

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Iron is an important trace element and an essential component of hemoglobin, myoglobin, cytochromes, and proteins responsible for oxygen storage, transport, and utilization.123 It is critical for oxidative energy generation. Therefore, cells with high energy demand, such as cardiac myocytes, are especially sensitive to iron underutilization.4 Iron deficiency (ID), regardless of the presence of anemia, can manifest as reduced quality of life, exercise capacity,5 and survival.6
The prevalence of ID ranges between 2% and 10% in the general population.78 In patients with heart failure (HF), dietary iron intake9 and enteral absorption are reduced10 and systemic inflammation is elevated,11 with prevalence of ID being as high as 50–60%.121314 Patients with ID had worse prognosis,131516 but its correction with intravenous (IV) iron supplementation improved the clinical outcomes.17181920
Despite the clinical importance of ID in HF, data on its prevalence are scarce, especially in East Asians.21 Therefore, in this prospective, multicenter study, we sought for the first time to determine the prevalence and risk factors of ID and ID anemia (IDA) in Korean patients with HF.
METHODS
Study population
In the FErrous Renown and UpShot in Korean Acute Heart Failure Patients (FERUS-HF) study, we prospectively enrolled patients hospitalized for acute HF at five tertiary university hospitals from January to November 2019 in Korea (clinical trials.gov: NCT04812873). Patients ≥ 19 years of age who had objective findings of structural and/or functional disorder of the heart with one of the following criteria were enrolled: 1) symptoms of HF, 2) signs of HF, or 3) lung congestion in chest X-ray. Patients who declined consent were excluded. Total 465 patients were enrolled initially in this study, and 4 patients were additionally excluded because of missing laboratory tests.
Study variables and definitions
Routine blood sampling and tests were conducted by laboratories at each center that were certified by the Korean Association of Quality Assurance for Clinical Laboratory at the index admission. Laboratory measurements regarding iron status were performed in laboratories of the participating centers after study enrollment and before discharge. Hematological measurements were performed using fresh venous blood with ethylenediaminetetraacetic acid. Ferritin (ng/mL), serum iron (μg/dL), total iron binding capacity (TIBC, μg/dL), and transferrin (mg/dL) were measured directly. Transferrin saturation was calculated as the ratio of serum iron and TIBC multiplied by 100. ID was defined as serum ferritin < 100 μg/L or ferritin 100–299 μg/L in combination with transferrin saturation of < 20%.1819 Anemia was defined as a hemoglobin concentration of < 12 g/dL in women and < 13 g/dL in men. IDA was defined as the presence of both ID and anemia. Chronic kidney disease (CKD) was defined as estimated glomerular filtration rate < 60 mL/min/1.73 m2.
All echocardiographic studies were performed using a standard ultrasound machine with a 2.5-MHz probe. Left ventricular ejection fraction (LVEF) was measured using Simpson’s biplane method unless this method was not possible. Based on the echocardiographic findings performed at the index acute HF hospitalization, patients were classified into those with HF with reduced ejection fraction (LVEF ≤ 40%), HF with mildly reduced ejection fraction (LVEF, 41–49%), and HF with preserved ejection fraction (LVEF ≥ 50%).222324 Valvular heart disease was defined as greater than mild stenosis or regurgitation, and previous valve surgery.
The primary endpoint was the prevalence of ID and IDA. Anemia and ID treatment was investigated between study enrollment and discharge.
Statistical analysis
Categorical variables are reported as frequencies (percentages). Continuous variables are expressed as means ± standard deviations or medians with interquartile ranges. For comparison between groups, the χ2 test (or Fisher’s exact test when any expected cell count was < 5 for a 2 × 2 table) was used for categorical variables, while the unpaired Student’s t-test or Mann-Whitney U test were used for continuous variables. A logistic regression model was used to determine the predictor of ID and IDA. Variables found to be statistically significant (P < 0.1) in the univariable analysis were included in the final multivariable model, except for variables with > 10% missing values or variables that were closely related to the other variables.
All tests were two-tailed, and a P value < 0.05 was considered statistically significant. Statistical analyses were performed by using R version 4.2.0 (The R Foundation for Statistical Computing, Vienna, Austria) and SAS Version 9.4 (SAS Institute, Cary, NC, USA) by a professional statistician.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Bundang Hospital (B-1811/504-302). Informed consent was submitted by all subjects when they were enrolled. This study complied with the principles of the Declaration of Helsinki.
RESULTS
Patients
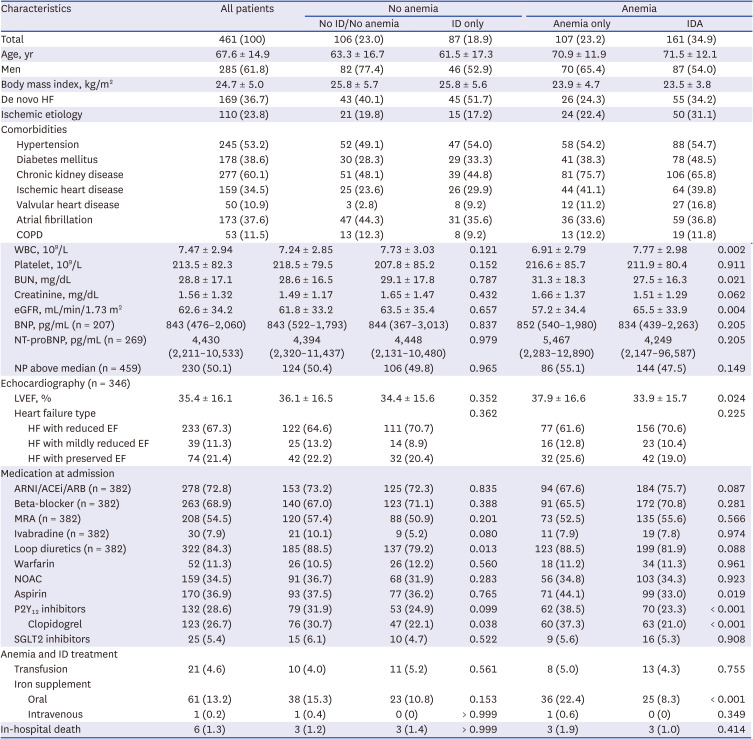
Finally, we analyzed 461 patients with acute HF (Table 1). The mean age was 67.6 ± 14.9 years, and 61.8% were male. Furthermore, 53.2% had hypertension, 38.6% had diabetes, 37.6% had atrial fibrillation, 60.1% had CKD, and 17.8% were current smokers. The mean LVEF was 35.4 ± 16.1%. Based on the hematological measurements, the following mean values were noted: hemoglobin, 12.1 ± 2.4 g/dL; iron, 65.0 ± 39.3 µg/dL; TIBC, 290.5 ± 82.7 µg/dL; transferrin saturation, 23.6 ± 14.6% and ferritin, 224.6 ± 453.8 ng/mL. Regarding antithrombotic medication, 11.3%, 34.5%, 36.9%, and 28.6% received warfarin, new oral anticoagulants, aspirin, and P2Y12 inhibitors, respectively.
Table 1
Baseline characteristics of the study population
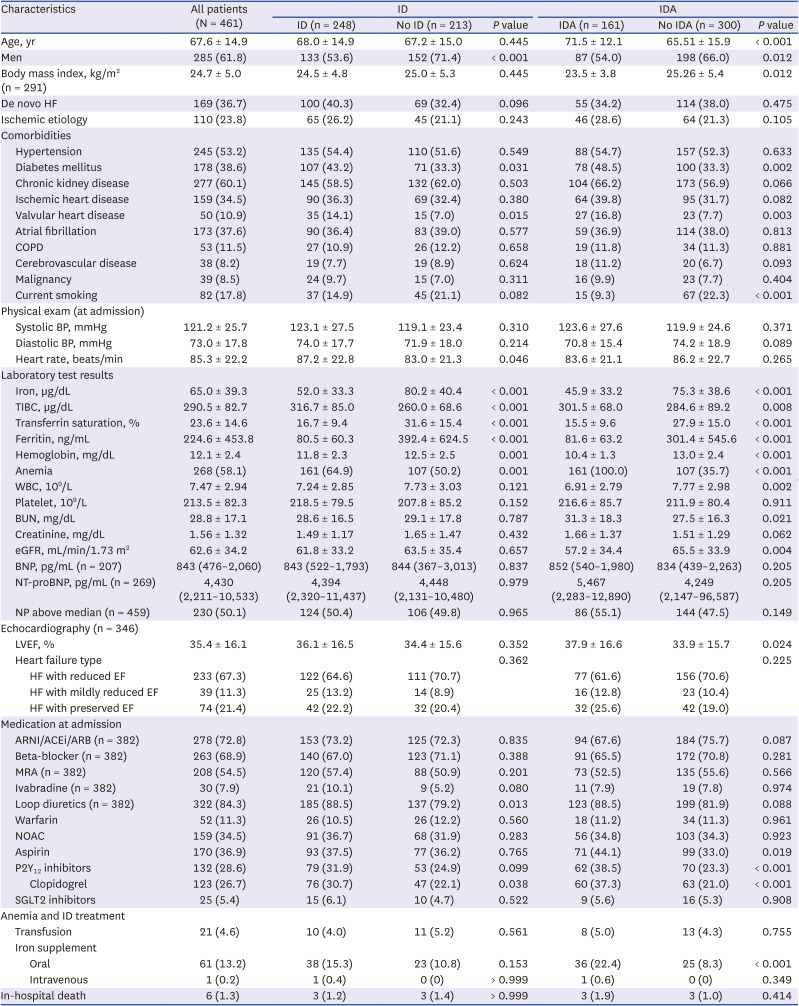
Values are expressed as number (%), mean ± standard deviation, or median (interquartile range).
ACEi = angiotensin-converting enzyme inhibitor, ARNI = angiotensin receptor-neprilysin inhibitor, ARB = angiotensin II receptor blocker, BNP = B-type natriuretic peptide, BP = blood pressure, BUN = blood urea nitrogen, COPD = chronic obstructive pulmonary disease, EF = ejection fraction, eGFR = estimated glomerular filtration rate, HF = heart failure, ID = iron deficiency, IDA = iron deficiency anemia, LVEF = left ventricular ejection fraction, MRA = mineralocorticoid receptor antagonist, NOAC = non-vitamin K oral anticoagulants, NP = natriuretic peptide, NT-proBNP = N-terminal pro-B-type natriuretic peptide, SGLT2 = sodium glucose cotransporter 2, TIBC = total iron binding capacity, WBC = white blood cell.
ID
Among total patients, 53.8% of patients had ID (Fig. 1). Table 1 shows the baseline characteristics of patients with and without ID. Patients with ID were more likely to be female (46.4% vs. 28.6%, P < 0.001), have diabetes (43.2% vs. 33.3%, P = 0.031), have a valvular heart disease (14.1% vs. 7.0%, P = 0.015), and have a higher heart rate (87.2 ± 22.8 beats/min vs. 83.0 ± 21.3 beats/min, P = 0.046). Regarding laboratory findings, patients with ID had lower hemoglobin levels (11.8 ± 2.3 mg/dL vs. 12.5 ± 2.5 mg/dL, P = 0.001) and ferritin levels (80.5 ± 60.3 mg/dL vs. 392.4 ± 624.5 mg/dL, P < 0.001) than patients without ID. The prescription of clopidogrel was more prevalent in the ID group (30.7% vs. 22.1%, P = 0.038). The prevalence of CKD and malignancy did not differ significantly between patients with and without ID. The prevalence of ID was not significantly different between patients with ischemic HF or non-ischemic HF (59.1% vs. 52.1%, P = 0.243).
Fig. 1
Prevalence of various parameters regarding iron deficiency and anemia. (A) Prevalence of iron deficiency. (B) Prevalence of iron deficiency anemia. (C) Prevalence of iron deficiency and iron deficiency anemia. (D) Treatment pattern of anemia.
ID = iron deficiency, IDA = iron deficiency anemia, IV = intravenous.
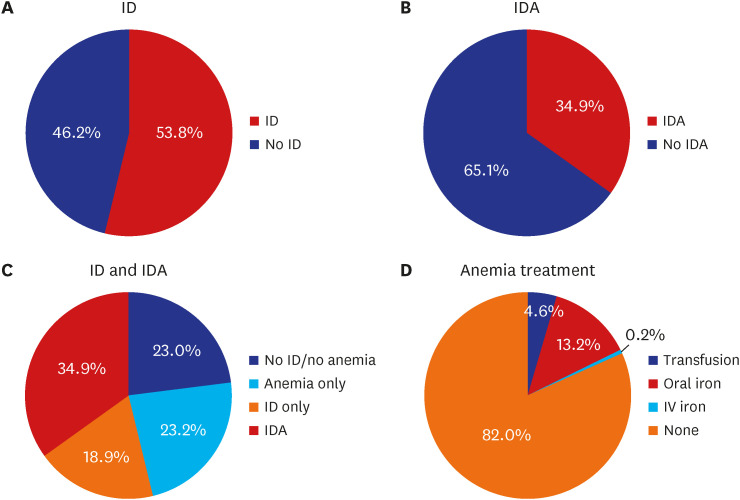
Regarding the treatment of anemia and ID, 4.6%, 13.2%, and 0.2% received blood transfusion, oral iron replacement, and IV iron replacement, respectively. The treatment did not differ between patients with and without ID. Among total 461 patients, 6 patients died before discharge. The in-hospital mortality rate did not differ between ID and non-ID patients (3/248 vs. 3/213; P > 0.999).
Logistic regression models to determine the predictor of ID are shown in Table 2. In the multivariable logistic regression analysis, the independent predictors of ID were female sex (odds ratio [OR], 2.19; 95% confidence interval [CI], 1.47–3.30), valvular heart disease (OR, 2.10; 95% CI, 1.10–4.17), heart rate (OR, 1.10; 95% CI, 1.01–1.21), anemia (OR, 1.60; 95% CI, 1.07–2.40), and the use of clopidogrel (OR, 1.56; 95% CI, 1.00–2.45) (Table 2).
Table 2
Predictors of ID and IDA
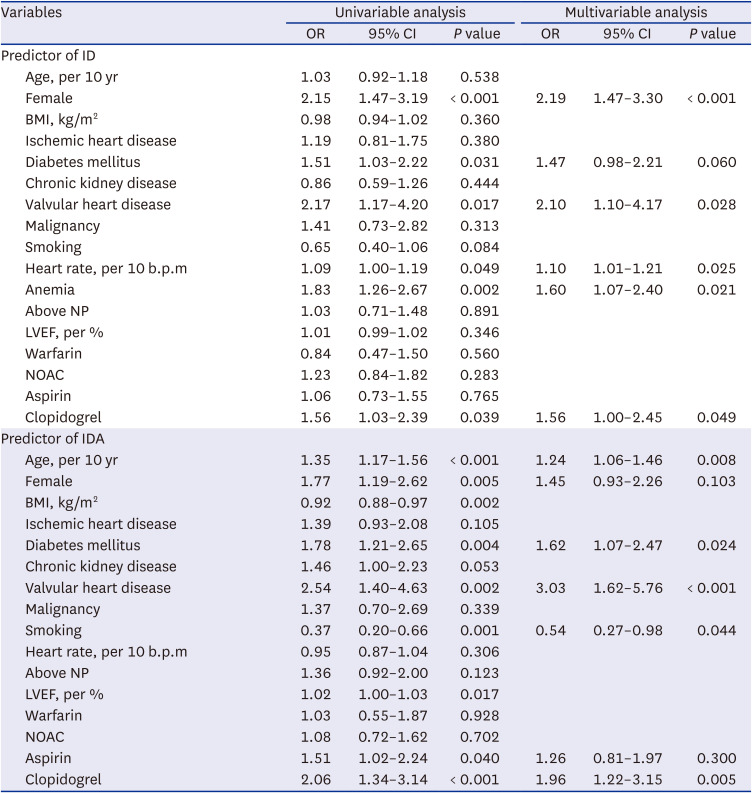
Variables found to be statistically significant (P < 0.1) in the univariable analysis were included in the final multivariable model, except for variables with > 10% missing values or variables that were closely related to the other variables.
BMI = body mass index, CI = confidence interval, ID = iron deficiency, IDA = iron deficiency anemia, LVEF = left ventricular ejection fraction, NOAC = non-vitamin K oral anticoagulants, NP = natriuretic peptide; OR = odds ratio.
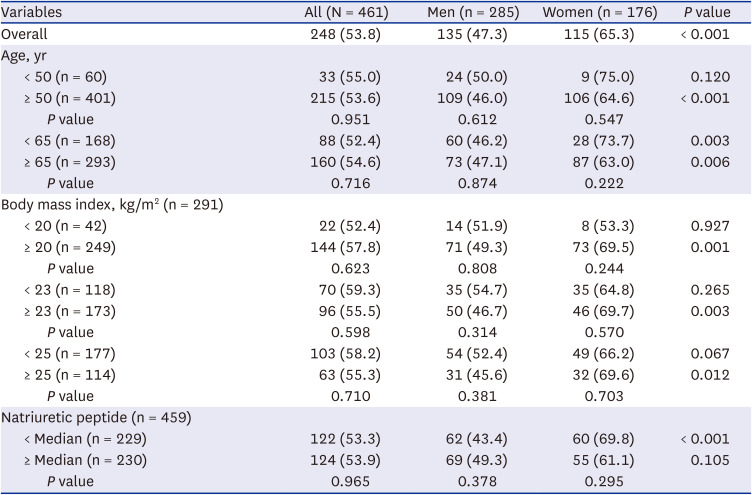
ID in women
Because female sex was the most important predictor of ID, we performed various post-hoc analyses according to sex, age, body mass index (BMI), NP levels and menopause, among others (Table 3). The prevalence of ID was significantly higher in females than in males (65.3% vs. 47.3%, P < 0.001). Interestingly, when stratifying the patients according to age, both the younger and older subgroups of females had a higher prevalence of ID than their male counterparts. Furthermore, there was no difference in the ID prevalence between the younger and older women. Similar findings were observed in subgroups stratified by different BMI cutoffs; females classified with low and high BMI had a trend toward higher ID prevalence than their male counterparts. Again, there was no difference in the ID prevalence between the women with low and high BMI. Similar findings were observed when stratified based on the median NP levels. Lastly, the prevalence of ID did not differ between those with and without menopause (menopause: 103/157 [65.6%] vs. no menopause: 12/19 [63.2%], P = 0.832).
Table 3
Prevalence of iron deficiency according to subtype
IDA
In this study, 34.9% of patients had IDA. They were older, more likely to be female, have diabetes, have valvular heart disease, and use clopidogrel, among others (Table 1). The independent predictors of IDA were older age, diabetes mellitus, valvular heart disease, non-smoking, and the use of clopidogrel (Table 2).
Stratification according to ID and anemia
Next, we classified the patients according to the presence of anemia and ID. Overall, 193 (41.9%) patients had no anemia, while 268 (58.1%) patients had anemia (Table 4). Patients with anemia were older and had a lower BMI than those without anemia. Interestingly, the baseline characteristics were comparable between non-anemic patients with and without ID. The same was true for anemic patients with and without ID. Also, among patients with ID, patients with IDA were more likely to be older and had a lower BMI, higher prevalence of diabetes and CKD, and higher use of aspirin and clopidogrel, and oral iron supplementation than those with non-anemic ID (Supplementary Table 1).
Table 4
Baseline characteristics according to anemia and iron deficiency
Values are expressed as number (%), mean ± standard deviation, or median (interquartile range).
ACEi = angiotensin-converting enzyme inhibitor, ARNI = angiotensin receptor-neprilysin inhibitor, ARB = angiotensin II receptor blocker, BNP = B-type natriuretic peptide, BP = blood pressure, BUN = blood urea nitrogen, COPD = chronic obstructive pulmonary disease, EF = ejection fraction, eGFR = estimated glomerular filtration rate, HF = heart failure, ID = iron deficiency, IDA = iron deficiency anemia, LVEF = left ventricular ejection fraction, MRA = mineralocorticoid receptor antagonist, NOAC = non-vitamin K oral anticoagulants, NP = natriuretic peptide, NT-proBNP = N-terminal pro-B-type natriuretic peptide, SGLT2 = sodium glucose cotransporter 2, TIBC = total iron binding capacity, WBC = white blood cell.
DISCUSSION
The main findings of the current study were as follows: 1) more than half and one-third of the patients hospitalized for acute HF had ID and IDA, respectively; 2) the most important predictor of ID was female sex; and 3) the treatment with IV iron supplementation was very low in these patients.In this study of patients with acute HF in Korea, 53.8% had ID, similar to previous reports. In patients with chronic HF, the prevalence of ID was 50% in an international pooled cohort from Poland, Spain, and the Netherlands,12 61% in 574 community-dwelling HF patients in the United States,25 and 61% among Southeast Asian HF patients.26 Meanwhile, in patients with acute HF, ID was present in up to 80%.2728
We showed that female sex, valvular heart disease, high heart rate, anemia, and the use of clopidogrel were independent predictors of ID. The use of clopidogrel is associated with an increased risk of bleeding, anemia, and iron loss.29 Interestingly, the use of aspirin was not the predictor of ID, which has been reported in other study as well.30 A higher heart rate may be more of a marker rather than a mediator of ID. In our study, CKD and malignancy were not a predictor of ID and IDA. Also, median value of NP and prevalence of NP above the median were not significantly different between patients with ID or without. Furthermore, neither LVEF nor HF type was associated with ID. NP level, which reflects the disease severity of HF, was a powerful predictor of ID in previous studies,13 and the same finding was seen for LVEF.26 The reason for the different results between ours and those may be due to ethnic difference or relatively small sample size of our study. Previous studies suggested that inflammation was associated with ID, and there was more inflammatory milieu in women.3132 Further researches are needed to evaluate the relationship between ID and inflammation.Our study confirmed that female sex is an important predictor of ID, which is in line with previous studies.1226 To elucidate the reasons for this, we performed a few subgroup analyses. The main causes of ID include decreased dietary intake, reduced absorption, and blood loss. The possible causes of ID in HF include cachexia/malnutrition, decreased iron resorption in the intestine due to congestion in the splanchnic area, and decreased iron utilization due to inflammation because HF itself is an inflammatory disease.33
It has been a well-accepted concept that menstruation is the leading cause of ID in females; however, when stratifying the patients according to age (i.e., 50 years and 65 years), the prevalence of ID did not differ between younger and older females, as well as between those with and without menopause. The median age of menopause in Korean women is 50 years.34 These results suggest that blood loss from menstruation is a unlikely cause of ID.26
We believe that stratification by BMI may infer the association between nutritional status and ID. Also, not only malnutrition but obesity is known to be associated with ID.353637 Females had a higher prevalence of ID than males, regardless of their BMI. In addition, there was no difference in the prevalence of ID between females with high and low BMI.
Reduced iron absorption can occur in patients with HF who have poor visceral circulation, i.e., congestion. NP is a hormone that is secreted in the ventricles in response to increased myocardial wall stress, which is proportional to the intra-cardiac pressure.38 As such, the NP level can be used as a surrogate for congestion. Interestingly, females had more ID than males, regardless of NP level. In addition, there was no difference in the ID prevalence between females with high and low NP levels.
Taken together, it is unclear why females have more ID than men with HF. Because ID is an important risk factor for outcomes in HF, further research is warranted.ID occurs in three stages: 1) depletion of iron storage without causing anemia, 2) followed by iron-restricted erythropoiesis, and 3) finally by hypochromic and microcytic anemia. Therefore, one may expect a gradual “aggravation” of the characteristics from normal (no ID/no anemia) to IDA. In this study, the anemic patients had more unfavorable clinical characteristics than the non-anemic patients. More importantly, among the anemic patients, those with and without ID had similar characteristics. The same was observed in the non-anemic patients with and without ID. For example, the mean age of anemic patients with and without ID was 70.9 ± 11.9 years and 71.5 ± 12.1 years, respectively, whereas that of non-anemic patients with and without ID was 63.3 ± 16.7 and 61.5 ± 17.3 years, respectively. These findings have important clinical implications. Because there is no obvious clinical factor that makes the presence of ID highly likely, routine laboratory tests should be performed to detect ID in HF, especially since HF is a disease with increasing prevalence and is associated with high morbidity and mortality.2139
A striking finding was that only 0.2% of patients received IV iron replacement, and 13.2% received oral iron supplements. Oral iron supplementation did not improve the clinical outcomes,40 whereas IV iron replacement with ferric carboxymaltose improved outcomes in both chronic17182041 and acute HF.19 Consequently, current practice guidelines recommend IV iron in patients with HF and ID.222324 Although this study enrollment was performed in 2019, the low prescription rate is alarming. Because the prescription rates of renin-angiotensin system modulators and beta-blockers in Korea are comparable to those of the United States and Europe,2142 both the lack of knowledge and inertia to administer IV iron may be the reasons for the unacceptably low application of adequate ID management.This study has several limitations. First, since this study was conducted at tertiary university hospitals, the results might not be generalized to other settings (e.g., community or primary settings). Second, our study had a relatively small number of patients, and statistical insignificance of prevalence of ID according to age, BMI, median NP levels, and menopause might be due to small sample size. Third, we could not evaluate the impact of presence of ID in the clinical course of HF except for in-hospital mortality because our study focused on the cross-section of patients’ characteristics. It is expected that further research will be possible in the future by collecting long-term clinical outcomes. Fourth, information on co-morbidities including previous surgery, chemotherapy, liver disease, or thyroid disease was missing, although these co-morbidities are likely to be associated with ID and anemia. Fifth, because not all patients were de-novo HF in our study, some patients might already have an oral or IV iron supplement before the index admission which may have affected the iron profile at the index admission. Despite these limitations, this study had certain strengths, showing prevalence of ID in Asian patients with HF.
In conclusion, the prevalence of ID is high in hospitalized Korean HF patients. Because ID cannot be diagnosed by clinical parameters, routine laboratory examinations are necessary to identify patients with ID.
 XML Download
XML Download