

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In January 2020, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first detected as the cause of coronavirus disease (COVID-19).12 Since then, SARS-CoV-2 has continuously evolved and spread. On November 26, 2021, the World Health Organization (WHO) defined variant B.1.1.529, more commonly known as omicron, as a variant of concern.3 Since it was reported, omicron has driven a surge of infection worldwide due to its high transmissibility.456 After the first case of omicron in Korea was detected on November 30, 2021, the variant rapidly outpaced Delta as the dominant variant in Korea.789 Furthermore, in the first week of September 2022, the highly contagious and immune-resistant BA.5 variant became the dominant subvariant in South Korea (97.1% of newly reported infections).10
The risk of hospitalization and death in patients with COVID-19 infected with the omicron variant has declined compared to those infected with the Delta (B.1.617.2) variant, and symptoms are less severe.111213 Despite its milder symptoms, those who are unvaccinated, with chronic health conditions affecting their immune system, and those aged ≥ 60 years are still at high risk of serious complications.1415
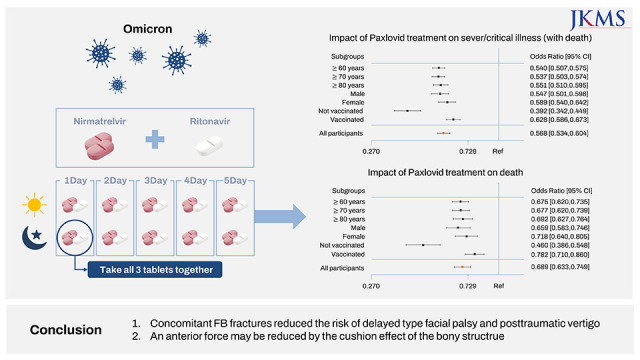
Recently, several oral antiviral drugs have been reported to reduce hospitalization, block the progression of disease, and reduce mortality in high-risk patients with COVID-19, including patients infected with the omicron variant.161718192021 The first oral treatment, nirmatrelvir and ritonavir (Paxlovid), was approved for emergency use in Korea on December 27, 2021, after reviews of the safety and effectiveness from the Ministry of Food and Drug Safety. On January 14, 2022, Paxlovid was administered first to patients with COVID-19 with mild-to-moderate symptoms who were at high risk of progressing to severe disease within 5 days of symptom onset, receiving at-home treatment or treatment at a residential facility center. A recent clinical report and retrospective analysis indicated that a 5-day dose of Paxlovid reduced the risk of death and hospitalization1622232425; however, these studies did not fully demonstrate its benefit in SARS-CoV-2 BA.5 infection, although they were performed during the omicron surge. There is a need to investigate the effectiveness of Paxlovid in the treatment of older patients with COVID-19 with the BA.5 variant. In this study, we conducted a retrospective cohort study to analyze the effectiveness of Paxlovid at reducing the severity and mortality of COVID-19 during the BA.5 wave as it became dominant in South Korea.
Go to : 
METHODS
Sources of data
This study analyzed data from four sources: the Drug Utilization Review (DUR) database, COVID-19 Patient Information Management System data from the Health Insurance Review and Assessment Service, confirmed patient information, and basic epidemiological investigation data from the COVID-19 Information Management System of the Korea Disease Control and Prevention Agency (KDCA). The database managed by the KDCA contained the results of the SARS-CoV-2 polymerase chain reaction diagnostic test, underlying diseases, and vaccination status. The DUR database contained prescription information regarding oral antivirals for COVID-19. The COVID-19 Patient Information Management System data contained medical history, including critical severity and death.
Study population
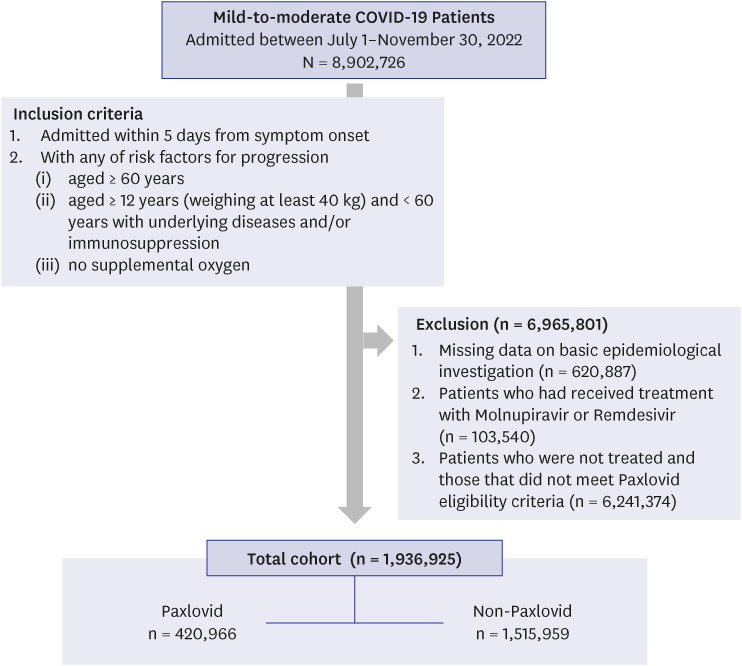
The study comprised 8,902,726 patients who contracted COVID-19 between July 1 and November 30. Paxlovid (given two times each day for 5 days) was considered for treatment of patients with mild-to-moderate COVID-19 who were at high risk for progression to severe illness, including hospitalization or death. KDCA recommends the use of Paxlovid in published COVID-19 treatment guidelines26 as follows: 1) aged ≥ 60 years, 2) aged ≥ 12 years (weighing at least 40 kg) and < 60 years with underlying diseases and/or immunosuppression, and 3) within 5 days of symptom onset and no supplemental oxygen. The inclusion criteria of the present study were as follows: 1) Koreans diagnosed with COVID-19 and reported to KDCA between July 1, 2022 and November 30, 2022; 2) aged ≥ 12 years; 3) contracted COVID-19 and were prescribed Paxlovid within 5 days of symptom onset; and 4) untreated patients who met the same study eligibility criteria as described in the Paxlovid guidelines. The exclusion criteria were: 1) missing data on basic epidemiological investigation; 2) patients who had received treatment with Molnupiravir or Remdesivir; 3) patients aged < 12 years; 4) patients who did not meet the Paxlovid eligibility criteria.
For each patient, follow-up monitoring ended 28 days after diagnosis of COVID-19 at the earliest. Patients with COVID-19 who were residing in homes, long-term care facilities, and convalescent hospitals were included.
Study outcomes
Disease severity for severe and critical COVID-19 was defined using the WHO COVID-19 clinical management guidelines.27 The severity ratio referred to patients with severe and life-threatening illness and those who died. COVID-19 death was defined when COVID-19 was reported as a cause of death or as “probable” or “presumed” on the death certificate. The study evaluated the effectiveness of Paxlovid for reducing the risk of severe/critical illness or death, and death in patients with COVID-19.
Patients were categorized according to their vaccination status (unvaccinated or vaccinated, regardless of the number of doses), age (≥ 60 years, ≥ 70 years, or ≥ 80 years, respectively), and sex (male or female).
Statistical analysis
Descriptive statistics (number and percent) were calculated to described the characteristics of study participants and to compare the untreated, Paxlovid-treated, unvaccinated, and vaccinated groups. The chi-square test was used to compare categorical variables. Multivariable logistic regression was performed to assess the risk of severe/critical disease and death in patients with COVID-19 according to their Paxlovid treatment status (treated/not treated), adjusting for age, sex, underlying conditions, and vaccination history. All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Statistical tests were two-sided, and P values < 0.05 were considered statistically significant.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of the Korean National Institute of Health and the requirement for informed consent waived (approval No. 2022-12-02-PE-A).
Go to :
RESULTS
Study population characteristics
During the nationwide retrospective cohort study period, 8,902,726 patients with mild-to-moderate COVID-19 enrolled in the DUR system for COVID-19 patient care were screened. After excluding 6,965,801 patients, 1,936,925 patients who were eligible for treatment with Paxlovid were included (Fig. 1). The patients were classified into a Paxlovid treatment group (n = 420,966), and an untreated (control) group (n = 1,515,959).
Among the 420,996 (21.7%) patients who received Paxlovid, 377,531 (89.6%) were aged ≥ 60 years. In the older age group, there were notably more patients aged between 60–69 years (41.3%) than those of other ages. The most common coexisting underlying diseases were hypertension (170,840; 40.6%), hyperlipidemia (89,014; 21.1%), and diabetes (85,766: 20.4%). Among 1,515,959 (78.3%) patients who were not treated with Paxlovid, 1,117,811 (73.8%) were aged ≥ 60 years. The number of patients aged between 60–69 years who did not take drugs was notably higher (636,485; 42.0%). The most common coexisting conditions in the untreated group of this age were also hypertension (703,095; 46.4%), hyperlipidemia (381,339; 25.2%), and diabetes (333,529; 22.0%). Overall, over 95% of the patients included in the analysis had received at least one dose of SARS-CoV-2 vaccine (Table 1). The sex, age, SARS-CoV2 immunity, underlying disease (and number of underlying diseases), severe/critical illness or death, and death differed significantly according to Paxlovid treatment status.
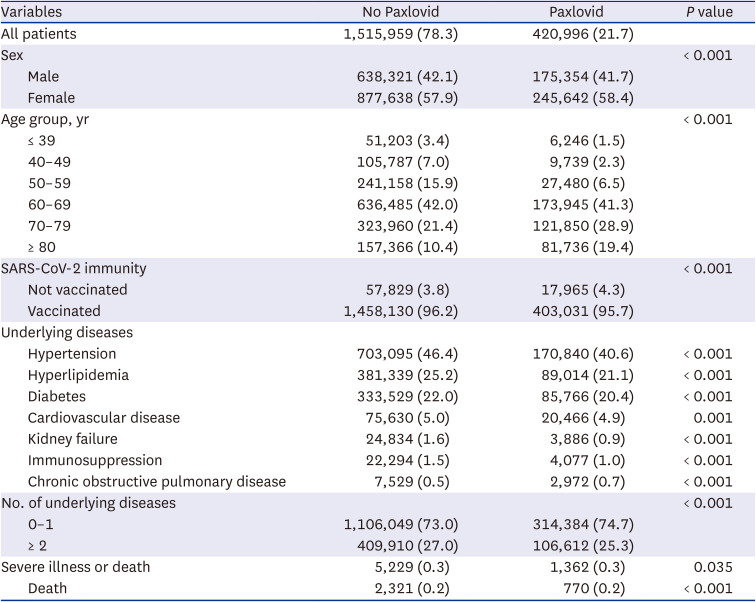
Table 1
Baseline patient characteristics according Paxlovid treatment status
Data are expressed as numbers and percentages (%) unless otherwise indicated. χ2 tests were used to determine differences between the non-Paxlovid and Paxlovid treatment.
![]()
Effectiveness of Paxlovid
Multivariable logistic regression was performed to assess the effect the Paxlovid on severe/critical illness or death, and death. The risk of these outcomes was lower in the Paxlovid treatment groups compared with the untreated group, regardless of their age, sex, and vaccination status (Table 2, Figs. 2 and 3).

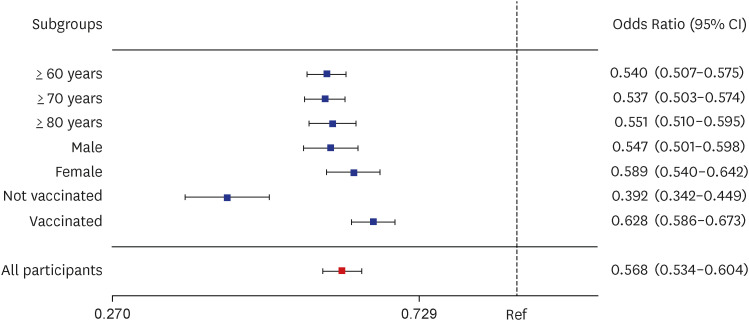 | Fig. 2Impact of Paxlovid treatment on severe/critical illness (with death) at subgroups. Multivariable logistic regression models were adjusted for age, sex, severe acute respiratory syndrome coronavirus 2 immunity (vaccination) and underlying diseases. Data are expressed as odds ratios (95% CIs).CI = confidence interval.
|
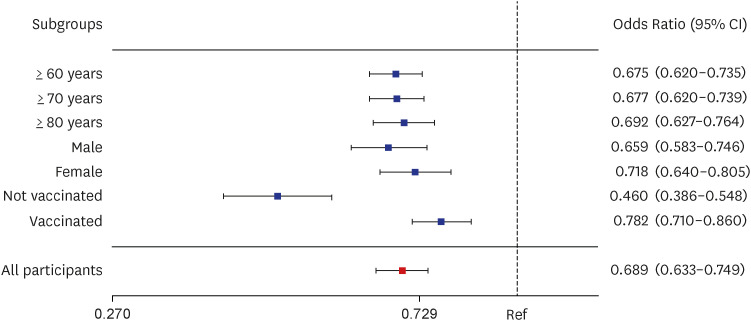 | Fig. 3Impact of Paxlovid treatment on death at subgroups. Multivariable logistic regression models were adjusted for age, sex, severe acute respiratory syndrome coronavirus 2 immunity (vaccination) and underlying diseases. Data are expressed as odds ratios (95% CIs).CI = confidence interval.
|
Table 2
Effect of Paxlovid treatment on severe/critical illness or death and death in patients with coronavirus disease 2019
The results are expressed as odds ratios (95% confidence intervals).
Model 1: non-adjusted. Model 2: adjusted for age and sex. Model 3: Model 2 + vaccination and underlying disease.
![]()
In subgroup analyses stratified by age, sex, and vaccination status, the risk of severe/critical illness or death was significantly lower in the Paxlovid treatment group compared with the untreated group. The adjusted odds ratio [OR] (95% confidence interval [CI]) for the total population receiving Paxlovid treatment was 0.568 (0.534–0.604). In older adults, the OR was 0.540 (0.507–0.575) for those aged ≥ 60 years, 0.537 (0.562–0.690) for those aged ≥ 70 years, and 0.551 (0.510–0.595) for those aged ≥ 80 years. The ORs (95% CIs) in men and women were 0.547 (0.501–0.598), and 0.589 (0.585–0.642), respectively. The ORs (95% CIs) in unvaccinated and vaccinated patients were 0.392 (0.342–0.449) and 0.628 (0.586–0.673), respectively.
The risk of death was significantly reduced in the aged and unvaccinated groups, but was not significantly reduced in the female and vaccinated groups. The adjusted ORs (95% CIs) were 0.689 (0.633–0.749) for all Paxlovid-treated patients. In older adults, the ORs (95% CIs) were 0.675 (0.620–0.735) for those aged ≥ 60 years, 0.677 (0.620–0.739) for those aged ≥ 70, and 0.692 (0.627–0.764) for those aged ≥ 80 years. The ORs (95% CIs) in men and women were 0.659 (0.583–0.746) and 0.718 (0.640–0.805), respectively. The ORs (95% CIs) in unvaccinated and vaccinated patients were 0.460 (0.386–0.548) and 0.782 (0.710–0.860), respectively.
Go to :
DISCUSSION
This retrospective cohort study of the Korean population showed that Paxlovid treatment within 5 days after COVID-19-related symptom onset in patients aged ≥ 60 years was associated with a significant reduction in the risk of progression, development of severe/critical illness, and risk of death, compared with non-treated patients.
The reduction in the risk of severe illness in the Evaluation of Protease Inhibition for Covid-19 in High-Risk Patients (EPIC-HR) trial was larger (89% of patients with mild-to-moderate COVID-19)1628; in comparison, this study showed less effective risk reduction (43.2%) than in that trial. This might be explained by several differences between the studies, including differences in virus genotypes, vaccination status, study design, and the quality of the data from clinical and administrative databases. Importantly, in the EPIC-HR trial, the dominant variant was the Delta strain, including clades 21J, 21A, and 21I,29 whereas the current study was conducted during a period when the dominant variant was omicron BA.5, including clades BA.2.3 and BA.2.1030 In the EPIC-HR trial, all patients were adults who were unvaccinated against COVID-19 who had also never previously contracted the disease. Our study include vaccinated and previously infected patients as the vaccination rate in Korea was over 90% during the study period.31
COVID-19 vaccines, including mRNA-1273 (Moderna) and BNT162b2 (Pfizer-BioNTech), are associated with a reduced risk of SARS-CoV-2 infection and COVID-19 hospitalization32333435; however, these benefits could also contribute to underreporting the effect sizes of drugs, including severe/critical illness and death. Our subgroup analysis based on vaccination showed a greater Paxlovid treatment effect in the unvaccinated group than in the vaccinated group. Further studies should be conducted on the association between prior vaccination and the therapeutic effectiveness of drugs in reducing disease progression. Furthermore, COVID-19 vaccination is a key strategy to reducing the risk of severe COVID-19-related illness or death, particularly among older adults. In addition, booster vaccination is important for enhancing the effectiveness of COVID-19 vaccination. The government recommends booster doses of COVID-19 vaccines, and a large proportion of the population have received a booster dose. Although vaccination history is an important factor to be considered in analyzing severity and mortality, the information available on patients’ vaccination history, including booster vaccination and the number of doses of vaccine received, was insufficient, so we were unable analyze the data according to booster vaccination status or the number of doses of vaccine received in this study. In this study, we considered only whether the patient had received at least one doses of vaccine before the onset of COVID-19.
The study has some limitations. First, we could not determine whether patients completed the 5-day course of Paxlovid treatment. Therefore, patients who did not complete Paxlovid treatment may have been included in the treated group. Second, although adaptive immune responses are important, we did not consider patients’ history of previous infection. Third, we did not consider the time from symptom onset to COVID-19 diagnosis, or the time from symptom onset to prescription of Paxlovid. Fourth, other treatment (such as the administration of steroids) was not considered.
In conclusion, this is the first report to analyze real-world data in Korea to assess the effectiveness of Paxlovid as a treatment to prevent COVID-19 progression in patients infected with the omicron variant. Treatment with Paxlovid was associated with a marked reduction in disease progression and death among patients infected with the omicron variant, especially in older adults, and those who had not been vaccinated. Therefore, we suggest that older patients who have COVID-19-related symptoms should be administered Paxlovid, regardless of their vaccination status. Rapid administration of this drug to patients at risk will contribute to reducing the severe/critical illness or death and death rate, and help to control the COVID-19 pandemic.
Go to :
 XML Download
XML Download