

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With the outbreak of the coronavirus disease 2019 (COVID-19) across the world, vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have achieved accelerated clinical development to alleviate the burden of COVID-19 on public health. More than 11 billion SARS-CoV-2 vaccine doses have been administered in the world.1 According to World Health Organization statistics,2 the protein subunit vaccine has become the predominant category (accounting for 32% of all vaccines), followed by the RNA-based vaccine (23%), the non-replicating viral vector (14%), and the inactivated virus (12%).
Considering the unprecedented health burden induced by the COVID-19 pandemic, most vaccines have received emergency use authorization, though they have not been extensively whetted for their possible adverse effects. Therefore, public concerns over the possible adverse effects of these vaccines have emerged. A series of reports about autoimmune/inflammatory diseases induced by SARS-CoV-2 vaccines have attracted more and more attention, such as Graves’ disease,3 autoimmune hepatitis,456 systemic lupus erythematosus,7 and so on. Fulminant type 1 diabetes (FT1D) is a rapidly progressing and severe subtype of type 1 diabetes (T1D) with high mortality and disability rate. Recently, several cases have been reported about new-onset FT1D following SARS-CoV-2 vaccination, but only limited to mRNA vaccine891011 and inactivated vaccine.12 Up to now, no cases have been reported about FT1D followed by SARS-CoV-2 protein subunit vaccination.
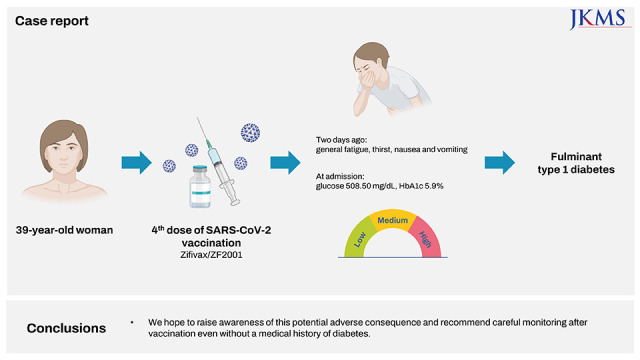
Herein, we reported a 39-year-old Chinese woman with new-onset FT1D four days after SARS-CoV-2 protein subunit vaccination. Meanwhile, we conducted a systematic review on the comparison between FT1D and autoimmune T1D followed by SARS-CoV-2 vaccination, so as to gain a better understanding of SARS-CoV-2 vaccine-related FT1D. We highly acknowledge the importance and benefits of mass SARS-CoV-2 vaccination, but we still hope to raise public awareness of its possible adverse effects and attach importance to the pharmacovigilance in guiding treatment.
CASE DESCRIPTION
We reported a 39-year-old woman with a family history of diabetes. She had no medical history of diabetes and the fasting blood glucose from her annual physical examination report seven weeks ago was 104.4 mg/dL. She attended a nearby hospital six days after the fourth dose of SARS-CoV-2 vaccination (Zifivax/ZF2001, Protein subunit vaccine) and complained of general fatigue, thirst, nausea and vomiting for 2 days. At presentation, the laboratory tests reported hyperglycemia (plasma glucose: 508.50 mg/dL) and ketoacidosis with a decreased bicarbonate and an increased anion gap (anion gap = [Sodium – {Bicarbonate + Chloride}] = 18.23 mmol/L, normal range ≤ 16 mmol/L). It was worth noting that the onset hemoglobin A1c (HbA1c) (5.9%) was below the threshold of diabetes. Pancreatic enzymes and thyroid function were normal. The initial diagnoses were diabetes and diabetes ketoacidosis (DKA). Then she received massive fluid infusion and intravenous insulin infusion and her symptoms relieved during a 10-day hospitalization in the nearby hospital.
Ten days later, she was transferred to our hospital due to poor blood glucose control and hoped for a definite diagnosis. On admission, her body mass index (BMI) was 17.97 kg/m2. Oral glucose tolerance test showed exhaustion of endogenous insulin secretion (fasting C-peptide: 0.01 ng/mL, 120-minute C-peptide: 0.13 ng/ml). In terms of islet-specific pancreatic autoantibodies, anti-glutamic acid decarboxylase (GAD) antibody, anti-islet cell antibody (ICA), insulin autoantibody, insulinoma-associated antigen-2 (IA-2) antibody and zinc-transporter 8 (ZnT8) antibody showed all negative. In light of the characteristics at onset and results above, she was diagnosed with FT1D. Further immunological tests showed a significantly reduction in T lymphocyte count. The CD4+ and CD8+ T lymphocyte count were both at a lower level though within the normal range (Table 1). We applied the continuous glucose monitoring after admission, and found high glucose variability (time in range [TIR]: 55.2–65.0%; time below range [TBR]: 10.4–33.3%; time above range [TAR]: 1.7–34.4%; glucose range: 2.2–25.0mmol/L; coefficient of variation [CV]: 45.05–70.02%) and recurrent hypoglycemia, which frequently occurred in the early morning. In order to control the blood glucose, insulin pump (Medtronic, Minneapolis, MN, USA) was used for five days. The dosage and category of insulin used in the insulin pump was 8.1 units of insulin aspart per day (the hourly dosage of insulin: 0.4 units per hour from 8 a.m.to 10 p.m., 0.2 units per hour from 10 p.m. to 3 a.m. of the next day and 0.3 units per hour from 3 a.m. to 8 a.m. of the next day). Five days later, she gained a more stable blood glucose curve (TIR: 76.1%; TBR: 0%; TAR: 23.9%; glucose range: 7.4–14.0 mmol/L; CV: 15.52%), so we switched the insulin pump to subcutaneous injection of insulin four times per day. Two weeks later, the blood glucose curve remained stable (TIR: 88.3%; TBR: 0%; TAR: 11.7%; glucose range: 4.7–15.6mmol/L; CV: 36.34%) and we completed the continuous glucose monitoring.
Table 1
Laboratory findings
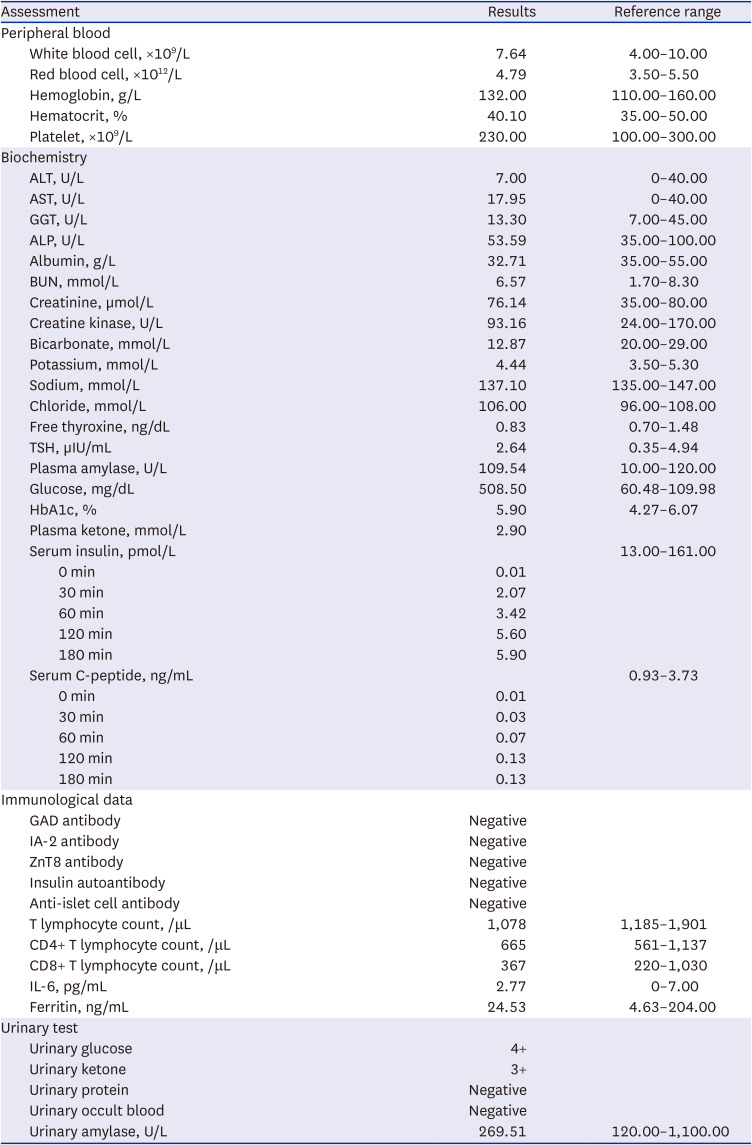
ALT = alanine aminotransferase, AST = aspartate transaminase, GGT = glutamyl transpeptidase, ALP = alkaline phosphatase, BUN = blood urea nitrogen, TSH = thyroid-stimulating hormone, HbA1c = hemoglobin A1c, GAD = glutamic acid decarboxylase, IA-2 = insulinoma-associated antigen-2, ZnT8 = zinc-transporter 8, IL-6 = interleukin-6.
DISCUSSION
To the best of our knowledge, this is the first case of FT1D induced by SARS-CoV-2 protein subunit vaccine. Although we could not confirm the objective causal relationship, the temporal relationship indicated a strong link between SARS-CoV-2 protein subunit vaccine and FT1D.
New-onset T1D has been observed following SARS-CoV-2 infection.1314 This phenomenon could be explained by the fact that the spike protein on the surface of SARS-CoV-2 virus can facilitate viral entry into islet cells via angiotensin converting enzyme 2 (ACE2), a membrane-bound receptor, and then initiate the imbalance of T lymphocytes and the activation of cytokine storm, thus inducing islet beta cell apoptosis and DKA.15161718 As an emerging and promising SARS-CoV-2 vaccine, the protein subunit vaccine utilizes recombinant protein technology to produce the extracellular portion of the spike protein of SARS-CoV-2.1920 Due to structural homology, molecular mimicry could be proposed to cause hyperglycemia after SARS-CoV-2 vaccination. It is possible that the spike protein in the SARS-CoV-2 vaccines could cross-react with the ACE2 receptors of islet cells target proteins due to molecular mimicry to cause islet cells damage. The mechanism of molecular mimicry has been also proposed to prove the causal relationship between thyroid dysfunction and SARS-CoV-2 vaccination.21 However, the mechanism of FT1D induced by SARS-CoV-2 vaccination still needs further research.
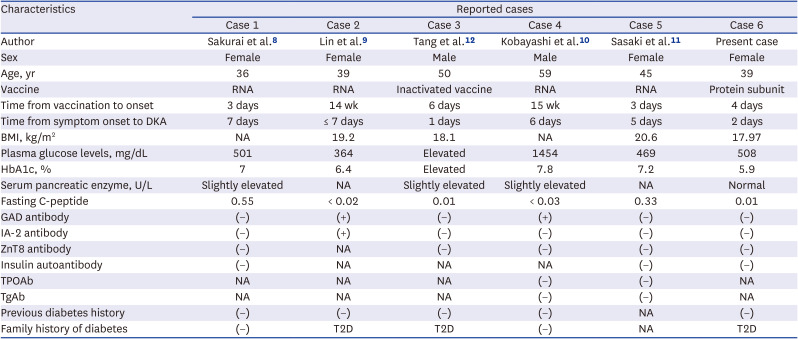
We further conducted searches in PubMed, Web of Science, and MEDLINE database for existing reported cases of FT1D induced by SARS-CoV-2 vaccination in order to have a better understanding of the clinical characteristics of SARS-CoV-2 vaccine-related FT1D. Five related cases were finally included. As shown in Table 2, patients with FT1D followed by SARS-CoV-2 vaccination were predominantly female (four female vs. two male), young and middle-aged (range from 36 to 59 years old) and thin (BMI range from 17.97 to 20.6 kg/m2). These reported vaccines included four mRNA vaccines and one inactivated vaccine while our present case was the first case with respect to the protein subunit vaccine. The duration from symptoms onset to diagnosis among these cases were all within seven days. The levels of serum pancreatic enzyme were slightly elevated in some cases,81012 corresponding to previous reported cases of FT1D.2223 This phenomenon could be explained by leukomonocyte infiltration in exocrine pancreatic acinar cells rather than insulitis.24 As for islet-specific pancreatic autoantibodies, there were only two cases with positive GAD antibody. We further compared the cases with positive and negative GAD antibodies, and found that positive GAD antibodies were significantly associated with more complete destruction and worse secretion capacity of islet beta cells. Kawasaki et al. have showed that the proportion of GAD antibody accounted for 9% of FT1D patients,23 which shared a similarity with these cases. This indicated that islet-associated autoimmune processes may partake in the pathogenesis of FT1D patients with positive GAD antibodies.22
Table 2
Comparison of characteristics of FT1D after SARS-CoV-2 vaccination
| Characteristics | Reported cases | |||||
|---|---|---|---|---|---|---|
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | |
| Author | Sakurai et al.8 | Lin et al.9 | Tang et al.12 | Kobayashi et al.10 | Sasaki et al.11 | Present case |
| Sex | Female | Female | Male | Male | Female | Female |
| Age, yr | 36 | 39 | 50 | 59 | 45 | 39 |
| Vaccine | RNA | RNA | Inactivated vaccine | RNA | RNA | Protein subunit |
| Time from vaccination to onset | 3 days | 14 wk | 6 days | 15 wk | 3 days | 4 days |
| Time from symptom onset to DKA | 7 days | ≤ 7 days | 1 days | 6 days | 5 days | 2 days |
| BMI, kg/m2 | NA | 19.2 | 18.1 | NA | 20.6 | 17.97 |
| Plasma glucose levels, mg/dL | 501 | 364 | Elevated | 1454 | 469 | 508 |
| HbA1c, % | 7 | 6.4 | Elevated | 7.8 | 7.2 | 5.9 |
| Serum pancreatic enzyme, U/L | Slightly elevated | NA | Slightly elevated | Slightly elevated | NA | Normal |
| Fasting C-peptide | 0.55 | < 0.02 | 0.01 | < 0.03 | 0.33 | 0.01 |
| GAD antibody | (−) | (+) | (−) | (+) | (−) | (−) |
| IA-2 antibody | (−) | (+) | (−) | (−) | (−) | (−) |
| ZnT8 antibody | (−) | NA | (−) | (−) | (−) | (−) |
| Insulin autoantibody | (−) | NA | NA | NA | (−) | (−) |
| TPOAb | NA | NA | NA | (−) | (−) | NA |
| TgAb | NA | NA | NA | (−) | (−) | NA |
| Previous diabetes history | (−) | (−) | (−) | (−) | NA | (−) |
| Family history of diabetes | (−) | T2D | T2D | (−) | NA | T2D |
FT1D = fulminant type 1 diabetes, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, DKA = diabetes ketoacidosis, BMI = body mass index, HbA1c = hemoglobin A1c, GAD = glutamic acid decarboxylase, IA-2 = insulinoma-associated antigen-2, ZnT8 = zinc-transporter 8, TPOAb = thyroperoxidase antibodies, TgAb = thyroglobulin antibodies, T2D = type 2 diabetes, (−) = negative, NA = not available.
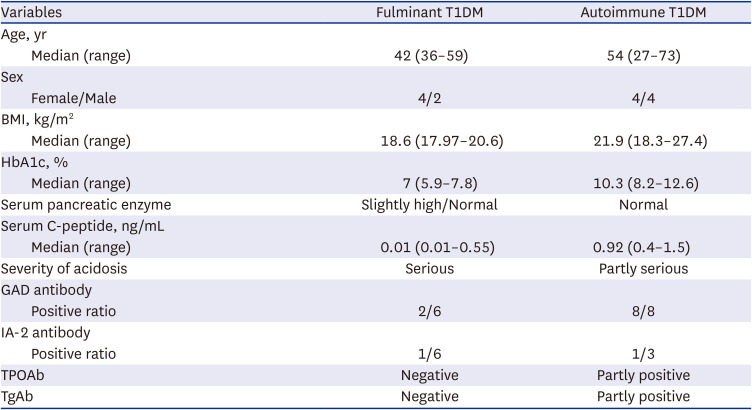
Moreover, we conducted a systematic review on the comparison between FT1D and autoimmune T1D followed by SARS-CoV-2 vaccination. After searching PubMed, Web of Science, and MEDLINE database for existing reported cases of new-onset T1D following SARS-CoV-2 vaccination, six cases with FT1D and eight cases with autoimmune T1D following SARS-CoV-2 vaccination were included. The characteristics of FT1D and autoimmune T1D after SARS-CoV-2 vaccination were summarized in Table 3. Patients with FT1D following vaccination were predominantly younger, female, and thinner. The first symptoms of FT1D were mostly typical symptoms of DKA, and some were accompanied by adverse reactions of vaccines such as fatigue and a slight fever.101112 Patients with FT1D were more likely to have shorter onset time, more serious ketoacidosis, and lower HbA1c. The levels of amylase increased in some FT1D patients.81012 Most cases with FT1D reported negative GAD antibodies while all patients with autoimmune T1D had positive GAD antibodies.
Table 3
Comparison between fulminant T1DM and autoimmune T1DM after SARS-CoV-2 vaccination
In conclusion, we reported a patient with typical fulminant type 1 diabetes four days after SARS-CoV-2 protein subunit vaccination. The normal fasting blood glucose in the physical examination report seven weeks ago and normal HbA1c onset of this patient confirmed the connection between FT1D and this vaccine. We could not confirm the causal relationship between them, which requires long-term and large-scale population research. Nevertheless, we summarized the characteristics of the currently published FT1D following SARS-CoV-2 vaccination to help clinicians make early diagnosis and treatment. We highly appreciate the tremendous benefits of large-scale SARS-CoV-2 vaccination, but we still hope to alert about related adverse consequences and strengthen the pharmacovigilance and supervision during mass SARS-CoV-2 vaccination. It is important for clinicians to remain vigilant for acute deterioration of hyperglycemia and acidosis and we also recommend careful monitoring following SARS-CoV-2 vaccination even without a medical history of diabetes. Early identification and treatment can halt the progression of FT1D and prevent complications.
 XML Download
XML Download