

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Congenital heart disease (CHD) is present in approximately 1% of births.1 The survival rate of patients with CHD has improved dramatically in recent decades and is currently estimated to be > 90%.234 As the number of long-term survivors has increased, CHD-related comorbidities have become an emerging issue in affected patients.35
Growth retardation (GR) can arise in children with CHD. This is because infants with CHD have higher rates of low birth weight or small for gestational age (SGA) than healthy newborns.678 Children with CHD also have a higher rate of nutritional deficiencies and increased metabolic demands, which lead to GR.910
METHODS
Study population
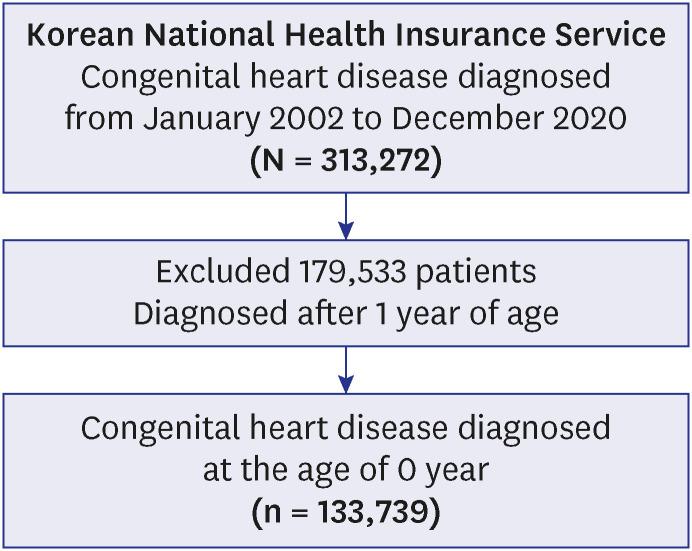
The Korean National Health Insurance Service (NHIS) claims data from January 2002 to December 2020 was used to extract the study population. CHD diagnoses were based on the International Classification of Disease, Tenth Revision (ICD-10). We included patients diagnosed with CHD under one year of age. All newborns born in Korea receive benefits from the Korean NHIS, which contains the medical information for all newborns from birth. The study flowchart is shown in Fig. 1.
Neonatal conditions for analysis
Neonatal conditions were defined based on ICD-10 codes. The potential neonatal risk factors for GR selected were twins, preterm birth, birth asphyxia, SGA, large for gestational age (LGA), low birth weight, respiratory distress, neonatal aspiration syndrome, bronchopulmonary dysplasia (BPD), congenital viral disease, bacterial sepsis, intracranial hemorrhage, neonatal jaundice, and necrotizing enterocolitis (NEC). And referring to the existing literature,31415 we classified cases of CHD into three groups according to their complexity, namely, simple, moderate, and complex; these groups were analyzed for their effects on GR. In addition, we classified cardiac procedure into non-complex and complex, and then we also investigated the impact of cardiac procedure on GR. The ICD-10 codes for neonatal conditions are summarized in Supplementary Table 1.
Growth retardation
GR was defined as a height impairment and data were extracted based on ICD-10 code for patients diagnosed with idiopathic growth hormone deficiency (E23) or short stature (E34) from NHIS claims data. A diagnosis of idiopathic growth hormone deficiency is made when the growth hormone level is < 10 ng/mL in at least two growth hormone stimulation tests.16 Short stature is defined as a height < 2-standard deviations for age and gender, with no structural or functional cause.17 We examined the potential risk factors for GR among neonatal CHD patients.
Statistical analysis
Continuous variables were described as the mean ± standard deviation or median with interquartile range, and categorical variables as counts with percentages. Student’s t-test or the Mann–Whitney U test was used for continuous variables, and χ2 or Fisher’s exact tests were used for categorical variables. The cumulative incidence of GR was calculated using the competing risk method, with any death event regarded as a competing risk. Gray’s test was used to estimate differences in the cumulative incidence among the groups. Variables from univariable models with P < 0.2 were selected for the multivariable model. Statistical significance was set at P < 0.05. Statistical analyses were conducted using R software (www.r-project.org).
RESULTS
Selection of study population
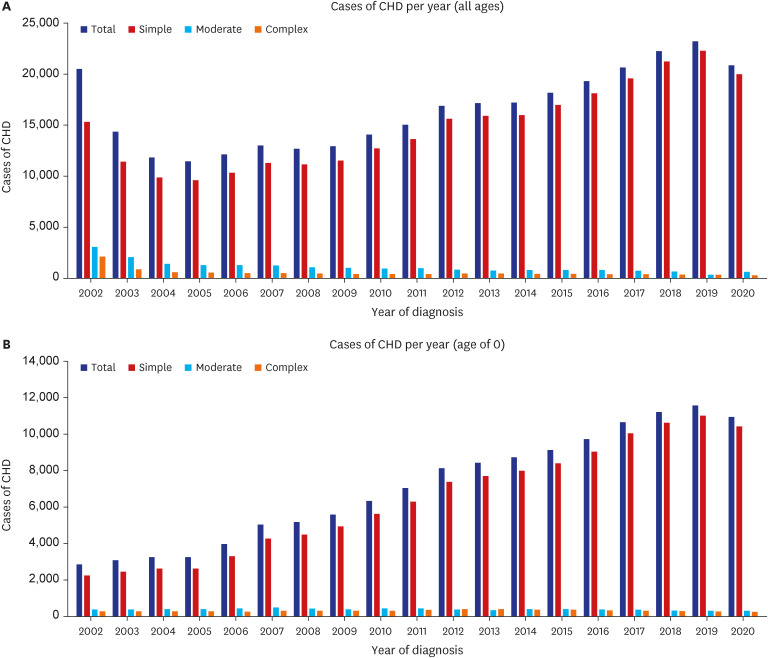
From 2002 to 2020, 313,272 patients were diagnosed with CHD (Fig. 1) and classified according to the complexity of the CHD diagnosis: 282,140 (90.1%), 20,835 (6.7%), and 10,296 (3.3%) patients were classified as having simple, moderate, and complex CHD, respectively. After excluding patients diagnosed with CHD after one year of age, 133,739 patients diagnosed with CHD within the first year of their birth were included in our analyses. Among these, 121,112 (90.6%), 7,010 (5.2%), and 5,617 (4.2%) were classified as having simple, moderate, and complex CHD, respectively. Fig. 2 illustrates the number of patients diagnosed with CHD per year.
Baseline characteristics
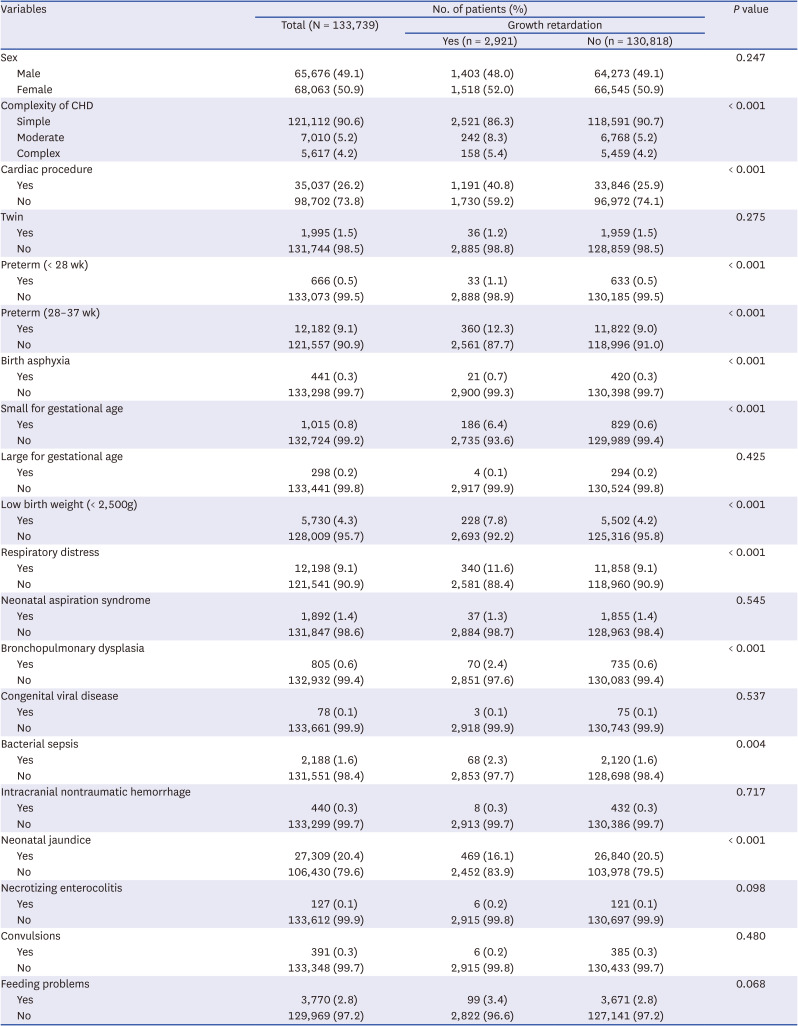
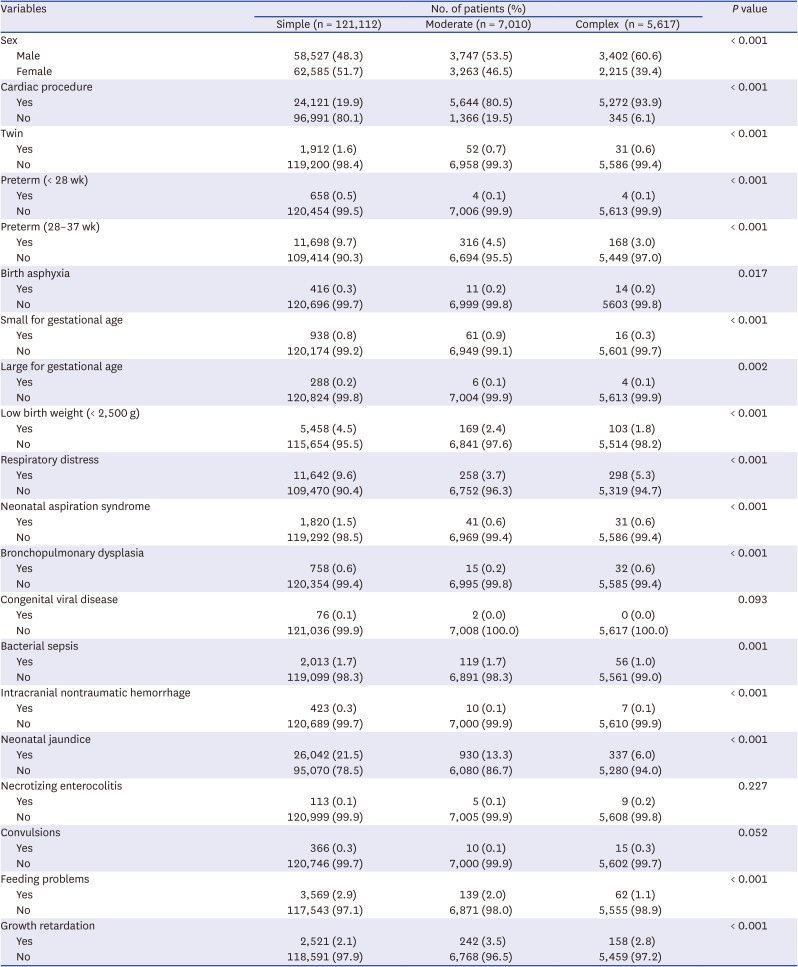
We enrolled 133,739 infants diagnosed with CHD younger than one year of age. The baseline patient characteristics are shown in Table 1. And the number of patients corresponding to each CHD diagnoses is attached in Supplementary Table 2. Within the study population, 2,921 newborns were diagnosed with GR. The proportion of patients with moderate and severe CHD was significantly higher in the GR group than those in the non-GR group (P < 0.001). The rate of cardiac surgery was also significantly higher in the GR group than in the non-GR group (40.8% vs. 25.9%; P < 0.001). The number of patients who underwent complex cardiac procedure is presented in Supplementary Table 3. Moreover, the proportions of premature births (< 28 weeks, 1.1% vs. 0.5%; 28–37 weeks, 12.3% vs. 9.0%; both P < 0.001), birth asphyxia (0.7% vs. 0.3%; P < 0.001), SGA (6.4% vs. 0.6%; P < 0.001), low birth weight (7.8% vs. 4.2%; P < 0.001), respiratory distress (11.6% vs. 9.1%; P < 0.001), BPD (2.4% vs. 0.6%; P < 0.001), bacterial sepsis (2.3% vs. 1.6%; P = 0.004), and neonatal jaundice (16.1% vs. 20.5%; P < 0.001) were significantly between GR and non-GR groups.
Table 1
Baseline characteristics
Growth retardation and neonatal conditions by CHD complexity
The characteristics according to CHD complexity are shown in Table 2. The rates of cardiac surgery for simple, moderate, and complex CHDs were 19.9%, 80.5%, and 93.9%, respectively (P < 0.001). The proportions of GR diagnoses were 2.1%, 3.5%, and 2.8% for simple, moderate, and complex CHD, respectively (P < 0.001). The neonatal conditions among the three groups were significantly different in terms of twins and preterm births, birth asphyxia, SGA, LGA, low birth weight, respiratory distress, neonatal aspiration syndrome, BPD, sepsis, intracranial nontraumatic hemorrhage, jaundice, and feeding problems.
Table 2
Clinical characteristics according to complexity of congenital heart disease
Cumulative incidences of growth retardation by CHD complexity and neonatal conditions
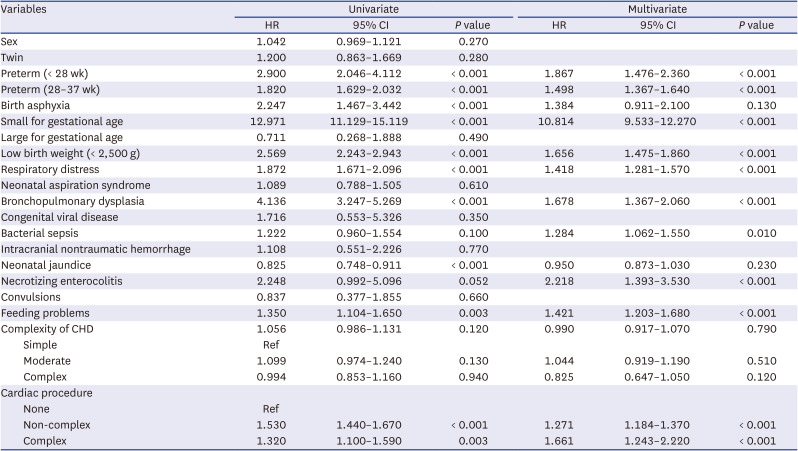
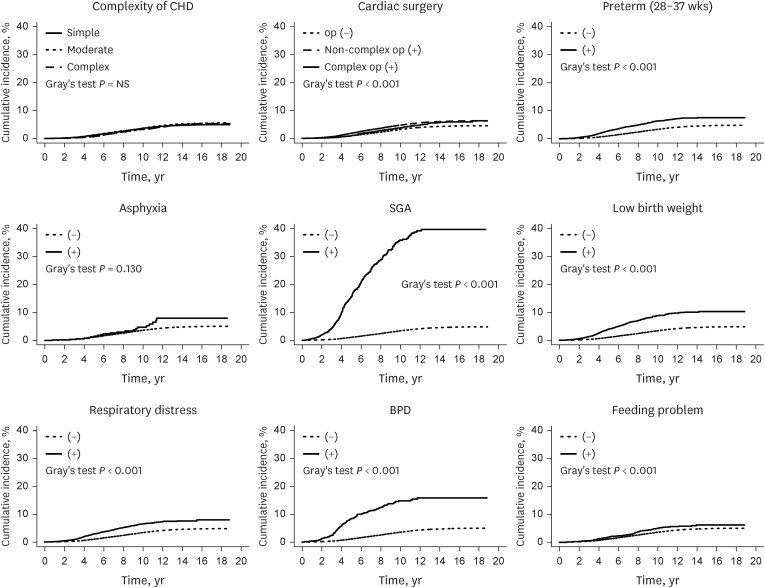
The cumulative incidence of GR at 19 years old age with diagnoses of CHD at infancy was 4.8% (Fig. 3). Table 3 summarizes the hazard ratios of different variables in the univariate and multivariate analyses, which were used to determine the risk factors for GR. In the univariate analysis, the significant neonatal conditions affecting the cumulative incidence of GR were any preterm birth, birth asphyxia, SGA, low birth weight, respiratory distress, BPD, jaundice, feeding problems, and cardiac procedure. In the multivariable analysis, the statistically significant risk factors for GR were any preterm birth, SGA, low birth weight, respiratory distress, BPD, bacterial sepsis, NEC, feeding problems and cardiac procedure. CHD complexity did not significantly affect the development of GR in the multivariate analysis (Fig. 4). In addition, we investigated whether there was a difference in GR according to complexity of cardiac procedure, but there was no significant difference.
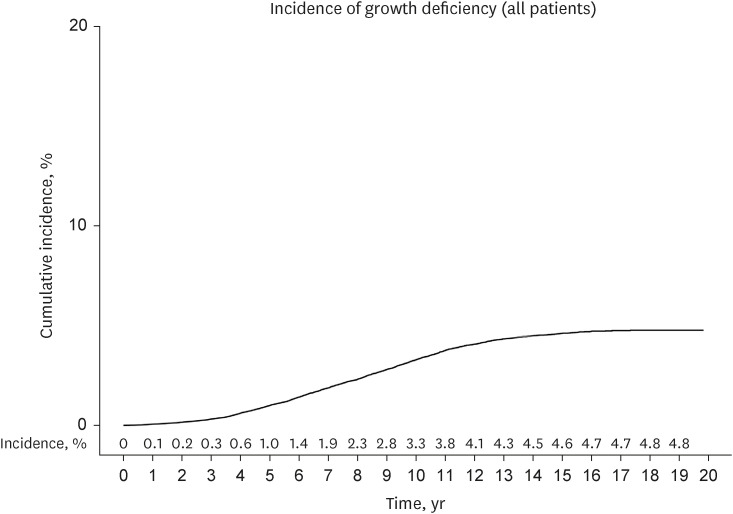
Table 3
Univariate and multivariate analysis for a cumulative incidence of growth retardation
DISCUSSION
In this study, we used the Korean NHIS claims data to investigate the incidence of GR in patients with CHD based on neonatal conditions. A height impairment was considered to be GR, defined as an idiopathic growth hormone deficiency or short stature. In patients with CHD aged < one year, the cumulative incidence of GR development over 19 years was 4.8%. In multivariate analysis, the significant risk factors for GR among the different neonatal conditions assessed were any preterm birth, SGA, low birth weight, respiratory distress, BPD, bacterial sepsis, NEC, feeding problems and cardiac procedure. Contrary to what was expected, CHD complexity was not a significant risk factor for GR and there was no difference according to complexity of cardiac procedure.
Newborns with CHD are more likely to have been born as SGA than general neonates.61819 Even after birth, cardiac lesions, the general condition of the patient, and other associated factors can lead to persistent weight, height, and head circumference growth problems.9101113 In particular, studies have reported that while the infant’s weight may gradually increase with age after birth, while height does not catch up well compared to weight.920 The causes of GR in patients with CHD are multifactorial.910 Increased metabolic demand, insufficient calorie intake, and feeding difficulty are important factors that may cause GR.910 Additionally, cardiac lesions, genetic factors, and hormonal changes may also play a role.91021
Growth hormone deficiency is known to have a close relationship with cardiovascular disease.22232425 Impairment of the GH/IGF-1 axis is a key mechanism that increases the risk of cardiovascular disease in growth hormone deficiency.222324 IGF-1 has the function of improving myocardial contractility and delaying cardiomyocyte apoptosis.2226 And it has been reported that myocardium and vessels have more GH receptor genes than other tissues, so GH has a direct effect on the heart and vessels.2728 The patients of growth hormone deficiency are at increased risk of cardiovascular disease and heart failure due to increases in body fat and insulin resistance, hypertriglyceridemia.22 In addition, growth hormone deficiency increases systemic vascular resistance, decreases nitric oxide production, and affects the sympathetic nervous system.24 It has been reported that young adults with growth hormone deficiency have decreased LV ejection fraction, stroke volume index, and cardiac index, and that GH treatment has a positive effect on the recovery of this decline in cardiac function.2930 Paajanen et al.31 also reported that short stature increased cardiovascular morbidity and mortality. These influences of GR on cardiovascular disease will not be different for CHD patients, and may be more vulnerable. Therefore, GR in patients with CHD has the potential to influence the surgical outcome and prognosis of the CHD.9 And growth hormone therapy for CHD patients with GR may reduce the risk of cardiovascular disease. In this study, the percentage of diagnosed GR increased most sharply between the ages of 5 and 12 years. At age five, 1% of CHD patients were diagnosed with GR, at age ten, 3.3%, and at age twelve, 4.1%. So, it seems that the number of CHD patients diagnosed with GR is the most, especially between the ages of five and twelve. Patients with CHD have a much higher risk of comorbidities, such as cardiovascular disease, than the general population; therefore, GR is an important factor to be considered for the long-term prognosis of CHD patients, and appropriate monitoring and treatment strategies are essential.3911
This study investigated the incidence of GR in patients with CHD using large-scale population-based data. Several neonatal conditions were found to be significant risk factors for future height impairment in patients with CHD diagnosed under the age of one. The cumulative incidence of height impairment in patients with CHD by 18 years of age was 4.8%. Among the neonatal conditions assessed, SGA was determined to be the most potent risk factor for GR. Since the proportion of SGA in patients with CHD is approximately 15%, which is higher than that of the general population; careful attention and monitoring for GR is therefore necessary for patients with CHD born SGA.618 NEC is also a significant risk factor for GR. It is known that NEC can occur in 1.6% to 6% of full-term infants with CHD.32 Bowel hypoperfusion and ischemia have been suggested as mechanisms that increase the risk of NEC in CHD patients.32 The complexity of CHD and cardiac surgery have been reported as risk factors, and also still controversial, there are studies on the association between the use of prostanglandin or enteral feeding, and NEC in patients with CHD.32333435 Since CHD increases the risk of NEC due to its pathophysiology and it is also associated with GR in the future, special attention to NEC in CHD patients will be needed. In addition, respiratory problems, such as BPD and respiratory distress, low birth weight, preterm births (28–37 weeks), feeding problems, and cardiac surgery were determined to be risk factors for GR.
Contrary to our expectations, CHD complexity was not a significant risk factor for GR. The GR rates were 2.1%, 3.5%, and 2.8% for simple, moderate, and complex CHD, respectively (Table 2). The incidence of GR in the complex CHD group was lower than that in the moderate CHD group. The low survival probability in patients with severe CHD may have led to the low incidence of GR. To confirm this, we analyzed the incidence of GR by adjusting for the risk of death as a competing risk factor. While CHD complexity was not a risk factor for GR, cardiac procedure affected the incidence of GR. In other words, regardless of cardiac complexity, the risk of GR was significantly higher in patients with CHD requiring cardiac procedure than in those with a mild form of CHD not requiring cardiac procedure. Moreover, although complex cardiac surgery had a higher HR for NEC than non-complex cardiac surgery, the difference was not statistically significant (Fig. 4). Although cardiac procedure is a risk factor for GR in patients with CHD, the effect of complexity of cardiac procedure was not confirmed within the procedure group. It is presumed that there was an influence of the relatively small number of patients who underwent complex cardiac surgery and unknown confounding variables, and further research is needed on this in the future.
In patients with CHD, GR development may also be closely related to the risk of subsequent cardiovascular diseases.92223242531 Therefore, appropriate strategies for the management of long-term cardiovascular complications are needed to improve the progress of GR in patients with CHD. Due to their increased caloric requirements and frequent feeding difficulties, specialized nutrition programs are required for patients with CHD.10 In addition, by identifying the risk factors for GR, early interventions such as hormone therapy may be helpful for high-risk patients diagnosed with GR through close-monitoring. Further investigations are warranted to develop effective treatment strategies for GR in patients with CHD.
This study had several limitations. First, this was a retrospective study, increasing the likelihood of an information bias. The primary outcome of this study was height impairment, and idiopathic growth hormone deficiencies and short stature were the target diseases. However, the diagnostic criteria for idiopathic growth hormone deficiency and short stature may differ depending on the clinician. Second, the classification criteria for CHD complexity were based on the diagnostic codes in the claims data. These diagnostic codes may bias the clinical severity of CHD. In addition, although we classified CHD complexity based on the previous literature, CHD is a very heterogenous disease. Even within the same complexity, the pathophysiology of each CHD may be different, and the effect on GR may also be different. Third, we cannot exclude the possibility that some confounding variables such as genetic and environmental factors may affect GR. We were unable to include factors that were most likely to affect GR, such as parental height or nutritional status, BMI. These variables are important factors that can affect GR, and additional studies including these variables are needed in the future.
Several neonatal conditions were significant risk factors for GR in CHD patients, and appropriate monitoring and treatment programs are required in CHD neonates with these factors. Considering this study is limited to claims data, further studies are warranted, including genetic and environmental factors affecting GR in CHD patients.
 XML Download
XML Download