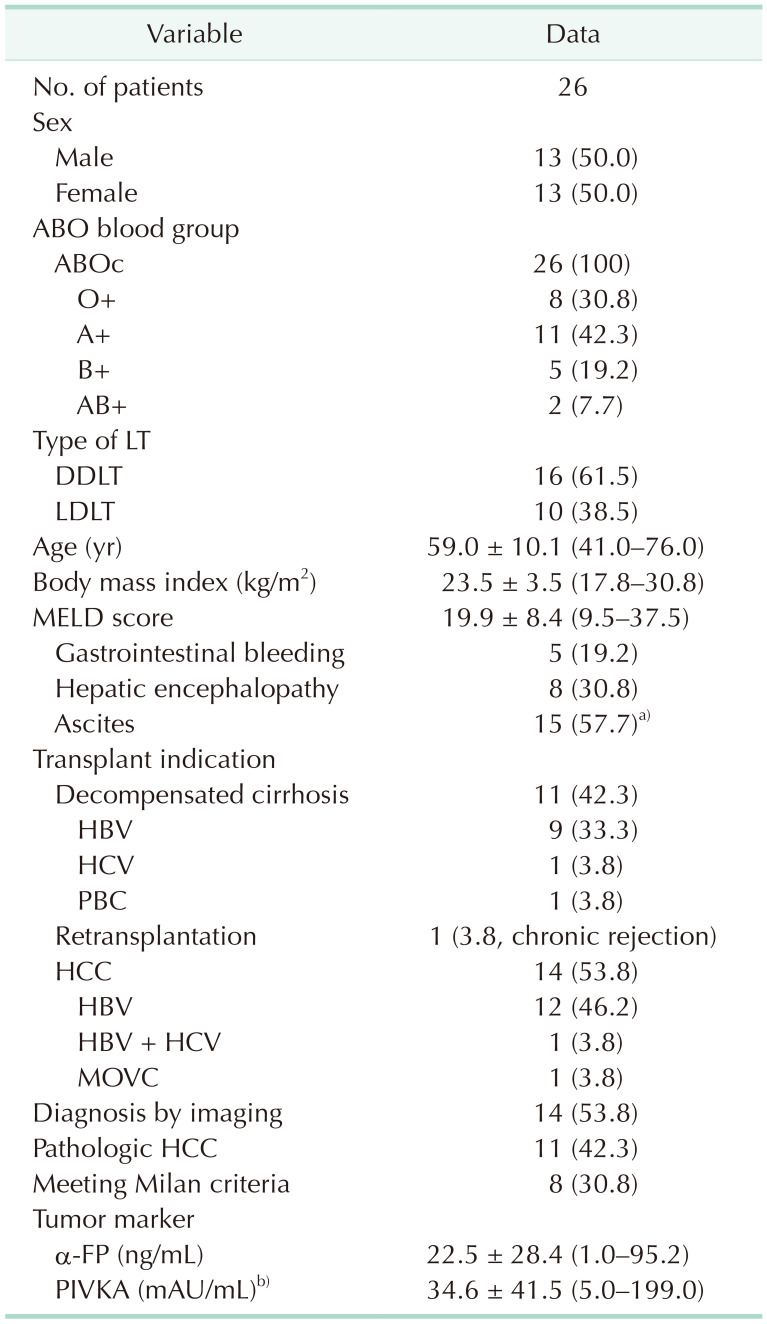
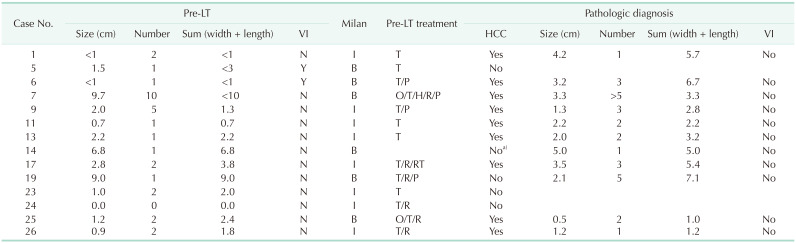
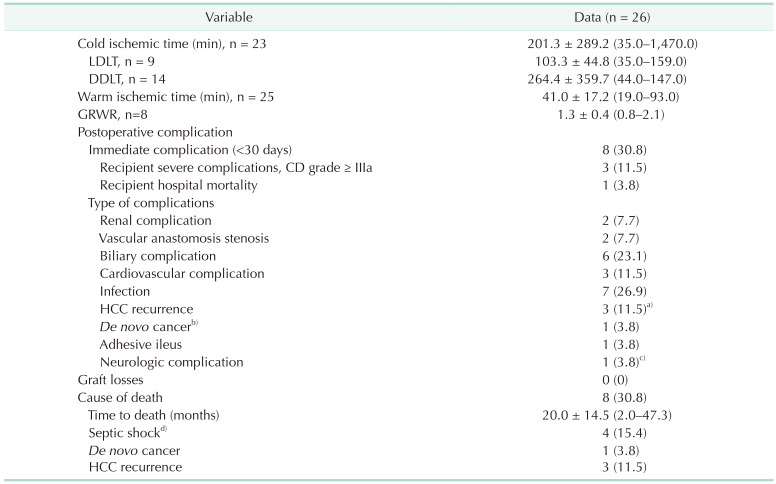
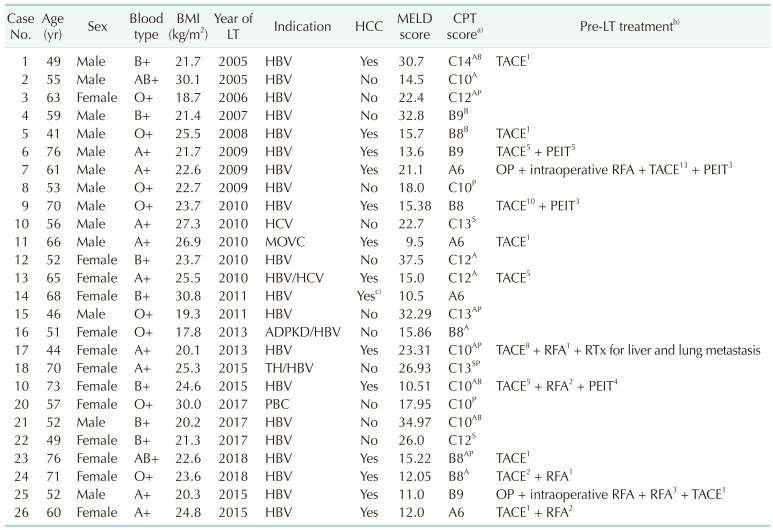
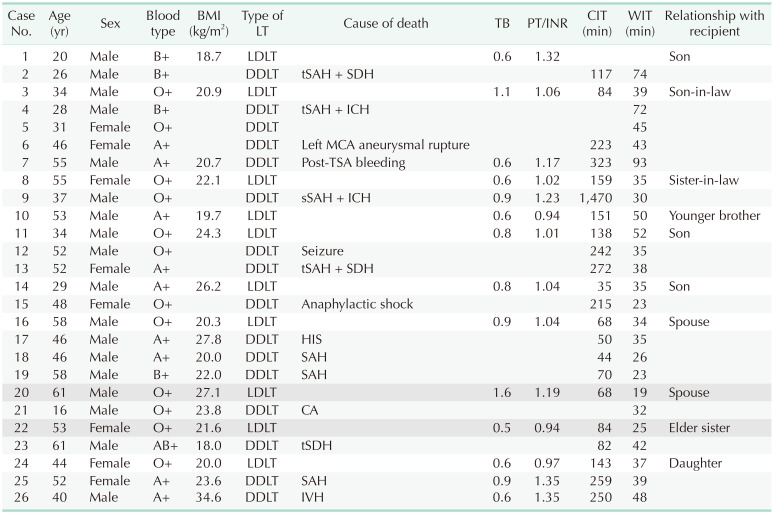
The mean age of the recipients was 59.0 ± 10.1 years (Table 1). The male-to-female ratio was 1:1. The mean body mass index (kg/m2) was 23.5 ± 3.5. The mean Model for End-Stage Liver Disease (MELD) score of the recipients before LT was 19.9 ± 8.4 (range, 9.5–37.5). There was no significant difference in MELD scores between DDLT and LDLT recipients (18.6 ± 7.0 vs. 20.7 ± 9.3, P = 0.150). The most common indication for LT was decompensated cirrhosis. Retransplantation was performed in 1 patient who had experienced chronic rejection after DDLT. Fourteen patients (53.8%) underwent LT for HCC. The numbers of HCC tumors ranged from 1 to 5, and the average tumor size was 3.96 ± 2.03 cm (range, 1.0–7.1 cm). Eight patients (30.8%) with HCC met the Milan criteria, and 6 exceeded the threshold Milan criteria (Table 2). Table 3 shows the serological statuses of donors and recipients. Cold ischemic time was shorter in the LDLT group (103.3 ± 44.8 minutes) than that in the DDLT group (264.4 ± 359.7 minutes) (Table 4). The graft-to-recipient weight ratio was 1.3 ± 0.4 in 8 LDLTs. Detailed information on each donor and recipient is presented in Tables 5 and 6.
Outcomes
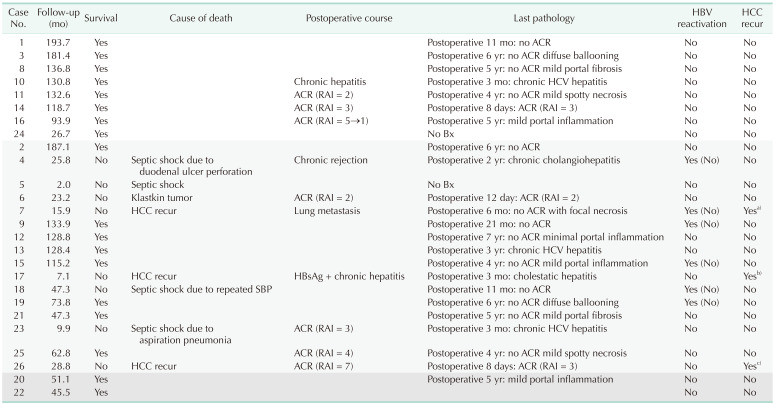
Immediate postoperative complications (postoperative days, 1–29) were reported in 8 patients (30.8%). Severe complications (Clavien-Dindo classification, ≥IIIa) were reported in 4 patients. The most common complication was infection. Three patients (11.5%) had HCC recurrence, and all of them died owing to cancer. Bone metastasis was detected in patient 7 on postoperative day 340. Patient 17 was found to have HBV recurrence in the liver and perihepatic space on postoperative day 390. Patient 26 was diagnosed with HCC metastasis in the pleura, chest wall, diaphragm, and lung on postoperative day 249. All 3 patients remained inactive HBV carriers, and HBV DNA was absent despite HCC progression after LT. No graft loss was identified in any of the patients during the follow-up period. The most common cause of death was septic shock. All deaths occurred in recipients who received HBsAg (+) grafts (Table 7, Fig. 2). The last biopsy results showed that all rejections were appropriately treated, and that there was no chronic liver damage in the surviving recipients. Based on our definition of reactivation, no HBV reactivation was observed during the follow-up period.
The target serum HBsAb level for HBIG administration was over 200 IU/mL during the posttransplantation period. Only 4,000 IU of HBIG was used for induction in patients 10 and 11 because serum HBsAg could not be detected and their serum HBV levels were low (<20 IU/mL). Patients who received HBsAb (+) and HBeAg (+) grafts (n = 2) were also treated with HBIG. The recipient who was in the resolved stage at the time of transplantation received 4,000 IU for the first 3 days posttransplantation based on their serology (HBsAg [–], HBsAb [+], and HBcAb [+]). Another recipient with chronic HBV was administered 10,000 IU in the long term. All but 4 LT recipients were administered NAs to prevent HBV reactivation; NAs were strictly administered postoperatively to those who received HBsAg (+) grafts.
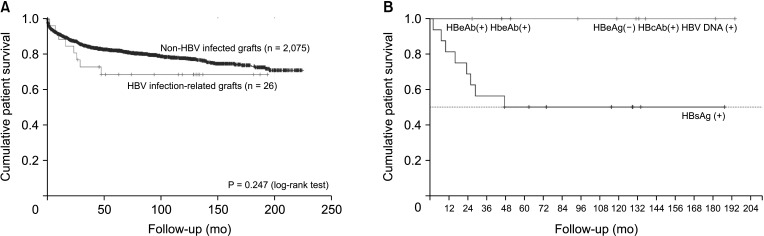
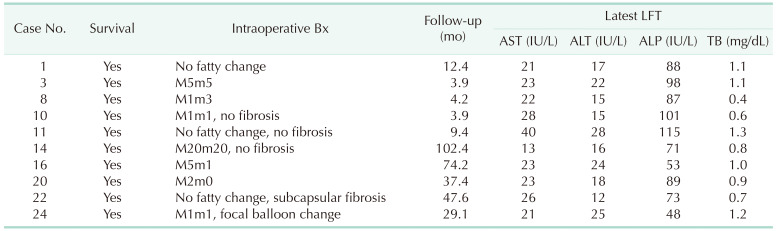
The mean follow-up duration was 82.6 ± 60.1 months, and the mean time to death was 20.0 ± 14.5 months (range, 2.0–47.3 months). The overall mortality rate was 30.8% (8 of 26), which was higher than the 18.6% mortality rate (387 of 2,076) among patients who received transplants from donors without HBV infection. However, there was no significant difference in patient survival (P = 0.250) (Fig. 3B). All living donors survived, and their most recent liver function test results were normal (Table 8).
DISCUSSION
Previous attempts to use chronic hepatitis or healthy HBV carrier grafts have shown outcomes comparable to those resulting from grafts from HBV-negative patients [12]. Development of antiviral agents with low resistance rates and HBIG has enabled the expansion of the LT donor pool to include HBV-infected graft tissue [1819]. Moreover, other studies have reported that chronic hepatitis grafts may be safely transplanted to vaccinated recipients without a history of HBV infection [5]. Therefore, grafts from HBV-positive donors may even be considered in recipients without a history of HBV infection if perioperative immunization and NA and HBIG therapies are administered. According to the 2020 position statement and recommendations of the European Liver and Intestine Transplantation Association (ELITA), HBsAg (+) grafts may be used after an assessment of the risks and benefits for each recipient. Moreover, HBsAg (+) grafts should be considered whenever there is an option of indefinite prophylaxis with entecavir or tenofovir [20].
After a nationwide HBV vaccination program was started in 1983, the vertical transmission rate of HBV in Korea decreased [21], and the overall prevalence of HBsAg carriage has remained at 2.9% since 2010 (intermediate endemicity range, 2%–7%) [16]. However, data from 2016 demonstrated that the prevalence of HBsAg in older age groups has remained higher than that in younger age groups [6]. Thus, using grafts from donors with chronic or active HBV infection could potentially increase the donor pool.
Reactivation of HBV was initially defined based on classical criteria, including an increased HBV DNA titer and positive seroconversion of HBsAg. However, in recipients of HBsAg (+) grafts, HBV recurrence should be defined as an increase in serum HBV DNA titer, because recipients have a persistent HBsAg (+) status [17]. HBeAg and HBV titers should also be monitored in these patients. In this study, recipient 2 was the only patient in the HBsAg (+) group in whom an increased HBV DNA titer was observed. The elevated HBV DNA titer in recipient 2 resolved spontaneously by 5 years postoperatively; their HBeAg test result was negative, and liver function test results were within the normal range. The results of this patient’s most recent pathology tests at 6 years postoperatively were normal.
We described the stage of HBV infection after LT [2223]. This staging addresses both HBV infection status and liver damage and seems to provide an accurate interpretation of the clinical aspects of HBV infection. Nevertheless, patients with chronic HBV infection may show various serologic profiles that do not clearly fit the criteria for chronic infection, especially in HBV-endemic areas. Therefore, we consulted with our hepatologist while classifying the infection stages of such patients. All donors and recipients were in varying stages of chronic hepatitis, except recipient 8, who was vaccinated before undergoing LT. LT recipients who survived were all classified as either inactive (n = 7) or resolved (n = 11), indicating that HBV was well controlled in these patients [24]. Living donors were classified as HBV resolving (n = 8, HBcAb [+] HBV DNA [+]/immune-inactive stage with low viral replication) or resolved (n = 2, HBsAb [+) HBeAg [+]) at the time of transplantation. The liver function test results were normal during the follow-up; this might indicate that liver donors with a stable HBV infection stage can safely donate their liver, even though major hepatectomy is known to be a major insult that may lead to an HBV flare-up, even in a healthy carrier.
HDV coinfection suppresses HBV recurrence in LT patients [25]. However, others have reported that recipients with HDV have poor prognosis owing to progression of HDV-inducing cirrhosis [2627]. In addition, HDV may contribute to HCC recurrence and de novo HCC progression [2527]. To improve surgical outcomes, clinicians must consider HDV infection status in both grafts and recipients when using grafts from HBV-positive donors, and screening for HDV should be a part of pre-LT assessments. The ELITA statement strongly suggests that HBsAg (+) grafts should be discharged when HDV is present in either the donor or the recipient [15].
Most deaths were reported approximately 2 years after LT. The relatively high mortality observed among patients transplanted with HBsAg (+) grafts seems to reflect the critically ill condition of patients undergoing DDLT. During the same period, HCC recurrence was reported, but no deaths were reported beyond 5 years after LT. Infection occurs most frequently at 2–4 years posttransplantation [28]. Early HCC recurrence is most common at 14–16 months postoperatively, although late recurrence may occur >5 years posttransplantation [1415]. Saab et al. [28] reported that HBV recurrence does not directly affect transplantation outcomes. However, many other studies have shown that HBV infection and HCC recurrence are closely related [2930]. In our study, 14 patients were followed up for >5 years; all were stable, and no increase in HCC recurrence rate was observed 5 years after transplantation. In addition, there was no difference in patient survival between those who underwent LT with HBV-infected grafts and those with non–HBV-infected grafts.
This study had a few limitations. First, the small patient cohort (n = 26) hindered clear interpretation of the results and prevented identification of risk factors affecting transplantation outcomes. Additionally, the lack of regular liver biopsies during follow-up restricted the accurate evaluation of long-term graft condition.
Nevertheless, the strengths of this study are its long-term evaluation of the safety of grafts from HBV-positive donors, and its introduction of HBV infection stage assessments for evaluating viral progression in the posttransplantation period. These assessments demonstrated that HBV recurrence and HCC risk were not significantly increased over the long term in LTs using HBV-infected grafts. In addition, grafts that are HBeAg (+), HBcAb (+), and HBV DNA (+) are considered safe to use in terms of long-term survival, HBV reactivation, and HCC recurrence. Furthermore, setting a standard management and follow-up schedule for transplantation using HBsAb (+), HBeAg (+), and HBcAb (+) HBV DNA (+) grafts is necessary to improve technique safety.
In conclusion, liver grafts from donors with active or chronic HBV infection can be safely used in the long term. Considering their comparable outcomes with HBV-negative donor grafts, they can be safely used in HBV-endemic areas to effectively expand donor pools.
 XML Download
XML Download