

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Internet use has become a youth's most important academic and recreational tool.1 According to the surge in smartphone ownership, adolescents frequently use smartphones after school, during classes, while eating, and while taking transportation.23 However, problematic internet gaming and internet addiction are becoming increasingly serious problems.4 Several studies showed that the risk factors for internet gaming disorder (IGD) include social isolation, lower-quality interpersonal relationships, low academic achievement, limited recreational activities, and low self-esteem.5678
The American Psychiatric Association (APA) determined that IGD required data accumulation and further research, therefore, it included IGD in section III of the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5) in 2013.91011 IGD is defined by the support of at least five core symptoms (from nine) in over one 12-month period, according to the DSM-5.912 IGD is associated with health-related outcomes such as social health, psychological health and physical health.13
IGD affected children and adolescents experience negative impacts on their mental health.141516 Recent studies1718 reported that depression and anxiety are positive independent predictors of IGD. A previous study19 reported ADHD (Attention Deficit Hyperactivity Disorder) and a large number of psychiatric IGD comorbidities in Korean children. In addition, previous study results have shown positive relationships between IGD, depression, anxiety, insomnia, and stress among adolescents.20 IGD directly influenced quality of life and insomnia among 1512 adolescents aged 13–18 years.21
Exposure to Adverse childhood experiences (ACEs) is an important predictor of addiction problems.22 Primarily young people experiencing household dysfunction reported increased levels of psychological symptoms and substance-related problems. According to previous studies, it was reported that pediatric symptoms were mediated by the relationship between ACEs and IGD.18232425 Recently, we reported that ACEs in selected populations affected IGD by mediating its relationship with depressive symptoms.26 Previous studies reported an association between ACEs and the risk for various types of addiction such as alcohol abuse, drug addiction, food addiction, and drug addiction.2728 Furthermore, the prior findings showed that ACEs exposure and addictive behaviors had a close relationship.29
Research has shown that individuals who experience ACEs are at a higher risk of developing addiction and substance use disorders later in life.30 One item of the ACEs measure included a family history of addiction.31 Especially, a family history of addiction has commonly been reported to increase the likelihood of other addictions.3233 A family history of addiction might help identify children and adolescents who are at risk for psychological problems. Moreover, investigating the family history of addiction in a pediatric population could allow for understanding of the impact of addiction behaviors and pediatric symptoms on development.34
However, there is a lack of empirical evidence on how a family history of addiction as an ACE influences IGD among children and adolescents. To the best of our knowledge, there are no published studies that more comprehensively focus on the relationship between a family history of addiction, IGD, and pediatric symptoms (attention, internalizing problems, and externalizing problems). Thus, our hypothesis is that pediatric symptoms (attention, externalization problems, and internalization problems) had a mediating effect on the association between family history of addiction and IGD in children and adolescents.
METHODS
Participants and procedure
We conducted an analysis using the results of an annual survey (2018 report of the survey on smart digital media among adolescents in Nowon-gu) performed by the Nowon Community Addiction Management Center in Korea. The participants were selected from 2,701 children and adolescents from 16 elementary, middle, and high schools and 8 local children’s community centers in a capital city in South Korea. The sample of the study subjects used a multi-stage cluster sampling method. In order to recruit research participants, the first stage was to extract the research target schools and local children’s centers from the institutions located in the region, and then in the second stage, the subjects to be surveyed were selected. The respondents completed a self-reported structured questionnaire and the questionnaire included demographic characteristics of age, sex, and school type. After the questionnaire, it was used as data collected in the process of community SBIRT (Screening, Brief Intervention, and Referral to Treatment) to screen for risk groups and intervene.35 We received approval from the Institutional Review Board (IRB) to conduct an analysis for public purposes. The collected questionnaire data, and among them, 115 questionnaires with missing data were excluded, there was no difference between the missing data group and the non-missing data group in age and gender characteristics. Finally, the number of samples used for analysis was 2,586.
Measure
Family history of addiction
The ACEs survey31 was designed to assess family history of addiction. The question was as follows: ‘Does anyone in your family currently have addiction problems (such as alcohol, gambling, Internet gaming, or smartphone use)?’ The respondents answered ‘yes (1)’ or ‘no (0)’ to this question. ‘Yes’ responses were summed to yield a family history of addiction score. The question was used as a tool to capture the presence or absence of a family history of addiction among ACEs.
In 2017, all questions of ACEs were implemented in the annual community project. During the analysis of the 2017 report, results with significant scores for ACEs and numbers for which frequency of ACEs were not derived were reviewed.3536 As a result, in the process of composing the questionnaire in 2018, it was agreed to reduce the question numbers after discussion among researchers. The questions about family history of addiction were constructed and measured as standard questions of ACEs. In our previous study, cronbach’s α-level was 0.767.36
Internet Game Use-Elicited Symptom Screen (IGUESS)
The IGUESS tool was used to measure the risk of IGD. The IGUESS tool is used to screen the level of IGD based on the diagnostic criteria suggested in the fifth edition of the DSM-5.37 The each questionnaire rated on a 4-point scale (0 = strongly disagree, 1 = somewhat disagree, 2 = somewhat agree, 3 = strongly agree). This scale assesses whether someone has experienced nine symptom-related experiences with Internet gaming in twelve months. The results allow the classification of respondents into high-risk and general groups. The tool consists of nine questions, and the higher score indicates greater severity of IGD.
The Pediatric Symptom Checklist-17 (PSC-17)
The PSC-17 is a psychosocial screening instrument designed to evaluate a child’s overall psychosocial functioning (attention, internalizing problems and externalizing problems).38 The PSC-17 was modified from the PSC-35 to create a shorter, adolescent self-report version. The scores of each of the 17 items are summed to calculate the total score, which ranges from 0 to 34. In this questionnaire, a sub score is generated for attention, internalizing problems, and externalizing problems. A PSC-17 score of 15 or higher suggests that significant emotional or behavioral issues are present. Scores of ≥5 indicate risk on the internalizing subscale, and scores of ≥ 7 indicated risk on the attention and externalizing subscales.39 Higher scores indicate greater risk.40
Statistical analyses
The data collected for this study were analyzed using Statistical Package for Social Science version 21.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistical analysis and χ2 tests were conducted to examine the demographic characteristics of the study subjects. Pearson correlation analysis was performed for IGD, family history of addiction and pediatric symptoms (attention, internalizing problems and externalizing problems). To verify the mediating effects of attention, internalizing problems and externalizing problems on the effects of family history of addiction on IGD, parametric modeling was performed using the SPSS PROCESS macro. Serial multiple mediation analysis was performed using bootstrapping with 5,000 replications.
Strengths and weaknesses of cross-sectional studies
Strengths of cross-sectional studies are that relatively quick, multiple outcomes and exposures can be studied, and good for descriptive analyses or for generating hypotheses.4142 However, it is important to be aware of the predictive limitations of cross-sectional studies. The primary limitation of the cross-sectional study design is that exposure and outcome are simultaneously assessed.43 It is generally no evidence of a temporal relationship between exposure and outcome. Furthermore, recall bias can occur if the study asks participants about past exposures. Nevertheless, it could provide a useful springboard to further research.4445
Ethics statement
This study was approved by the IRB of the Nowon Eulji Medical Center, Eulji University (IRB No. EMCS 2020-02-002). The study procedures were carried out in accordance with the Declaration of Helsinki. All adolescents signed for informed consent, after detailed information on the aims and course of the study.
RESULTS
Demographic characteristics
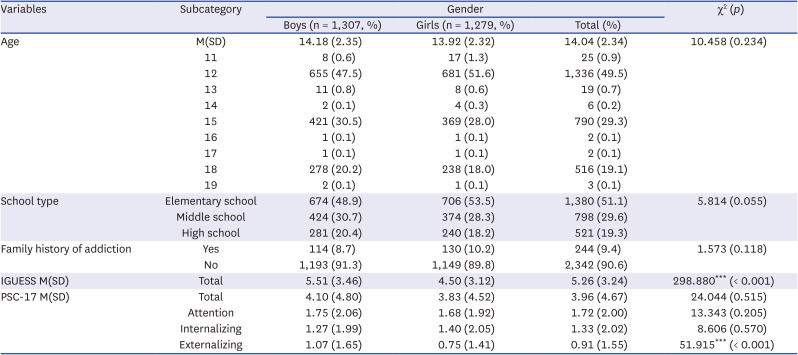
The mean age of the participants was 14.04 years (standard deviation = 2.34), and the age range was from 11 to 19 years. Among the participants, 1,307 (50.5%) were boys, and 1,279 (49.5%) were girls. A total of 1,238 participants were 12 years old (47.9%), followed by 779 participants aged 15 years old (30.1%) and 513 participants aged 18 years old (19.8%). Regarding the school type, there were 1281 elementary school students (49.5%), 787 middle school students (30.4%), and 518 high school students (20.0%). A total of 244 children and adolescents (9.4%, boys = 114, girls = 130) had been exposed to family history of addiction. Among the participants with family history of addiction, elementary school students were the most common (n = 183, 75.0%), followed by middle school students (n = 47, 19.3%) and high school students (n = 14. 5.7%). The demographic characteristics of the subjects are detailed in Table 1.
Table 1
Sociodemographic characteristics (N = 2,586)
Covariates
Possible confounding factors were obtained from the baseline data to control for the variables in the final model. The IGUESS and PSC-17 data were obtained from participant’s self-evaluations.
The results of the Pearson correlation analyses of the family history of addiction, IGUESS and PSC-17 scores
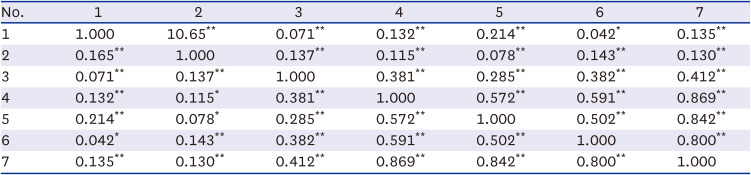
The results showed that there were significant differences in family history of addiction, IGUESS and PSC-17 scores (P < 0.05). The total PSC-17 score and attention subscale score were strongly correlated with the other subscale scores (internalizing and externalizing problems) (all P < 0.01). The results are described in Table 2.
Table 2
Person correlation coefficients between the family history of addiction, IGUESS and PSC-17 scores
Mediating effect of pediatric symptoms on the association between family history of addiction and IGD
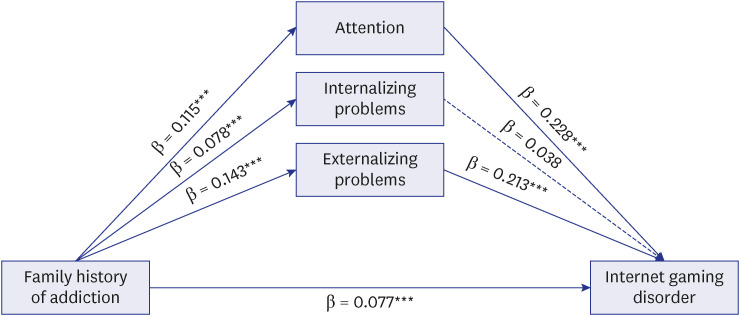
To examine whether pediatric symptoms (attention, internalizing problems and externalizing problems) had a mediating effect on the association between family history of addiction and IGD, hierarchical multiple regression analysis was performed according to the steps proposed by Baron and Kenny.46 An analysis to determine whether family history of addiction significantly predicted the mediators revealed that family history of addiction had a significant effect on attention (β = 0.115, P < 0.001), internalizing problems (β = 0.078, P < 0.001), and externalizing problems (β = 0.143, P < 0.001). In addition, family history of addiction had a significant effect on IGD (β = 0.077, P < 0.001). Subsequently, we examined the influence of the mediators on the dependent variables. Attention problems (β = 0.228, P < 0.001) and externalizing problems (β = 0.213, P < 0.001) had significant effects on IGD. This result suggests that attention and externalizing problems have a mediating effect between family history of addiction and IGD. However, internalizing problems showed no partial mediating effect (β = 0.038, P > 0.05). Furthermore, the indirect effect of the independent variable on the dependent variable through the mediators was significant (Sobel’s T: Z = -5.006, P < 0.001) (Table 3).
Table 3
Mediating effect of pediatric symptoms on the relationship between family history of addiction and IGD

We estimated the confidence interval by using the bootstrapping method proposed by Hayes.47 The number of replications for bootstrapping was 5,000. The lower and upper limits of the coefficient of the mediating effect estimated through the 95% confidence interval are presented in Table 4. The confidence interval did not include 0, indicating that attention and externalizing problems significantly mediated the effect of family history of addiction on IGD. On the other hand, the confidence interval for internalizing problems included 0, indicating that this variable did not significantly mediate the effect of family history of addiction on IGD (Table 4).
Table 4
Bootstrapping results for the indirect effects of family history of addiction, PSC-17 score and IGUESS score from PROCESS
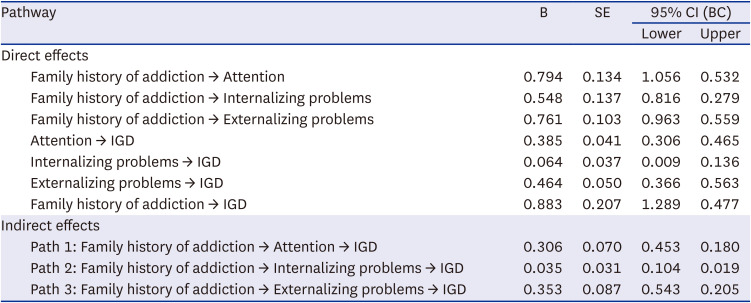
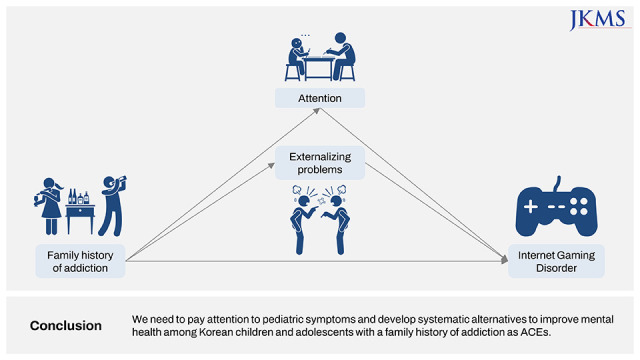
The mediation model indicated that attention and externalizing problems mediated the effect of family history of addiction on IGD. However, internalizing problems did not significantly mediate this effect. Based on these results, the final mediation model of this study is shown in Fig. 1.
DISCUSSION
The present study examined the associations among several variables that influence IGD among children and adolescents with a family history of addiction in Korea. To the best of our knowledge, our study is the first to investigate the association between a family history of addiction, IGD, and pediatric symptoms (attention, externalizing problems, and internalizing problems) in a youth population in South Korea. Additionally, we examined the mediating effects of attention, externalizing problems, and internalizing problems on the relationship between a family history of addiction and IGD.
The family history of addiction itself is one of the variables in ACEs and has been reported to be associated with trauma symptoms in various studies.21344849 Of note, it may be genetic and environmental factors at play in the relationship between a family history of addiction and IGD.50 Especially, trauma is associated with an increased risk for addiction, and this may be related to its impact on the developing brain regions, such as the prefrontal cortex and the limbic system.49515253 Trauma could cause the amygdala to become overactive, leading to enhanced emotional reactivity.5455 Trauma may also impair prefrontal cortex functions, leading to difficulty with impulse control and emotional regulation.5356 Furthermore, decreased impulse inhibition entails the disability to manage compulsive internet gaming use despite negative consequences.5758 Accordingly, trauma could disrupt brain regions’ development and function, which may have a negative consequence on social-emotional development among children and adolescents and heighten the risk of mental health issues.59
We found that attention problems mediated the relation between family history of addiction and IGD (β = −0.228, P < 0.001). A decrease in self-regulation ability is associated with addiction problems such as IGD. Therefore, addiction and attention are highly correlated.60616263 A previous study64 showed that children and adolescents with attention problems were more prone to IGD. A lack of attention is one key aspect of behavioral addiction.65 Immediate rewards and the variety of activities on the internet may provide quick rewards and decrease boredom among youth. Additionally, an earlier study showed that inattention symptoms in IGD groups were significantly more severe than those in the control group.64 In Taiwan, elementary and junior high school students (n = 1,153) were recruited for a longitudinal study, and the results showed that IGD was related to poor social adjustment, lower family support and severe ADHD-related symptoms.66 Our results are generally similar to those of a previous study suggesting that young people with a family history of addiction were more likely to report psychological symptoms and substance-related problems.67 Also the moderating resources and primary stressors contributed to the association between psychological functioning and family history of addiction.6869 These findings are in close agreement with previously published results70 showing that effective assessment and treatment for attention problems are necessary for adolescents with IGD. Therefore, our results demonstrated that IGD and attention problems might interact with each other, and that inattention may also have an influence on IGD. Therefore, in children and adolescents who are at risk for IGD, clinicians may need to focus on screening and intervention.
The current study also found that externalizing problems (β = 0.213, P < 0.001) mediated the relation between family history of addiction and IGD. IGD-related psychological risk factors include impulsivity and low self-control.24 Externalizing problems and strong emotions such as excitement and powerfulness from online gaming could promote excessive gaming disorder.54 Our results are similar to those of a prior study71 in which individuals with a high level of aggression had a higher tendency for internet addiction. The results of the present study are consistent with previous results suggesting that IGD is associated with externalizing problems in youths and causes mental health issues, such as anxiety, among both youths and parents.72 As more time is spent on online gaming, ‘real-world’ social relationships tend to deteriorate, and the lack of ‘real-life’ social relations could lead youth with IGD to develop symptomatology.73 Furthermore, external factors such as intra familial violence and deficient social skills could increase the risk of developing IGD.74
This finding showed that internalizing problems (β = 0.038, P > 0.05) did not mediate the relation between family history of addiction and IGD. Impulse control symptoms are mainly caused by problems of the prefrontal cortex, which are related to attention and externalizing problems.757677 It is possible that the family history of addiction measured in this study influenced external behavior through social modeling rather than affecting affection problems. In our recently published study,26 we used all 10 items on ACEs and reported that ACEs affected IGD by mediating internalizing symptoms. The reason for the difference between the results of the previous study and the current study was that the participating group was a community sample, and ACEs were measured using one item and modeled to include attention and externalizing symptoms.
In the final model in this study, we showed that attention and externalizing problems mediated the relation between a family history of addiction and IGD. This finding suggests that a family history of addiction as an ACE may be a higher risk for developing IGD. However, IGD is a highly heterogeneous condition and depends on a wide range of psychological factors.54 Individual factors might be related to the increased risk of developing IGD.78 Therefore, it is important to understand individual psychological factors to plan therapeutic interventions. Furthermore, it is necessary to study these factors separately to conduct research related to IGD.
Some limitations of our study must be considered. In the present study, one community sample was investigated. Therefore, it remains unclear whether our results can be generalized to the general population. In addition, family history of addiction (ACEs measures) was not gathered with a full questionnaire; it did not accurately capture each adverse experiences of participants. As a result, this Family history of addiction should be considered an indicator of potential ACEs. Although our study found relationships between family history of addiction as an ACEs and IGD, more research on the mechanisms of these relationships is needed. Finally, our data was a cross-sectional analysis, thus, it could not determine causation or directionality. Therefore, further prospective study should be performed to prove the association between a family history of addiction, IGD, pediatric symptoms among children and adolescents.
This study demonstrated the associations among family history of addiction as an ACEs, IGD, and pediatric symptoms (attention, externalizing problems and internalizing problems) among Korean children and adolescents. We found that the family history of addiction among children and adolescents had an effect on IGD, and attention and externalizing problems had a mediating effect. Therefore, we need to screen the Korean children and adolescents exposed to ACEs and develop effective preventive intervention models.
 XML Download
XML Download