

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
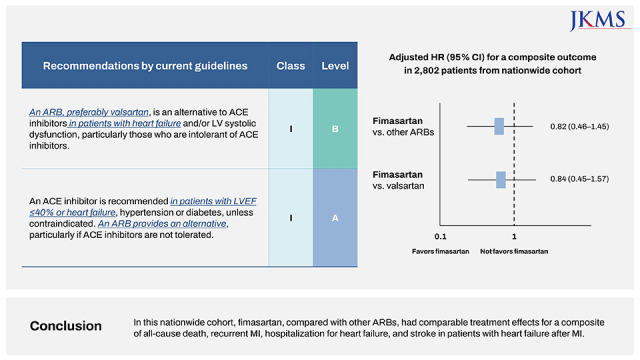
In patients with myocardial infarction (MI) and heart failure or left ventricular systolic dysfunction, current guidelines recommend angiotensin II receptor blocker (ARB) therapy during and after hospitalization for those who do not tolerate an angiotensin-converting enzyme inhibitor (ACEI).123 However, due to high rate of adverse symptoms and consequent discontinuation of ACEIs,4567 ARBs are often prescribed as a first-line drug in these populations. In the nationwide registry of acute MI between 2005 and 2016, the prescription rate of ARBs at hospital discharge was 26%.8 Although valsartan is preferably recommended by the guideline for management of acute MI,1 various ARBs are used in real world practice.9
Fimasartan is the ninth ARB that is a derivative of losartan, but is more potent and longer-acting than losartan.10 Fimasartan demonstrated an effective blood pressure lowering effect in patients with hypertension and excellent safety profile in a large population observational study.11 In animal studies, fimasartan ameliorates heart failure12 and is cardioprotective after acute MI.13 However, so far, no data are available for treatment effects of fimasartan in patients with heart failure after acute MI. Therefore, in the present study, we sought to compare fimasartan with other ARBs in patients with heart failure after MI using the nationwide medical insurance data of Korean population.
METHODS
Study population
Korea has a single-payer national health system, and the National Health Insurance Service (NHIS) maintains national records of all covered inpatient and outpatient visits, procedures, and prescriptions. This is a population–based retrospective cohort study which was built using the NHIS data.141516 NHIS provides 50% of the random sample of the national data if the study includes information about specific drugs.
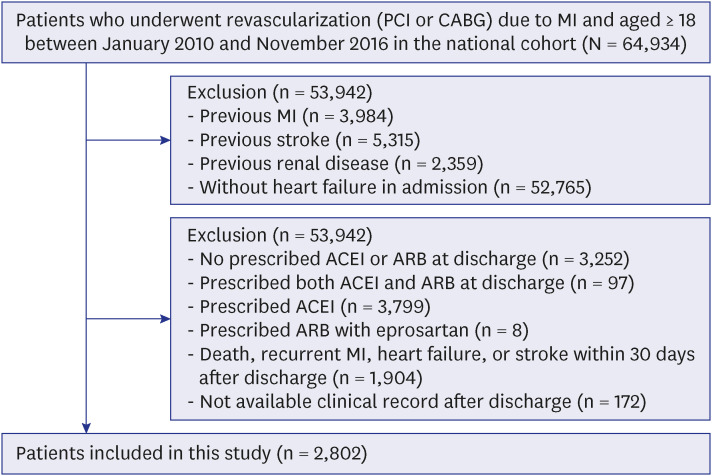
Among all Korean men and women over 18-years-old between January 1, 2010 and November 31, 2016, we selected patients who underwent revascularization (percutaneous coronary intervention [PCI] or coronary artery bypass graft surgery) due to MI (n = 64,934). Because our objective was to compare clinical outcomes according to different types of ARBs after hospital discharge in patients with heart failure, we excluded patients who did not have heart failure at hospital discharge regardless of previous diagnosis (n = 52,765). We also excluded patients who had history of MI (I21–I23, I252) (n = 3,984), stroke (I60–I63) (n = 5,315), and renal disease (N18, N19) (n = 2,359). Then we excluded patients without any prescription of ARB or ACEI (n = 3,252), or those with prescription of ACEI (n = 3,799) or both ARB and ACEI (n = 97) at discharge. Patients who received eprosartan (n = 8) were excluded due to low prescription rate. In addition, we excluded patients who had death, recurrent MI, heart failure, or stroke within 30 days after index MI (n = 1,904) or those without any medical record available after discharge (n = 172). Finally, 2,802 patients were included in this study (Fig. 1).
Outcomes and definitions
NHIS claims for inpatient and outpatient visits, procedures, and prescriptions were coded using the International Classification of Diseases, 10th Revision.17 As the NHIS routinely audits the claims, such data are considered reliable and used in numerous peer-reviewed publications.1415 In regard to diagnosis of MI, the validation study in 2013 showed the value of 93%.18
The primary outcome was a composite of all-cause death, recurrent MI, hospitalization for heart failure, and stroke. Vital status and cause of death were obtained from death certification collected by Statistics Korea at the Ministry of Strategy and Finance of South Korea.14 The secondary outcomes were individual components of the primary outcome.
Study exposure was an initial type of ARB used at hospital discharge. The initial use of study drugs was defined as prescription for at least 7 days among the admission claim or as prescription at first outpatient clinic. Previous ARB therapy was defined as presence of prescription during 6 months prior to index MI. Comorbidities were summarized using Charlson index. In addition, we included diabetes mellitus (E11–E14), hypertension (I10–I13, I15), atrial fibrillation or flutter (I48), chronic obstructive pulmonary disease (J43–J46), and peripheral artery disease (I73, I701, I702, I708, I709, I771, I792, K551, K558, K559). Comorbidities were defined as presence of code in claims within a year before index MI. We identified medications including calcium channel blocker, statin, aspirin, clopidogrel, ticagrelor or prasugrel, anticoagulant, beta-blocker, and spironolactone at discharge. Medications were identified with using the Korean Drug and Anatomical Therapeutic Chemical Codes (Supplementary Table 1).
Statistical analysis
Patients were followed-up until the development of study outcomes, or the end of the study period (December 31, 2016). Clinical outcomes of fimasartan were compared with other ARBs or valsartan. Cumulative incidence of outcome was estimated by the Kaplan-Meier method and log rank tests were applied to evaluate differences between the groups. We calculated hazard ratios (HRs) with 95% confidence intervals (CIs) for incidence of clinical outcome using a mixed-effects Cox regression model including an admitted hospital as a random intercept to adjust hospital effect. Furthermore, to account for potential confounding factors, we adjusted for age, sex, previous revascularization, previous ARB or ACEI therapy, diabetes mellitus, hypertension, hyperlipidemia, atrial fibrillation of flutter, chronic obstructive pulmonary disease, peripheral artery disease, malignancy, admission at tertiary hospital, and discharge medication including calcium channel blocker, statin, aspirin, clopidogrel, ticagrelor or prasugrel, anticoagulant, beta-blocker, or spironolactone. We examined the proportional hazards assumption using plots of the log-log survival function and Schoenfeld residuals.
Additionally, clinical outcomes of each ARB were compared with other ARBs in the same way as fimasartan. All P values were 2-sided, and a P value of less than 0.05 was considered as significant. Analyses were performed with the use of SAS® Visual Analytics (SAS Institute Inc., Cary, NC, USA).
RESULTS
Clinical characteristics
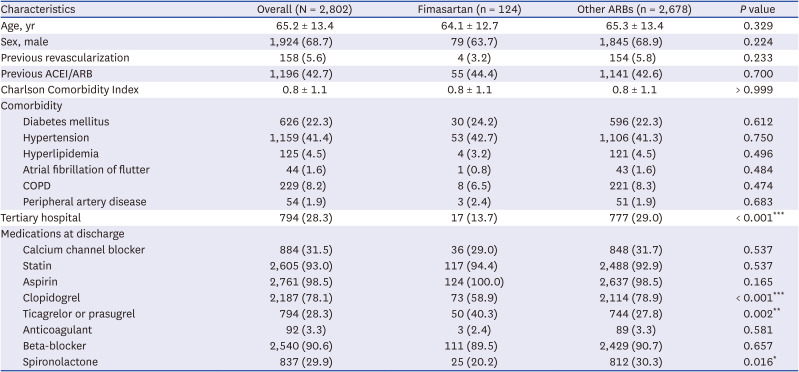
The mean age of 2,802 study patients was 65.2 years, 68.7% were male, and 42.7% had a history of ARB or ACEI prescription before the index MI. At hospital discharge, the most frequently prescribed ARB was candesartan (30.2%), followed by valsartan (26.5%), losartan (21.3%), telmisartan (7.6%), Olmesartan (6.0%), fimasartan (4.4%), and irbesartan (4.0%).
Compared with other ARBs, patients receiving fimasartan were less likely to be treated in tertiary hospital and to receive clopidogrel and spironolactone (Table 1). There were no significant differences in age, sex, previous history of ACEI or ARB prescription and comorbidities between patients receiving fimasartan and those receiving other ARBs. Baseline characteristics according to each type of ARBs are summarized in Supplementary Table 2.
Table 1
Characteristics of study participants between valsartan and other ARBs
Clinical outcomes of fimasartan
During follow-up (median 2.2 years, interquartile range 1.0–3.9), 613 events of the primary outcome occurred. There was no significant difference in the primary outcome among 7 different ARBs (P = 0.098; Fig. 2). Compared with patients receiving other ARBs, those receiving fimasartan had the numerically lowest incidence of the primary outcome (63.6 per 1,000 person-years) but it was not statistically significant (adjusted HR, 0.82; 95% CI, 0.46–1.45; P = 0.489 vs. other ARBs) (Tables 2 and 3).
Fig. 2
Clinical outcomes according to different types of angiotensin II receptor blockers.
aA composite of all-cause death, recurrent myocardial infarction, hospitalization for heart failure, and stroke.
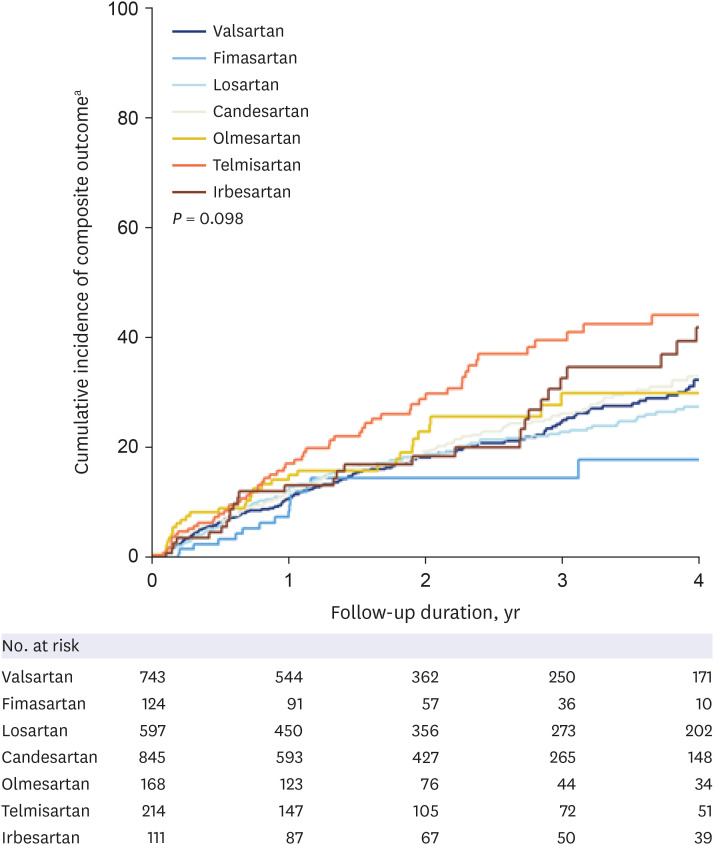
Table 2
Incidence of a composite of all-cause death, recurrent myocardial infarction, hospitalization for heart failure, and stroke according to types of angiotensin II receptor blockers

Table 3
HRs (95% CIs) of fimasartan for clinical outcomes compared to other ARBs or valsartan
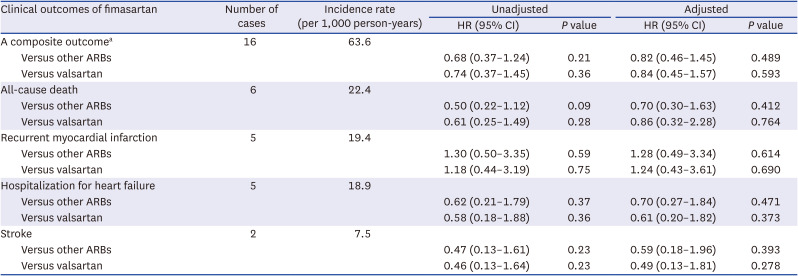
HRs were adjusted for age, sex, previous revascularization, previous ARB or angiotensin-converting enzyme inhibitor therapy, diabetes mellitus, hypertension, hyperlipidemia, atrial fibrillation of flutter, chronic obstructive pulmonary disease, peripheral artery disease, malignancy, admission at tertiary hospital, and discharge medications.
ARB = angiotensin II receptor blocker, CI = confidence interval, HR = hazard ratio.
aA composite of all-cause death, recurrent myocardial infarction, hospitalization for heart failure, and stroke.
Patients receiving fimasartan had no significant differences in the incidence of all-cause death (adjusted HR, 0.70; 95% CI, 0.30–1.63; P = 0.412), recurrent MI (adjusted HR, 1.28; 95% CI, 0.49–3.34; P = 0.614), hospitalization for heart failure (adjusted HR, 0.70; 95% CI, 0.27–1.84; P = 0.471), or stroke (adjusted HR, 0.59; 95% CI, 0.18–1.96; P = 0.393) compared with those receiving other ARBs.
When compared with patients receiving valsartan, there were no significant differences in the incidence of primary and secondary outcomes in those receiving fimasartan (Table 3).
Clinical outcomes of other ARBs
Each ARB (candesartan, valsartan, losartan, telmisartan, olmesartan, or irbesartan) had no significant differences in the incidence of the primary outcome compared with other ARBs (Supplementary Table 3). The secondary outcomes are presented in Supplementary Table 4.
DISCUSSION
In the present study, we investigated clinical outcomes of fimasartan compared with other ARBs in patients with MI with heart failure. The main findings were as follows. First, there was no significant difference in the incidence of a composite of all-cause death, recurrent MI, hospitalization for heart failure, or stroke in patients receiving fimasartan compared with those receiving other ARBs. Second, the clinical outcomes with fimasartan were comparable with valsartan, the recommended ARB by practice guideline.
Current guidelines for management of MI recommend ACEI as a first-line drug over ARB in patients with heart failure. ACEIs, however, have frequent side effects. For example, the rate of cough is reported up to 44% in Asian population taking ACEI.19 Therefore, as an alternative to ACEI, ARBs are often prescribed in real-world practice.20 The prescription rate of ARBs has been increased over time,9 and the reported rate at hospital discharge was up to 26%.8 Although there are various ARBs commercially available, current practice guidelines for heart failure management2122 recommended the candesartan, losartan, and valsartan as evidence-based drugs. In guidelines for MI,13 the preferred ARB is valsartan based on the VALsartan in Acute myocardial iNfarcTion (VALIANT) trial that showed non-inferiority of valsartan compared to captopril.5 In real world practice, however, various ARBs are prescribed in patients with MI with heart failure. In observational studies, ARBs other than valsartan was prescribed in more than 70% of all patients.923 Because of different pharmacokinetic-pharmacodynamic profiles between ARBs available on market,2425 treatment effect on reducing cardiovascular events could be also different between ARBs.2627 However, data are very limited on this issue in patients with MI and heart failure.
Fimasartan is one of the latest ARBs developed in 2010’s. Fimasartan, a pyrimidin-4(3H)-one derivative of losartan with the imidazole ring replaced, which enables higher potency and longer duration than losartan. With a strong binding affinity to AT1 receptor, fimasartan had the highest association rate compared to other ARBs28 and better efficacy on blood pressure lowering.293031 In addition, fimasartan has the cardioprotective effects against myocardial ischemia and reperfusion injury,32 or heart failure progression12 in preclinical studies. Hence, the favorable data so far suggest the clinical benefit of fimasartan in high-risk population, such as those with MI with heart failure. In this nationwide study, incidence of a composite of all-cause death, recurrent MI, hospitalization for heart failure, or stroke was not significantly different between patients receiving fimasartan and those receiving other ARBs. In addition, clinical outcomes in patients receiving fimasartan was not significantly different compared with those receiving valsartan, the preferable ARB by current guidelines for management of MI.13 Taken together with previous preclinical and clinical evidence, our findings suggest the clinical efficacy of fimasartan in patients with MI with heart failure.
Our study has several limitations. First, this was an observational study. The choice of drug was at the physician’s discretion. Although we conducted an intraclass comparison among different ARBs in patients with MI with heart failure, there is a potential selection bias induced by unrecorded confounders. Second, we did not consider the changes of medication during follow up. The current results should be interpreted considering that each ARB was a prescription at the time of discharge. Third, patients who were event-free at 1 month after discharge were included in the final analysis. The adverse events immediately after discharge might be affected by the severity of disease or patients’ sickness than the beneficial effect of ARBs, especially in high-risk patients such as those with MI complicated by HF. Therefore, we conducted a 1-month landmark analysis to compare outcomes according to the different ARBs. Fourth, although this was a nationwide study using health insurance data, the sample size of each type of ARBs could be inadequate to conclude statistical significance to compare clinical outcomes among different drugs. Last, because the diagnosis of heart failure was based on claims, not the specific criteria such as left ventricular ejection fraction, care should be taken in the interpretation of this study. Despite these limitations, our study has strengths to present clinical outcomes of fimasartan, the latest ARB, in patients with MI with heart failure. In addition, we compared clinical outcomes among various ARBs currently available in real world practice. A large-scale randomized study is needed to determine the current findings, including patients with heart failure unrelated to MI.
In this nationwide cohort study of patients with MI with heart failure, there was no significant difference in incidence of a composite of all-cause death, recurrent MI, hospitalization for heart failure, and stroke in patients receiving fimasartan compared with those receiving other ARBs.
 XML Download
XML Download