

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
One of the most common types of cancer worldwide is hepatocellular carcinoma (HCC), which is often a complication in patients suffering from chronic liver diseases [1]. The initial treatment preference for patients who have small, singular tumors is liver resection (LR) [1].
There are various causes of HCC, including HBV, HCV, and alcohol use, and these risk factors cause chronic liver disease through continuous liver inflammation, resulting in recurring liver fibrosis and hepatocyte regeneration. In addition, as epigenetic molecular changes occur, cells develop cancerous features, and liver cancer eventually occurs [2].
For these reasons, the majority of HCC patients have coexisting liver cirrhosis, and liver functional reserve is one of the key prognostic factors [3]. There is a widely accepted notion that liver cirrhosis is an independent and unfavorable risk factor that can affect the survival of patients who have undergone HCC resection [45] and the development of liver fibrosis and cirrhosis as a result of chronic liver diseases is a major contributor to the high rates of morbidity and mortality.
Therefore, evaluating the fibrotic stage of the liver in these patients is important, and there are a variety of methods, such as imaging modalities, laboratory findings, and liver biopsy, which is the gold standard tool for staging cirrhosis [67]. However, since liver biopsy is an invasive procedure, it can be difficult to do in patients with certain medical conditions and socioeconomic statuses, and there are possible limitations associated with variations in practitioner approaches and errors in the sampling process [8].
For this reason, various staging systems, such as the Child-Pugh score, Barcelona Clinic Liver Cancer (BCLC) staging system, Fibrosis-4 index (FIB-4), AST-to-platelet ratio index (APRI), AST-to-ALT ratio (AAR), AAR-to-platelet ratio index (AARPRI), and albumin-bilirubin (ALBI) score, and liver function models have been used recently to determine the degree of liver cirrhosis and to predict the prognosis of HCC [9101112].
Initially, the Child-Pugh score was developed to predict the prognosis of cirrhotic patients undergoing surgery for portal hypertension [13]. This score appears to be a reliable predictor of survival and has been the reference for assessing the stage of cirrhosis in HCC patients [14]. However, there are some limitations, as this score consists of subjective variables (ascites and encephalopathy) and is designed for cirrhotic patients. BCLC staging was an overall guideline for treatment methods in HCC patients, and it was also related to the prognosis [15]. Since most cases considering curative surgical resection had low staging, it was thought that there might be pitfalls in predicting the prognosis of patients who had undergone surgical treatment as in this study.
Although these staging systems and liver reserve models were not developed to predict HCC prognosis, several studies have investigated their prognostic values in predicting the prognosis of HCC patients after curative hepatic resection. The aim of our study is to evaluate which biomarkers are meaningful in predicting the prognosis after curative LR in HCC patients.
METHODS
Study design and population
This study was approved by the Institutional Review Board of Samsung Medical Center (No. 2021-05-167-004). This study was a prospective study and was reviewed retrospective way. Data were collected using an electronic medical record system. Between 2006 and 2013, a total of 973 patients were diagnosed with HCC and underwent hepatic resection at Samsung Medical Center. HCC diagnosis was based on the noninvasive criteria of the American Association for the Study of Liver Diseases. All laboratory data, including the tumor marker for HCC and α-FP, were measured at the time of HCC diagnosis. We excluded patients who underwent combined operations, such as intraoperative radiofrequency ablation (RFA), other major organ operations due to simultaneous primary cancer, and metastasectomy (n = 11). In total, 962 patients were included in this study.
Preoperative evaluation and indications for hepatectomy
Laboratory findings for liver function tests included conventional liver function tests and the indocyanine green retention rate at 15 minutes (ICG-R15). Tumor markers used for liver cancer, including α-FP and protein induced by vitamin K absence/antagonism-II (PIVKA-II), were also measured in all patients. Preoperative evaluation included chest CT, cardiac echogram, electrocardiogram, enhanced liver CT, liver magnetic resonance imaging, and PET/CT [16]. HCC diagnoses were confirmed based on the current American, European, and Korean practice guidelines [1718].
Selection criteria for the LR procedure were tumor location and extent, liver function, ICG test, and future liver remnant volume. In patients without ascites and with normal bilirubin levels, ICG-R15 was the main resectability determinant [16].
Surgery and pathology
Standard operative techniques for hepatectomy were used. Adequate mobilization was achieved based on the part of the liver to be resected. Selective clamping of the portal vein and hepatic artery was performed when feasible; if not, the intermittent Pringle maneuver was used. Parenchymal transection was performed using a cavitron ultrasonic surgical aspirator under low central venous pressure. Major hepatectomy was defined as the resection of 3 or more Couinaud segments, and minor hepatectomy was defined as the resection of fewer than 3 segments. Postoperative histological assessment and reporting included maximal tumor size, tumor number, encapsulation, tumor hemorrhage, tumor grade, tumor necrosis, portal vein tumor thrombosis, bile duct tumor thrombosis, intrahepatic metastasis, multicentric occurrence, microvascular invasion, serosal involvement, tumor-free resection margin, and cirrhosis [19].
Surveillance after surgical resection
The procedures used for surveillance after LR are previously described. All patients were followed up 1 month postoperatively and then every 2 or 3 months thereafter. Follow-up parameters included physical examination, chest X-rays, and tests for serum α-FP, PIVKA-II, and liver function. Abdominal CT was performed every 3 months or when recurrence was suspected. MRI and/or PET scans were performed if CT did not show definitive evidence of recurrence. Patients with intrahepatic recurrences were treated with RFA, transcatheter arterial chemoembolization, LR, liver transplantation, or radiation according to their functional liver reserve and pattern of recurrence. The follow-up period was the length of time from surgery to the final follow-up or death, and the median follow-up period was 58.8 months.




Statistical analysis
The primary endpoint was 2-year disease-free survival and overall survival. Patient data were collected from electronic medical records. Categorical variables were expressed as numbers and percentages and compared using the chi-square test or Fisher exact test. Continuous variables were expressed as mean ± standard deviation and median with 95% confidence interval (CI), compared using the t-test or Mann-Whitney U-test. Receiver operator curve analysis was used to determine the optimal cut-off values for biomarkers.
After binarizing the fibrosis stage into a higher stage (stage 3 or higher) and a lower stage, biomarkers with higher area under the curve (AUC) values were selected as predictors. The cut-off value for each biomarker was determined by the receiver operating characteristics (ROC) curve. Univariate analyses were performed to identify risk factors for recurrence and death using a Cox regression model. Multivariate analysis was performed using a Cox proportional hazard model on all variables that were significantly associated with survival by univariate analysis. Patient survival and recurrence were calculated using the Kaplan-Meier method and compared using the log-rank test. A P-value of <0.05 was considered statistically significant. All data were analyzed using IBM SPSS Statistics ver. 26.0 (IBM Corp.).
RESULTS
Study patient characteristics
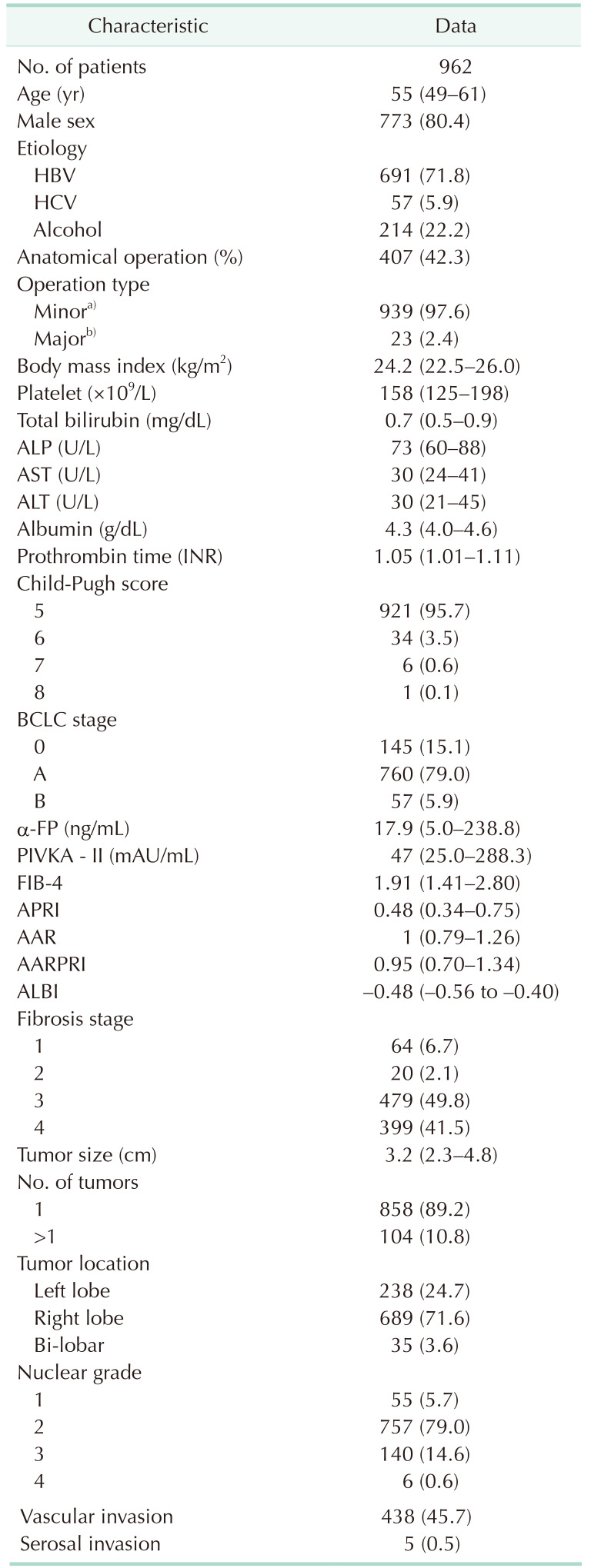
The median age of the patient group was 55 years 95% CI, 49–61 years), and the cohort was predominantly male (n = 773, 80.4%). The most common cause of HCC was HBV (n = 691, 71.8%), followed by alcohol (n = 214, 22.2%) and HCV (n = 57, 5.9%). The number of patients who underwent anatomical resection was 407 (42.3%) and most patients underwent minor hepatectomy defined as hepatectomy of less than 3 segments (n = 939, 97.6%). The median values of liver-related laboratory findings in the entire patient group were within the normal range, and those of α-FP and PIVKA-II levels were 17.9 (95% CI, 5.0–238.8) and 47 (95% CI, 25.0–288.3), respectively. Most patients were included in Child-Pugh scores of 5 (n = 921, 95.7%) and BCLC stage of A (n = 760, 79.0%).
The median size of HCC was 3.2 cm (95% CI, 2.3–4.8 cm), and most of them were solitary mass (n = 858, 89.2%). Microvascular invasion was observed in 45.7% and serosal invasion was observed in 0.5% of patients. We retrospectively studied fibrosis stage by pathologic reports (Metavir fibrosis stage for non-tumor liver lesion). For statistics, the 4 fibrosis stages were divided into a lower stage (stage 1 and 2; n = 84, 8.7%) and a higher stage (stage 3 and 4; n = 878, 91.3%). The details are described in Table 1.
Area under the receiver operating characteristics curve of each biomarker and cut-off values
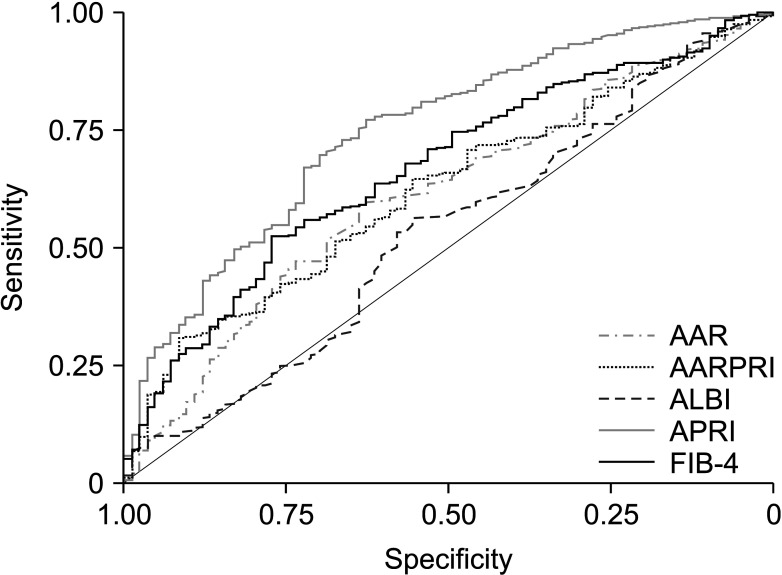
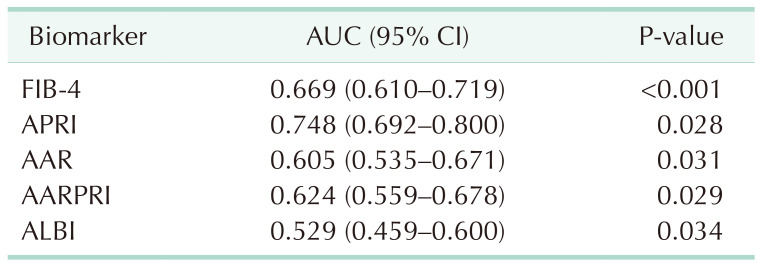
Table 2 shows the area under the ROC curve (AUROC) values for fibrosis stage about the 5 biomarkers included in this study, and AUROC comparison graphs are shown in Fig. 1. Among them, the AUROC values for FIB-4 and APRI were larger than the other biomarkers and included in that statistical analysis of recurrence and overall survival; 0.669 (95% CI, 0.610–719) and 0.748 (95% CI, 0.692–0.800), respectively.
Table 3 summarizes the cut-off values of FIB-4 and APRI for fibrosis stage. Method of calculating the cut-off values for these biomarkers was described in the ‘Statistical analysis’ section and values of each biomarkers were 1.67 and 0.34, respectively.
Risk factors for 2-year recurrence-free survival and overall survival
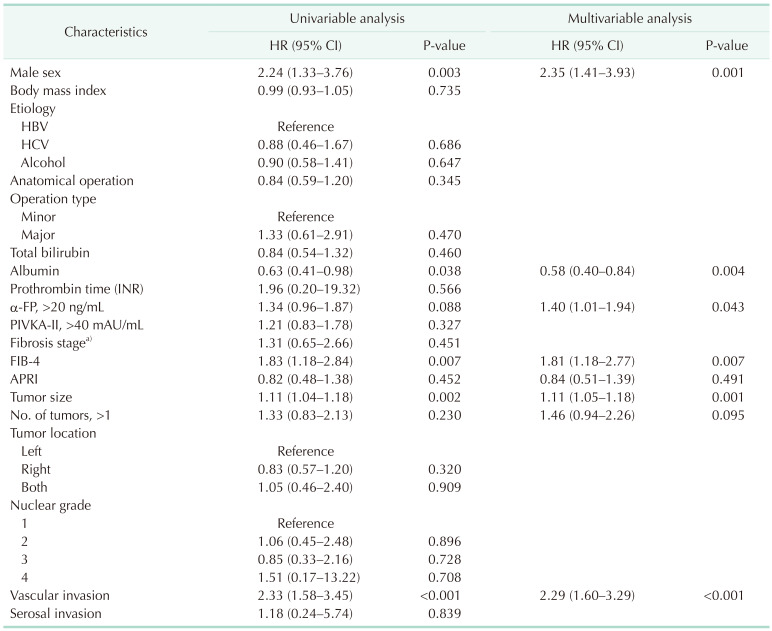
Thereafter, the hazard ratio (HR) was calculated through Cox regression analysis for all variables included in the baseline characteristics of the patient group after excluding the laboratory findings and variables included in the calculation of each noninvasive biomarker among them, such as AST, ALT, platelet, and age, and the results are shown in Table 4.
In the multivariable analysis for recurrence, sex, albumin level, α-FP level of >20 ng/mL, tumor size, and microvascular invasion were statistically significant predictive variables. HRs of each value were 2.35 (95% CI, 1.41–3.93; P = 0.001), 0.58 (95% CI, 0.40–0.84; P = 0.004), 1.40 (95% CI, 1.01–1.94; P = 0.043), 1.11 (95% CI, 1.05–1.18; P = 0.001), and 2.29 (95% CI, 1.60–3.29; P <0.001). FIB-4 showed a statistically significant result as a prognostic factor for recurrence (1.81; 95% CI, 1.18–2.77; P = 0.007); however, APRI was not (P = 0.510).
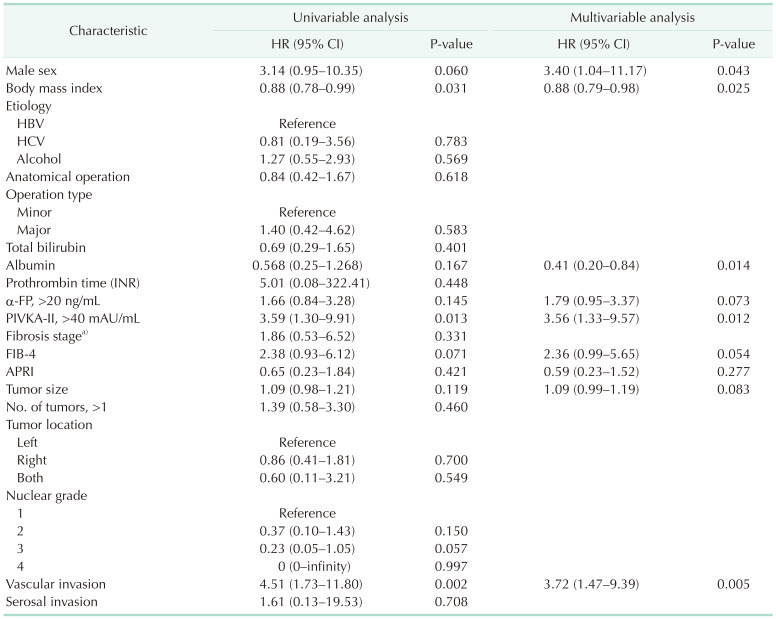
Sex, body mass index (BMI), total bilirubin, PIVKA-II of >40, and microvascular invasion were statistically significant predictive variables of 2-year overall survival and the results were shown in Table 5. About FIB-4 and APRI, HRs were 2.36 (95% CI, 0.99–5.65; P = 0.054) and 0.59 (95% CI, 0.23–1.52; P = 0.277), respectively.
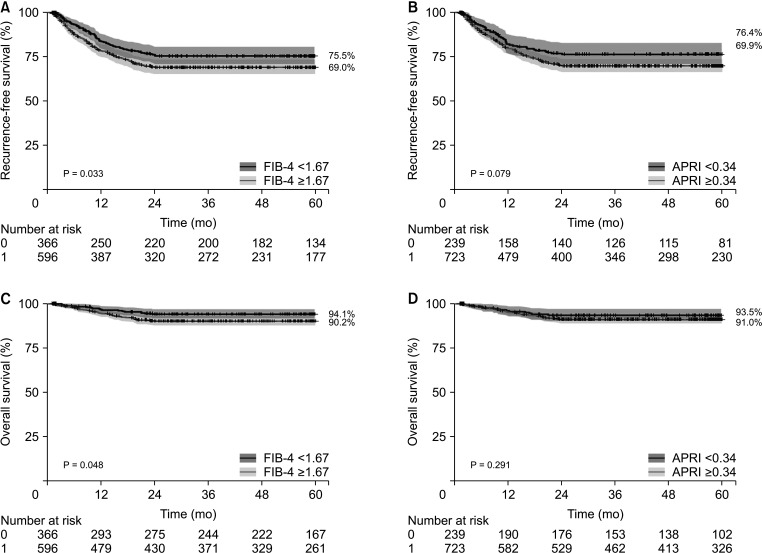
Fig. 2 summarized the Kaplan-Meier curve of recurrence and overall survival according to these 2 biomarkers (FIB-4 and APRI). The group with lower FIB-4 value showed better survival outcomes in recurrence and overall survival (P = 0.033 and P = 0.048, respectively). For long-term survival, 5-year overall survival was 84.4%, and 5-year recurrence-free survival was 62.5%.
Correlation between fibrosis stage and biomarkers
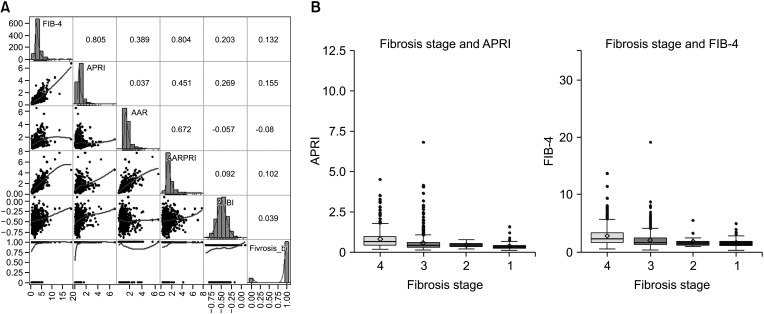
There was no significant correlation between the 5 biomarkers (FIB-4, APRI, AAR, AARPRI, and ALBI) and fibrosis stage binarized lower and higher stage according to the pathologic report (each Spearman correlation value was 0.132, 0.155, –0.08, 0.102, and 0.039, respectively) (Fig. 3A). Box plot of FIB-4 and APRI, variables included final survival analysis, according to 4 fibrosis stages was shown Fig. 3B (since there were few patients belonging to stage 1, we set both 0 and 1 stages to stage 1 and drew a box plot). The higher the stage, the higher the FIB-4 and APRI values, but as described above, the results were statistically insignificant.
DISCUSSION
Preoperative diagnosis of liver fibrosis before hepatectomy in HCC patients is important in determining the operability and extent of LR since liver fibrosis and cirrhosis often accompany impaired liver function and are associated with postoperative liver dysfunction, which increases morbidity and mortality [23].
A major obstacle to HCC treatment is the high frequency of recurrence even after curative hepatectomy [24], therefore we focused on short-term (2-year) outcomes. The recurrence rate and prognosis of HCC are influenced by the features of the tumor and the initial function of the liver. Large tumor size, microvascular invasion, and cirrhosis are usually important contributing factors for tumor recurrence and mortality [25].
Many studies have suggested that hepatic function plays an important role in HCC prognosis after surgery [26]. Preoperative evaluation of hepatic functional reserve through noninvasive methods is essential for individualized surgical strategies. In particular, serum albumin and bilirubin levels are important factors. In the case of functional reserves such as albumin or international normalized ratio (INR), these are also meaningful as variables that determine hepatic resection and constitute a model like the Child-Pugh score. The Child-Pugh score and BCLC stage are closely related to liver cirrhosis, one of the major risk factors for HCC, as mentioned above [27].
In our study, the majority of patients were Child-Pugh scores of 5 (n = 921, 95.7%) and early BCLC stage of 0 (n = 145, 15.1%) or A (n = 760, 79.0%). Since these staging systems were designed to determine the liver function and treatment method of HCC patients, most patients considering curative LR have no choice but to belong to early staging of Child-Pugh scores and BCLC stage due to the retrospective study design. There might be limitations in predicting prognosis of HCC patients through these models, so there is a need for research on new models to predict prognosis after curative LR in HCC patients. For these reasons, we retrospectively studied the relationship between noninvasive biomarkers and HCC prognosis for those who have undergone curative hepatectomy using preoperative laboratory findings. The noninvasive scoring models that are used to measure hepatic function impairment, including the FIB-4, APRI, AAR, and AARPRI, were developed in chronic HCV patients [28]. The ALBI grade has been also proposed as a simple and objective method to assess functional reservoirs in HCC [26].
The reason we tried to find a correlation between fibrosis and these biomarkers was that the occurrence of HCC was ultimately due to epigenetic changes caused by chronic infection or inflammation [2] which leads to liver fibrosis, and the degree of liver fibrosis was associated with the development of liver cancer [29]. We examined 5 different noninvasive biomarkers mostly based on laboratory findings. Unlike previous studies supporting there was a correlation between the fibrosis stage and these biomarkers [11], we did not find any correlation. As described above in ‘Introduction’ section, epigenetic changes caused by repetitive inflammation and resulting fibrosis are very important mechanisms in the pathogenesis of HCC. Although there is no statistical correlation between fibrosis stage and noninvasive biomarkers in our study, it is a commonly known clinical relationship between the biomarkers and fibrosis stage has been revealed. Instead, FIB-4 and APRI showed higher AUC values than the others and we evaluated these 2 biomarkers as predictors of HCC patients after curative hepatectomy. FIB-4 showed statistically significant results in predicting recurrence (P = 0.007). For overall survival (P = 0.054), there is no statistically significant difference, but there is such a tendency that additional data analysis is required.
In addition to these biomarkers, several variables have been shown to be helpful in predicting the prognosis of HCC patients. Child-Pugh score, one of the most universally used liver function models, consisted of 2 clinical variables and 3 laboratory findings. Among them, higher albumin level showed better prognosis in both recurrence-free survival and overall survival outcomes (P = 0.004 and P = 0.014, respectively). However, serum bilirubin and INR levels were not prognostic factors in both recurrence-free survival and overall survival. High α-FP level (over 20 ng/mL) was also the risk factor for recurrence (P = 0.043). While no statistically significant difference in overall survival was observed for patients with high α-FP levels, there is a trend toward a potential effect. However, further data analysis is needed to confirm this trend as the P-value falls within the marginally significant range (P > 0.05 and P < 0.1). Vascular invasion by tumor has been a clinical dilemma in treating patients with HCC owing to its close correlation with post-treatment tumor recurrence. After curative therapy for HCC, patients with vascular invasion face frequent tumor recurrence and challenges in treatment allocation. These limitations can negatively impact their long-term survival [30]. Our analysis showed that the presence of microvascular invasion, as confirmed by histological examination following hepatectomy, was a significant negative prognostic factor for both recurrence and survival (P < 0.001 and P < 0.005, respectively).
In addition to the 5 noninvasive biomarkers we introduced earlier and used in our study, new noninvasive biomarkers have recently been developed. As a simple predictor of liver fibrosis, the fibrosis-cirrhosis index (FCI) comprised of ALP, bilirubin, serum albumin, and platelet count targeting HCV patients in 2011 was studied [31]. In addition, FIB-5, which developed FIB-4, is comprised of ALT, AST, ALP, albumin, and platelet count for the detection of significant hepatic fibrosis in patients with chronic hepatitis C [32] or King’s fibrosis score comprised of age, AST, and platelet counts were also studied [33].
Noninvasive liver fibrosis biomarkers for nonalcoholic fatty liver disease, which have recently been watched with interest, are also being studied. HAIR (hypertension, ALT, insulin resistance), NAFLD fibrosis score (age, BMI, hyperglycemia, platelet count, albumin, AST/ALT ratio), BAAD score (BMI, AST/ALT ratio, diabetes mellitus) have been developed, all of which has been reported to be useful for predicting liver fibrosis [34].
However, there are no separately developed biomarkers that predict the prognosis after surgical treatment in HCC patients. Instead, most of the predictions are made using existing noninvasive fibrosis biomarkers. Therefore, it seems that research on this will be necessary in the future, and we are collecting additional data for this purpose.
There are several limitations to this study. All patients were ethnically Korean, and the predominant etiology of liver fibrosis was HBV infection. However, FIB-4, an index designed to find out the degree of liver fibrosis in HCV-infected patients, is considered to be important in that it is also meaningful in predicting the prognosis of HCC patients in the HBV-dominant populations. There is also the possibility of a selection bias, as all patients were treated at a tertiary single center. Due to the homogeneous nature of the study population and considering that this is a single-center study, there are limitations to applying the above results to the entire population. These results should be evaluated in other ethnicities with a different distribution of liver fibrosis etiologies and further prospective multi-institutional studies that include not only resection cases but also patients who undergo other curative treatments to evaluate the true usefulness and generalizability of the FIB-4 as prognostic factors after curative treatment for HCC patients. In addition, the present study was based on a retrospective review of an accumulated database. However, there were no missing data, as the FIB-4 indexes were included in the standard preoperative investigations, and the design of the present study is thought to be similar to that of other studies based on prospectively accumulated data. Finally, previous HCC treatment history was thought to be an important factor in predicting HCC prognosis after hepatectomy, but it was not included in this study. We plan to collect related data and carry out additional research in the future.
In conclusion, we found noninvasive laboratory index, FIB-4, was a statistically significant predictor of prognosis in HCC patients of HBV-dominant populations after curative LR. The meaning of our study is not simply to predict prognosis based on these laboratory findings but rather to suggest that more intensive surveillance and postoperative management are required if a poor prognosis is predicted preoperatively.

 XML Download
XML Download