

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Kawasaki disease (KD) is an acute-onset febrile disease with systemic vasculitis involving small-to-medium-sized arteries. KD is the most common cause of acquired heart disease in paediatric patients aged < 5 years, manifesting as coronary artery aneurysm and/or dilatation, aortic root dilatation, and myocarditis.12 In contrast to many other diseases, complete KD is diagnosed based on the observed clinical findings alone, and laboratory findings are not considered during diagnosis. Although KD occurs globally, its prevalence is high in Asian countries. With respect to sex, KD is more common in boys than in girls.3 However, the exact aetiology of KD has not yet been identified and is thought to be triggered by infectious agents in individuals with environmental and genetic factors.456 The administration of intravenous immunoglobulin (IVIG) within the first 10 days of illness reduces the incidence of coronary complications. About a quarter of patients with KD are IVIG resistant and are prone to developing coronary artery aneurysms.3
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has rapidly escalated into a global crisis. As COVID-19 has become the most urgent medical issue in the world in patients of all ages, research on the association between COVID-19 and existing diseases is being actively conducted. Although COVID-19 rarely causes serious illness in paediatric patients, post-COVID-19 immune dysregulation, especially in young patients, is emerging as an important medical subject.7 Patients with hyperinflammation syndrome have been reported to present with clinical features comprising high fever and mucocutaneous manifestations resembling those of KD.8 Abnormal post-infectious immunological reactions may play a key role in pathogenesis. Although multisystem inflammatory syndrome in children (MIS-C) has a distinct immunophenotype compared with KD, it is difficult to distinguish from KD.79
With increasing COVID-19 cases, the spectrum of KD has broadened.1011 As it is difficult to distinguish between overlapping MIS-C and KD, the clinical features of KD have changed. Previously, a study comparing SARS-CoV-2 polymerase chain reaction (PCR)-positive KD with negative KD was reported.12 However, to the best of our knowledge, the clinical manifestation of KD have not been previously compared between patients with and without SARS-CoV-2 antibody positivity. In this study, we aimed to 1) determine the clinical features of SARS-CoV-2 antibody-positive KD, 2) compare the clinical features according to the type of SARS-CoV-2 antibody, and 3) analyse the echocardiographic results to compare cardiac complications according to antibody test results.
METHODS
Study design
All consecutive paediatric patients with KD who were admitted at Jeonbuk National University Children’s Hospital Tertiary Referral Center, South Korea between January 1, 2021 and August 15, 2022, were enrolled in this study. KD was diagnosed based on the American Heart Association (AHA) diagnostic criteria.13 The diagnosis was primarily based on clinical symptoms, and laboratory tests were used as adjuncts to the diagnosis of incomplete KD. Eighty-two patients diagnosed with KD, based on echocardiographic data, were enrolled in this study. MIS-C was diagnosed using the criteria of the US Centers for Disease Control published on May 14, 2020.14 Among the enrolled patients, 12 patients met the MIS-C criteria. As we wanted to enrol patients without a diagnosis of MIS-C, only 70 patients were enrolled in this study. The demographic, clinical manifestations, and laboratory findings of KD and the excluded MIS-C cases is presented in Supplementary Table 1. Here, we retrospectively analysed the patients’ demographic data, clinical signs of KD at diagnosis, COVID-19 history, laboratory findings, echocardiographic data, clinical course, response to IVIG, and echocardiographic results after 1 month of IVIG treatment.
A case requiring secondary treatment was defined as refractory KD case. On the other hand, treatment failure on the first IVIG was defined as a case with persistent fever for 36 hours after IVIG, only in patients primarily treated with IVIG.
Serologic tests
Serologic tests were performed for both nucleocapsid (N) and spike (S) proteins. Both IgM and IgG antibodies were used for the interpretation. Serologic tests of both the N and S proteins were performed using blood samples. The samples were analysed using a chemiluminescence immunoassay (SG Medical Inc., Seoul, Korea). Values were regarded as positive if they had a cut-off index of > 1.0, which corresponds to 0.80 U/mL when analysed using electrochemiluminescence immunoassay.
The patients were divided into 2 groups according to the antibody test results (Fig. 1). The SARS-CoV-2 N antibody positive patients were assigned to group 1, whereas group 2 included the SARS-CoV-2 N antibody negative patients. As S antibody positivity can occur even in vaccinated patients, we categorized patients only based on the results of the N antibody test.
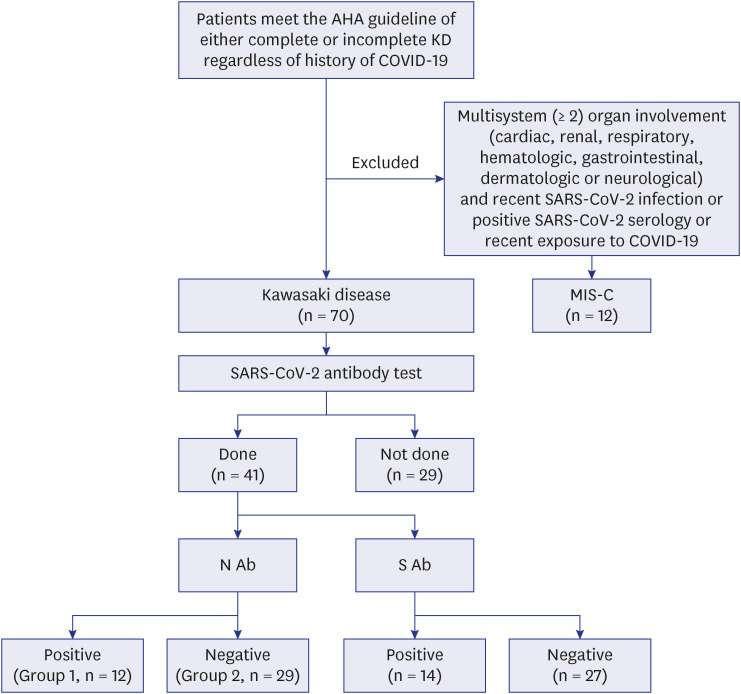
Fig. 1
Flow chart of enrolled patients and the result of SARS-CoV-2 Ab test.
AHA = American Heart Association, KD = Kawasaki disease, COVID-19 = coronavirus disease 2019, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, MIS-C = multisystem inflammatory syndrome in children, N = nucleocapsid, S = spike, Ab = antibody.
![]()
Echocardiography
A Philips IE33 system (Philips Medical Systems, Andover, MA, USA) was used for echocardiography. Echocardiography was performed by a paediatric cardiologist (J.Y.). The video recorded the heartbeat of 3-cycle loops. Transducers were selected based on the patient’s physique. All echocardiographic data were analysed using an in-machine analysis program, aCMQ (Philips Medical Systems). The z-score of coronary arteries was calculated according to the method published by Dallaire and Dahdah15 Coronary artery dilatation was defined as a z-score ≥ 2.0 or a decrease in z-score ≥ 1.0 during follow-up according to the AHA KD guideline.13 The coronary artery aneurysm was defined as a z-score ≥ 2.5.13 The diastolic left ventricular internal diameter (LVIDd) z-score was calculated using the method reported by Pettersen et al.16
For 2-dimensional strain analysis, the myocardium was manually traced at end diastole on a single frame, and the machine automatically analysed it later. Longitudinal strain was analysed using apical 4-chamber images. As only 1 experienced investigator performed and evaluated the echocardiogram, inter-observer reproducibility testing was not conducted.
Statistical analysis
The SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses. Statistical significance was set at P < 0.05. Numerical data are expressed as mean ± standard deviation, and categorical data are expressed as frequency (%). A comparison of echocardiographic data between the 2 time points (at diagnosis vs. 1 month after diagnosis) was performed using a paired t-test. The patients were divided into 2 groups according to the results of the serological test for SARS-CoV-2. Group 1 comprised patients who were positive for N-type antibodies, and they were considered to have had COVID-19 previously, whereas group 2 comprised patients who were negative for N-type antibodies. Unpaired t-tests, Mann-Whitney test, Fisher’s exact test, and Pearson χ2 tests were used to compare the data between the 2 groups. To investigate the predictors of IVIG-refractory KD, we performed univariable and multivariable logistic regression analyses, with IVIG-refractory KD treated as a categorical variable (1 for refractory KD and 0 for non-refractory KD).
RESULTS
An antibody test was conducted in 53 patients. The SARS-CoV-2 N antibody test result was positive in 23 patients, and the S antibody test result was positive in 24 patients. After excluding patients with MIS-C, an antibody test was conducted in 41 patients. Among them, the SARS-CoV-2 N antibody was identified in 12 patients, and the S antibody was identified in 14 patients. A flow chart of the enrolled patients can be seen in Fig. 1. Differences in demographic and clinical characteristics depending on whether the antibody test was performed are shown in Supplementary Table 2. No significant differences in the demographic and clinical manifestations were observed between patients who did and did not undergo the antibody test. The mean age of the group in which the antibody test was performed was 2.4 ± 3.0 years.
Clinical and laboratory findings according to the result of the antibody test
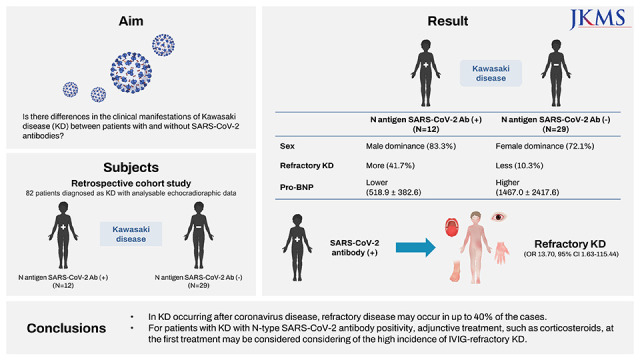
The demographic and clinical characteristics according to the SARS-CoV-2 N antibody test results are shown in Table 1. The mean age of group 1 was 2.4 ± 2.0 years, and that of group 2 was 2.4 ± 3.3 years (P = 0.972). In group 1, the proportion of male patients was significantly higher than that in group 2 (P = 0.008). The incidence of other symptoms, such as duration of fever until treatment, rash, conjunctivitis, lip or oral mucosal change, and extremity change, was not significantly different between the groups.
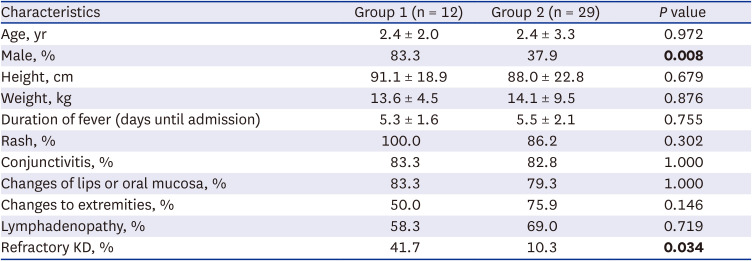
Table 1
Demographic and clinical characteristics, and outcomes according to the SARS-CoV-2 N antibody test results
Group 1, SARS-CoV-2 N antibody positive patients; Group 2, SARS-CoV-2 N antibody negative patients.
P value less than 0.05 are indicated in bold.
KD = Kawasaki disease, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, N = nucleocapsid.
![]()
Laboratory findings
A comparison of the laboratory findings in both groups is presented in Table 2. No difference was observed between groups 1 and 2 in complete blood counts, blood chemistry results, and electrolyte levels. However, group 1 showed lower pro-B-type natriuretic peptide (pro-BNP) levels than group 2 (518.9 ± 382.6 vs. 1,467.0 ± 2,417.6, P = 0.049).
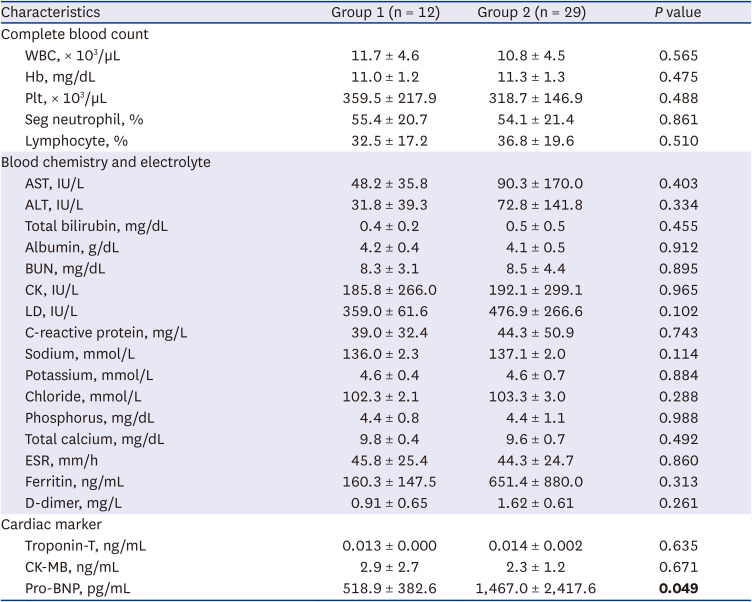
Table 2
Laboratory findings according to the results of SARS-CoV-2 N antibody test
Group 1, SARS-CoV-2 N antibody positive patients; Group 2, SARS-CoV-2 N antibody negative patients.
P value less than 0.05 are indicated in bold.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, N = nucleocapsid, WBC = white blood cell, Hb = hemoglobin, Plt = platelet, Seg neutrophil = segmented neutrophil, AST = aspartate aminotransferase, ALT = alanine aminotransferase, BUN = blood urea nitrogen, CK = creatine kinase, LD = lactate dehydrogenase, ESR = erythrocyte sedimentation rate, CK-MB = creatine kinase-myoglobin binding, pro-BNP = pro-B-type natriuretic peptide.
![]()
Response to IVIG treatment
In group 1, refractory KD occurred in 41.7% of patients. Its incidence was higher than that in group 2 (10.3%, P = 0.034, Table 1). All patients with refractory KD used corticosteroid concomitantly to the secondary IVIG treatment. IVIG treatment failure occurred in 41.7% of patients in group 1 and in 13.0% of patients in group 2 (P = 0.056). In other words, six patients (20.7%) of group 2 recovered from KD without IVIG treatment, whereas no patient in group 1 recovered spontaneously without IVIG treatment. The laboratory findings regarding refractoriness are shown in Supplementary Table 3. Only sodium levels were different between the two groups. In the refractory group, the sodium level was lower than that of the responsive group (134.9 ± 2.0 vs. 137.3 ± 1.9, P = 0.003). To clearly identify the relationship between the N SARS-CoV-2 antibody and refractory Kawasaki, multivariable analysis was performed by setting the independent variables previously known to cause refractory KD: age ≤ 12 months, fever ≤ 4 days, neutrophil level ≥ 80%, sodium level ≤ 133 mmol/L, platelet count ≤ 300,000/µL, aspartate aminotransferase (AST) level ≥100 IU/L, and C-reactive protein (CRP) level ≥ 10 mg/dL. SARS-CoV-2 antibody positivity could predict the occurrence of refractory KD even in the multivariable analysis (odds ratio, 13.70; 95% confidence interval, 1.63–115.44; P = 0.016) (Table 3).17

Table 3
Risk factors of immunoglobulin-resistant Kawasaki disease
The univariable and multivariable analysis of risk factors according to the reported Kobayashi score.
P value less than 0.05 are indicated in bold.
OR = odds ratio, CI = confidence interval, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, Ab = antibody, Na = sodium, Plt = platelet, AST = aspartate aminotransferase, CRP = C-reactive protein.
![]()
Echocardiographic data
There was no statistically significant difference between the groups on echocardiography at the time of diagnosis (Table 4). The mean left main coronary artery (LMCA) z-score was larger than 2.0 only in group 1 (2.44 ± 1.42), and the mean left anterior descending artery (LAD) z-score was larger than 2.0 in both groups (2.65 ± 1.34 and 2.06 ± 1.72). Aneurysm of one or more coronary arteries occurred in a total of 16 patients (39.0%); more specifically, in 5 (41.7%) and 11 (37.9%) patients from groups 1 and 2, respectively. There was no significant difference in the occurrence of coronary artery aneurysm between groups (P = 1.000).
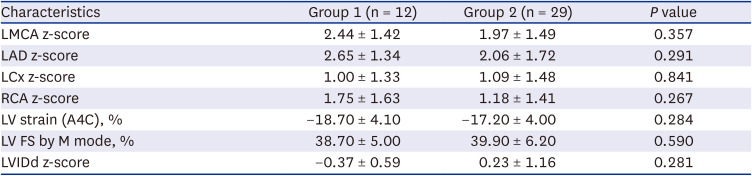
Table 4
Echocardiographic data at diagnosis according to the results of SARS-CoV-2 N antibody test
Group 1, SARS-CoV-2 N antibody positive patients; Group 2, SARS-CoV-2 N antibody negative patients.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, N = nucleocapsid, LMCA = left main coronary artery, LAD = left anterior descending artery, LCx = left circumflex artery, RCA = right coronary artery, LV = left ventricle, A4C = apical four chambers, FS = fractional shortening, LVIDd = diastolic left ventricular internal diameter.
![]()
Echocardiographic changes 1 month after KD diagnosis
The z-score of all coronary arteries decreased 1 month after the diagnosis of KD (Fig. 2). The mean LMCA, LAD, left circumflex artery, and right coronary artery z-scores 1 month after KD diagnosis were 1.56 ± 1.12, 1.33 ± 0.92, 0.80 ± 0.97, and 1.25 ± 1.32, respectively (P < 0.001, P < 0.001, P = 0.003, and P = 0.005, respectively). The mean LVIDd z-score 1 month after the diagnosis of KD was −0.11 ± 1.11, which was larger than the value at diagnosis (−0.39 ± 0.65, P = 0.018).
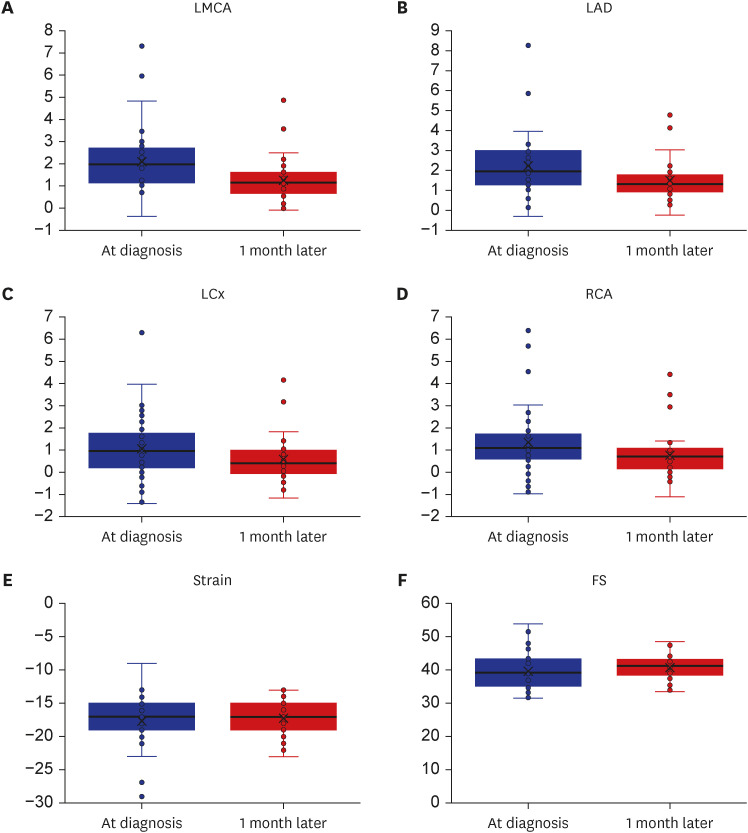
Fig. 2
Echocardiographic parameters change 1 month after KD diagnosis. (A) LMCA z-score changes at diagnosis and 1 month after diagnosis (2.30 ± 1.15 to 1.56 ± 1.12, P < 0.001). (B) LAD z-score changes at diagnosis and 1 month after diagnosis (1.95 ± 1.02 to 1.33 ± 0.92, P < 0.001). (C) LCx z-score changes at diagnosis and 1 month after diagnosis (1.23 ± 1.22 to 0.80 ± 0.97, P = 0.003). (D) RCA z-score changes at diagnosis and 1 month after diagnosis (1.84 ± 1.45 to 1.25 ± 1.32, P = 0.005). (E) Apical 4-chamber LV longitudinal strain changes at diagnosis and 1 month after diagnosis (−17.3 ± 2.6% to −17.9 ± 4.0%, P = 0.424). (F) LV FS changes at diagnosis and 1 month after diagnosis (40.9 ± 3.8% to 40.0 ± 5.8%, P = 0.462).
LMCA = left main coronary artery, LAD = left anterior descending artery, LCx = left circumflex artery, RCA = right coronary artery, LV = left ventricle, FS = fractional shortening, KD = Kawasaki disease.
![]()
In group 1, all coronary arteries z-scores, LVIDd z-score, and fractional shortening (FS) on M mode changed 1 month after diagnosis (Supplementary Table 4). In group 2, only the z-scores of all coronary arteries changed 1 month after KD diagnosis (Supplementary Table 5). Aneurysm of one or more of the coronary arteries was detected 1 month after the diagnosis in a total of 5 patients (12.2%), 1 patient (8.3%) of group 1 and 4 patients (13.7%) of group 2; there were no differences between both groups (P = 0.640).
DISCUSSION
To the best of our knowledge, this is the first study to investigate the effect of SARS-CoV-2 antibodies on the clinical manifestation of KD. As COVID-19 has become a pandemic, the number of asymptomatic and mild symptomatic patients with COVID-19 who do not undergo SARS-CoV-2 PCR testing has increased. Although approximately 0.3 million people have been newly infected in the last 24 hours globally, the exact percentage or number of COVID-19-infected paediatric patients has not been estimated.18 The SARS-CoV-2 antibody test can be used to identify the number of paediatric patients infected with SARS-CoV-2, especially in situations where we cannot accurately estimate the number of infected patients. As COVID-19 will become endemic, knowing its impact on the underlying disease is important to prepare for the post-COVID-19 era.
A few studies on the effect of a history of COVID-19 on KD other than MIS-C have been conducted. Although there is 1 study on the effect of COVID-19 on KD, no studies have reported the effect of SARS-CoV-2 antibody production on KD. In a previous study, patients with COVID-19 PCR-positive KD had a higher incidence of rash (72% vs. 30%, P = 0.023) and fewer echocardiographic abnormalities (31.8% vs. 40.0%, P = 0.040) than those with COVID-19 PCR-negative KD.12 In this study, none of the patients were PCR positive for COVID-19. Moreover, we studied past COVID-19 infection, which can affect the clinical manifestation of KD, but not current COVID-19 infection.
Patients diagnosed with MIS-C were excluded from this study. No difference in demographic data between the 2 groups were observed. Although MIS-C and KD have common clinical features, they are considered distinctly different diseases.919 Despite some reports showing that IVIG-refractory cases are more frequent in MIS-C than in KD, accurate data are inadequate.20 Even after excluding patients with MIS-C, our study showed that patients with SARS-CoV-2 antibody positivity had 6.19 times greater odds of developing IVIG refractory KD than those with SARS-CoV-2 antibody negativity. Additionally, we investigated the risk factors of refractory KD already reported by Kobayashi et al.17—age ≤ 12 months, fever ≤ 4 days, neutrophil level ≥ 80%, sodium level ≤ 133 mmol/L, platelet count ≤ 300,000/µL, AST level ≥ 100 IU/L, and CRP level ≥ 10 mg/dL. However, SARS-CoV-2 N antibody positivity was the only risk factor for immunoglobulin resistance on the multivariable analysis. The mechanism by which SARS-CoV-2 antibody may trigger immunoglobulin resistance should be investigated. We hypothesised that this was due to changes in cytokine levels. In a previous study, MIS-C patients had higher levels of inflammatory monocyte-activating SARS-CoV-2 IgG antibodies compared to those in acute cases of COVID-19 in children.21 In another study, MIS-C patients were characterized with high levels of interleukin (IL)-1β, IL-6, IL-8, IL-10, IL-17, interferon-γ, and different T- and B-cell subsets, resulting in lymphopenia.22 We hypothesised that even in patients with KD, previous COVID-19 infection can affect lymphocyte activation and cytokine production, resulting in a condition resembling to that of MIS-C. Further studies on the pathophysiology of COVID-19 are needed.
Although it is traditionally known that boys have a higher prevalence of KD than girls, in this study, we observed a higher incidence of KD in girls than in boys among those without a history of COVID-19.19 The pro-BNP level was different between the 2 groups, although there was no significant difference in echocardiographic data between the 2 groups. The pro-BNP levels were higher in group 2 than in group 1. We hypothesised that this is because group 1 had a lower LVIDd z-score than group 2, although this was not statistically significant. The tendency for a lower preload in group 1 can affect pro-BNP levels. Unlike in group 2, in group 1, LVIDd and FS also tended to normalize after 1 month, which is presumably because, as mentioned above, LVIDd z-score tends to lower in group 1 than in group 2.
Our study included many patients with coronary artery dilatation. We chose Dallaire and Dahdah’s equation for calculating the coronary arteries z-scores. Since only one investigator performed the measurements, the possibility of bias in coronary artery diameter evaluation cannot be ignored. Considering that the mean z-score of the coronary arteries decreased on the follow-up echocardiography after 1 month, it may not be enough to explain the overestimation. In fact, although approximately two-fifths of patients with KD had a z-score ≥ 2.5, showing coronary artery aneurysm of one or more of the coronary arteries at the time of diagnosis, that percentage decreased to 12.2% of cases in the 1-month follow-up echocardiographic data.
Antibodies after SARS-CoV-2 infection in adults can remain detectable beyond 500 days depending on the patient’s underlying condition.23 In paediatric patients, antibodies remained detectable for up to 3 months after COVID-19.24 In our study, KD occurred 25–109 days after COVID-19. However, among the 12 patients with SARS-CoV-2 N antibody-positive KD, only 5 had a history of COVID-19 in our study. Therefore, it is not possible to determine the presence of antibodies solely based on the history of COVID-19. In our study, we investigated the clinical manifestations and laboratory and echocardiographic findings according only to antibody results, regardless of past COVID-19 infection. Further studies will be necessary to determine whether the SARS-CoV-2 N antibody is a prevailing predictor of refractory KD that can be reduced by COVID-19 vaccination.
As a limitation, this was a single-centre retrospective study, and SARS-CoV-2 antibody test was not performed in all patients. However, there were no differences in the clinical features depending on whether the antibody test was performed. Further large-scale studies are required in the future. Nevertheless, this study is the first to analyse whether the presence of SARS-CoV-2 antibody affects the clinical manifestations of KD.
In post-COVID-19 KD, resistance to IVIG treatment may occur in up to 40% of the cases. In patients with SARS-CoV-2 N antibody-positive KD, there is a high incidence of IVIG-refractory KD. In conclusion, adjuvant treatments, such as corticosteroids, may be considered as a first approach for such patients.
 XML Download
XML Download