

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mortality of critically ill patients has been decreasing in adults and children.1234567 The relative decrease in in-hospital mortality was 35% among adult patients admitted to US intensive care units (ICUs) from 1988 to 2012 and was 20% in New Zealand from 1993 to 2003.12 Multiple reports suggest an approximately 50% decrease in in-hospital mortality among critically ill children in the US and Netherlands in the past 20 years.45 The cause of reduction in mortality is suspected to be multifactorial.4 Along with advances in critical care, including centralization and a dedicated transport system, changes in admission criteria to allow less severe cases in ICUs and changes in end-of-life care to support dying at home rather than in hospitals could all have contributed to the mortality reduction.891011 By monitoring the mortality trends among critically ill children, we can identify key areas of medical practice in need of change and possible areas for improvement.
While mortality trends among adult Korean ICU patients have been reported, there is a paucity of Korean studies regarding mortality trends among critically ill children.12 There have been several changes in the medical environment in Korea. Since 2014, tertiary hospitals have been obligated to have dedicated intensivists in ICUs.13 In 2015, reimbursement codes for pediatric intensive care units (PICUs) have been established. Resident duty hour regulation has been fully implemented in 2017.14 Previous studies focused on mortality covered a relatively short period and did not evaluate trends.151617 Furthermore, studies relying on data from national databases are lacking for Asian children.18
Therefore, we conducted a retrospective cohort study based on the national health insurance database of Korea to evaluate the in-hospital mortality trends among critically ill children.
METHODS
Study population and design
We conducted this population-based, retrospective study based on the Health Insurance Review and Assessment (HIRA) from the Korean Ministry of Health. The HIRA database is composed of reimbursement claims from the Korean National Health Insurance (KNHI) and Medical Aid Program. The KNHI covers 97% of Koreans, and the remaining 3% who cannot afford KNHI are covered by the Medical Aid Program. Therefore, the HIRA database covers all procedures and prescriptions from the Korean population.
Among all pediatric admissions between January 2012 and December 2018 (seven years), admissions of pediatric patients from age 0–18 to ICUs were screened. Neonatal admissions (< 1-month-old) were excluded due to ambiguity in personal identification before birth registration, and neonatal ICU admissions were excluded because Korean neonatal ICUs have a unique organizational structure.
Measurements
The primary outcomes were incidence and mortality trends of pediatric admissions in ICUs. An ICU admission was defined as the presence of at least one ICU admission code during overall hospital admission (AJ001–AJ590). In-hospital mortality was coded in the HIRA admission database.
Demographic characteristics, hospital information, and procedure data were obtained from the KNHI claim database. International Classification of Disease 10th Revision (ICD-10) defines primary diagnosis as a condition with the highest medical resources for diagnosis or treatment during admission.19 Because the KNHI database encodes primary diagnosis under the International Classification of Disease (ICD-10) codes, we defined the primary diagnosis using the ICD-10 as in the previous studies.1720 Use of mechanical ventilation (M5850-M5860), extracorporeal membrane oxygenation (ECMO) (O1901-O1904), and continuous renal replacement therapy (CRRT) (O7001-O7004) were defined by the presence of KNHI procedure codes. Use of vasopressor drugs (dobutamine, dopamine, epinephrine, and norepinephrine) was determined using Korean Drug and Anatomical Therapeutic Chemical codes.
In Korea, critically ill children can be admitted to PICUs or other ICUs, depending on bed availability. Also, not all ICUs are staffed with dedicated intensivists. PICU hospitals were defined as those that report PICU admission codes (AJ004, AJ005, AJ008, AJ009, AJ043, AJ044, AJ045, and AJ046), which differentiate PICU admissions from other ICU admissions within each hospital. Similarly, intensivists were defined according to the presence of codes for dedicated intensivists regardless of pediatric intensivists or intensivists for adult patients (AJ003, AJ005, AJ007, AJ009, and AJ043-AJ046) within each hospital.
Statistical analysis
Continuous and categorical variables are presented as median with interquartile range and number with percentage, respectively. The χ2 test was used for comparing categorical variables of in-hospital mortality. We used univariable and multivariable logistic regression analyses to estimate the odds ratios (ORs) of factors associated with in-hospital mortality of admitted critically ill children. In multivariable regression analysis, we adjusted for age; sex; year of admission; primary diagnosis; department (medical versus surgical); admission path (outpatient clinic versus emergency room); presence of PICU; presence of dedicated intensivists; region (capital versus metropolitan versus rural); and use of mechanical ventilation, ECMO, CRRT, and vasopressors. The P for trend was calculated to evaluate trends in incidence and in-hospital mortality of critically ill children using the Cochrane-Armitage test. A P value < 0.05 was considered significant for all analyses, performed using SAS Visual Analytics (The SAS Institute, Cary, NC, USA).
RESULTS
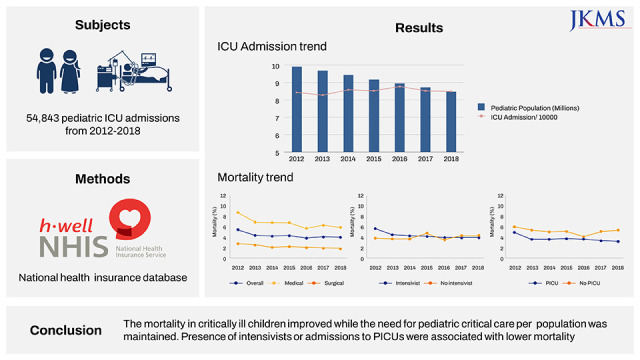
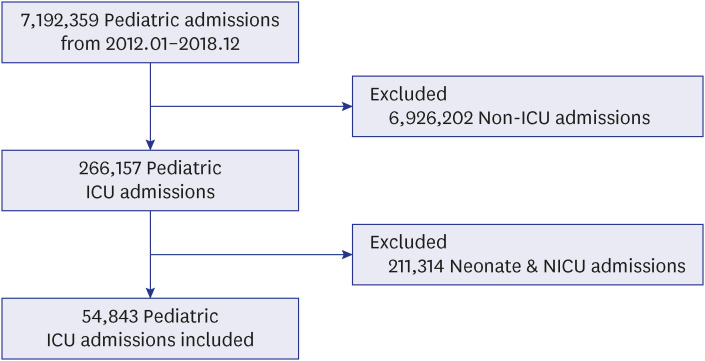
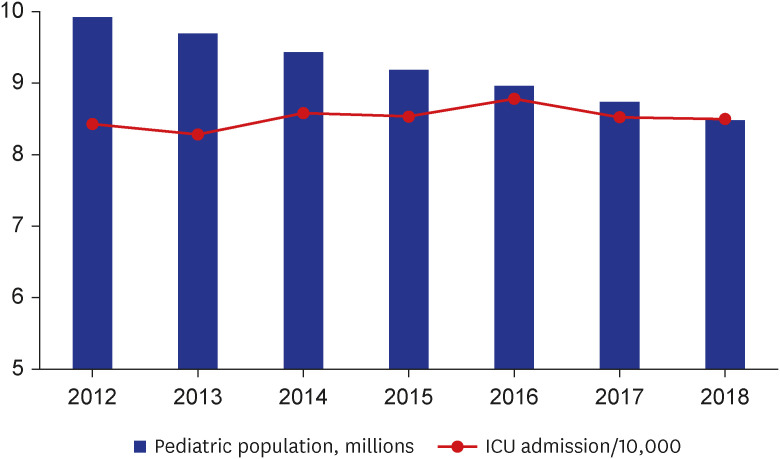
Among 7,192,359 pediatric admissions among children ages 0–18 years during the study period, 266,157 with ICU stay were selected. After excluding 211,314 neonates and neonatal ICU admissions, 54,843 pediatric admissions with ICU stay were selected (Fig. 1). Due to a decreasing fertility rate, the pediatric population decreased from 9,921,012 in 2012 to 8,176,335 in 2018. However, the number of critically ill children remained around 8.5/10,000 population during the study period (P for trend = 0.069) (Fig. 2).
Fig. 1
Flowchart of patient selection.
ICU = intensive care unit, NICU = neonatal intensive care unit.
The median age of children admitted to ICUs was 3.0 years. The most common primary diagnosis was congenital anomaly (31.9%, 17,497 admissions), followed by injury (12.0%, 6,585 admissions), and malignancy (10.2%, 5,575 admissions). Admissions at hospitals with PICUs represented 57.3% (31,415 admissions) of cases, and admissions at intensivist-supported hospitals represented 88.0% (48,276 admissions) (Table 1).
Table 1
Characteristics of pediatric patients admitted to intensive care unit (N = 54,843)
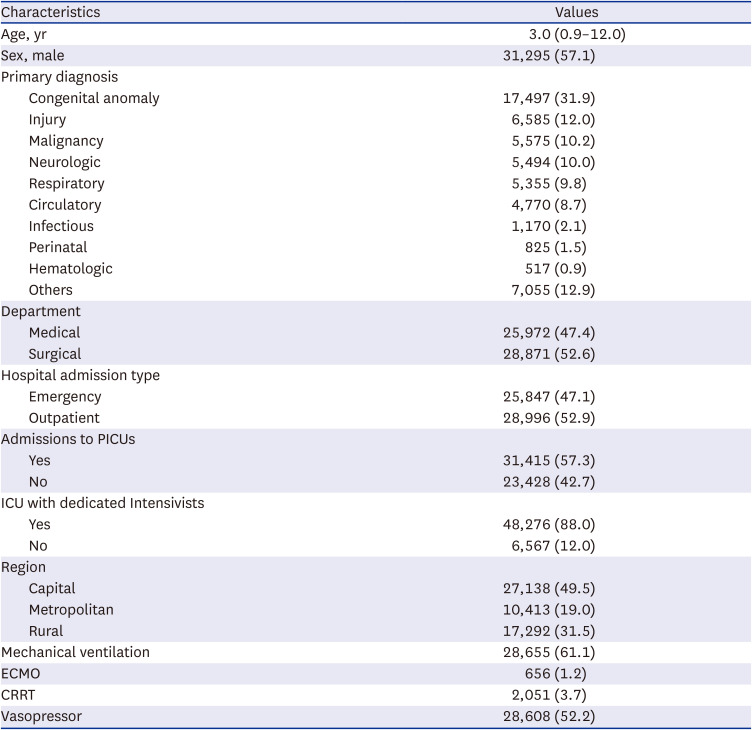
The overall mortality rate was 4.4% (2,396/54,843 admissions). Pediatric ICU admissions via an emergency center (6.1% vs. 2.8%, P < 0.001), admissions in older groups (3.8% in < 1 year, 4.5% in 1–12 years, and 5.0% in ≥ 13 years, P < 0.001), medical department of admission (6.8% vs. 2.2%, P < 0.001), and non-PICU hospitals (5.2% vs. 3.7%, P < 0.001) were associated with higher mortality (Table 2).
Table 2
Incidence and mortality according to the characteristics
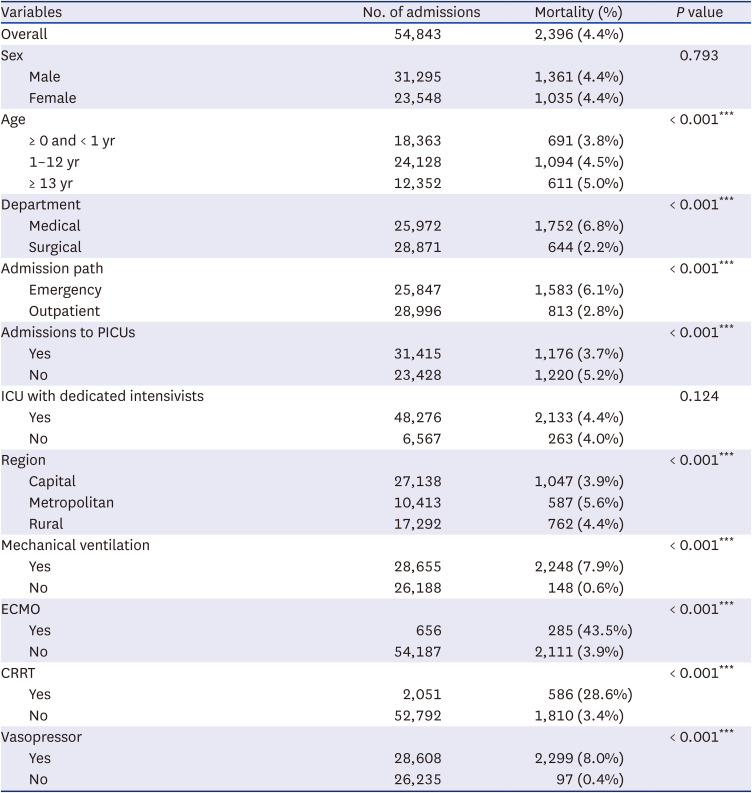
Adjusted logistic regression analysis revealed that admission into the medical department (unadjusted OR, 2.262; P < 0.001 and adjusted OR, 2.918; P < 0.001), admission through the emergency room (unadjusted OR, 2.262; P < 0.001 and adjusted OR, 1.556; P < 0.001), admission to a non-PICU (unadjusted OR, 1.434; P < 0.001 and adjusted OR, 1.962; P < 0.001), and absence of dedicated intensivists (unadjusted OR, 0.903; P = 0.124 and adjusted OR, 1.346; P < 0.001) were associated with higher ORs of mortality. An estimated annual reduction in the OR of mortality was 4.6% (P < 0.001) in the unadjusted model and 11.3% in the adjusted model (P < 0.001) (Table 3).
Table 3
Logistic regression analysis for the mortality risk

| Parameters | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P value | OR | 95% CI | P value | |
| Year of admission | 0.954 | 0.935, 0.974 | < 0.001 | 0.908 | 0.887, 0.930 | < 0.001*** |
Model was adjusted for age, gender, primary diagnosis (congenital anomalies, injury, respiratory disease, neoplasms, neurologic disease, circulatory disease, not elsewhere classified, gastrointestinal disease and infectious disease), and treatment requirements (mechanical ventilation, extracorporeal membrane oxygenation, continuous renal replacement therapy, and vasopressor), department (medical, surgical), hospitals with pediatric intensive care units, intensive care units with dedicated intensivists.
OR = odds ratio, CI = confidence interval.
***P < 0.001.
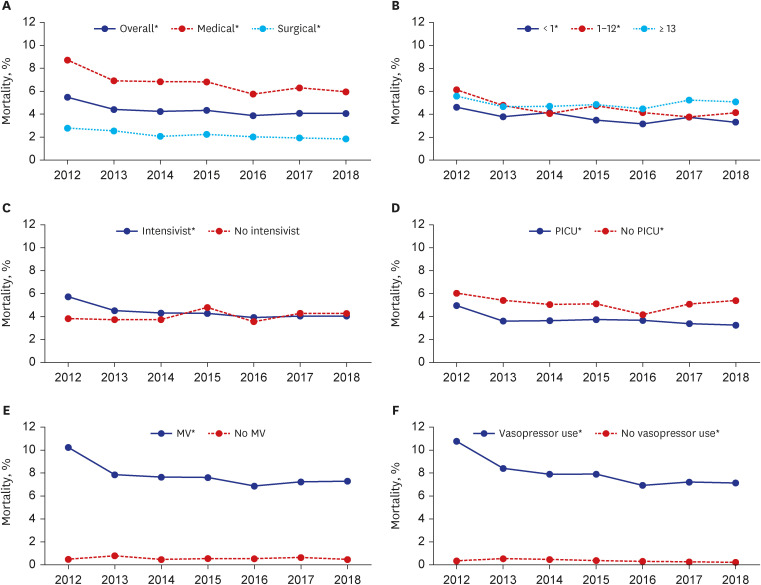
Mortality of critically ill children significantly decreased during the study period, from 5.5% in 2012 to 4.1% in 2018 (P for trend < 0.001). Such a decreasing trend in mortality was observed regardless of admission to a surgical or medical department (P for trend < 0.001 in medical department and P for trend < 0.001 in surgical department) and whether admissions were to a PICU or non-PICU (P for trend < 0.001 in PICU and P for trend = 0.047 in non-PICU). In contrast, a decrease in mortality was significant only in patients younger than 13 years (P for trend = 0.009 in infants and P for trend < 0.001 in 1–12-year-olds) and for admissions to intensivist-supported hospitals (P for trend < 0.001). The mortality trend was not significant in patients older than 13 years (P for trend = 0.731) or with admission to non-intensivist-supported hospitals (P for trend = 0.380). The mortality decrease in non-PICUs (from 6.0% in 2012 to 5.4% in 2018, P for trend < 0.001) was less prominent than in PICUs (from 5.0% in 2012 to 3.2% in 2018, P for trend = 0.047) (Fig. 3, Supplementary Table 1). The decreasing mortality trend was significant among congenital anomalies (P for trend = 0.004), respiratory (P for trend = 0.005) or neurologic (P for trend = 0.003) disease, and malignancy (P for trend = 0.021) (Supplementary Table 2).
Fig. 3
Trend of pediatric mortality of critically ill children in subgroups. Mortality trend in (A) overall, medical, and surgical group, (B) each age group, (C) hospitals with or without dedicated intensivists, (D) hospitals with or without PICUs, (E) admissions with or without mechanical ventilation, and (F) admissions with or without use of vasopressor.
PICU = pediatric intensive care unit, MV = mechanical ventilation.
*Indicates P for trend < 0.05.
DISCUSSION
In this retrospective pediatric population-based study, we showed a decreasing trend in ICU mortality without a changing trend in admission incidence. ICU mortality decreased prominently in severe patients requiring mechanical ventilation or vasopressor as well as in patients admitted to hospitals having a PICU or any ICU managed by intensivists.
Incidence of ICU admission among children in our study was moderate compared with those of previous reports.2122 A study from Australia reported that pediatric ICU admission excluding NICU was 15.1/1,000 hospital admissions, which is higher than our study (7.6/1,000 hospital admissions).21 An epidemiologic study of the United States from 2010–2015 found 2.73–2.84 ICU admissions/1,000 children, including NICU admissions.22 Because these countries have differing medical environments regarding admission criteria, medical facilities, and insurance policies, direct comparisons are not practical. However, the stable incidence of ICU admissions among children in our study suggested a persistent need for pediatric critical care despite a decrease in the pediatric population.
In-hospital mortality of 4.4% among pediatric ICU admissions was comparable to that of a previous study from the United States that reported 4.8% in-hospital mortality from 2005 to 2006.6 The most recently reported in-hospital mortality rate in the United States was 2.8% in 2015, indicating improvement since 2006.5 In-hospital mortality of pediatric ICU patients varies widely from 2.8–12.9% among countries depending on patient characteristics, medical resource availability, and medical practice regarding end-of-life care.56716212324 In this study, there were differences in mortality rates by region (3.9% to 5.6%). We suspect that patient severity or organizational structure, such as bed-to-burse ratio, might affect ICU outcomes.25 Although the mortality rate varied according to study population (medical vs. surgical, tertiary vs. general hospital), our current national study results were similar to those of the United States 15 years ago.
In-hospital mortality decreased by approximately 25% during the study period, from 5.5% in 2012 to 4.1% in 2018, comparable to previous studies in both pediatric and adult populations.1234567 Multiple factors could have contributed to the mortality reduction. A previous study suggested that medical and technological advances, dedicated inter-hospital transport teams, and centralization to tertiary PICUs could improve outcomes for critically ill children.7 In addition to advances in certain pediatric critical care areas, changes in admission criteria and end-of-life care could also affect mortality.46 More permissive admission criteria would more patients admitted with moderate issue severity and lower mortality.
The reduction in mortality was partly explained by a significant decreasing trend in mortality among patients with congenital anomaly or respiratory disease (Supplementary Table 2). Our observation was similar to that of a previous study contributing the decreasing mortality among congenital heart disease patients to the decreasing overall mortality trend.6 In contrast, a mortality decrease was not evident among critically ill children with injury (Supplementary Table 2), which could explain the lack of improvement in mortality among critically ill children older than 13 years. Previous studies have reported higher injury incidence as children age and higher mortality among traumatic ICU admissions among children.1726
Subgroups admitted to PICUs and ICUs with dedicated intensivists showed significantly decreasing trends in mortality in our study. While general ICU admission also showed decreasing mortality trends, the reduction in mortality (from 6.0% to 5.4%, 10% reduction) was smaller compared with that of PICU admission (from 5.0% to 3.2%, 36% reduction). Additionally, ICUs without intensivists did not show decreasing trends in mortality during the study period. Our results were consistent with previous studies that found a benefit of PICUs for critically ill children.272829 A national multicenter cohort study in Finland demonstrated that admission of children to non-PICUs was associated with higher OR of mortality than admission to PICUs even after adjusting for diagnostic group and severity.29 Also, evidence exists in both adult and pediatric populations that the presence of intensivists is associated with improved patient outcomes, including survival.303132 In the only observational study of a pediatric population, Pollack et al.32 found that intensivist-led teams in a PICU improved survival compared to that in a hospital without a PICU. Our study further shows that the reduction in mortality was more prominent if PICUs or intensivists were present. These results suggest that advances in critical care could be better connected to improvements in mortality if appropriate organizational structures are present. Much progress has been made in the field of critical care to improve mortality, including the low tidal volume in managing acute respiratory distress syndrome, shock protocols of surviving sepsis campaign, and application of A to F bundles.333435 Dedicated medical personnel and specialized facilities are required for application of those progress in critical care.
A strength of this study is the inclusion of all hospital data in Korea, which decreased the risk of selection bias. Additionally, a large sample size of critically ill children allowed statistical subgroup analyses of mortality. However, there were also some limitations. First, clinical severity indices were unavailable due to lack of clinical data in the HIRA database. However, information regarding use of mechanical ventilation, CRRT, ECMO, and vasopressors were described. Second, causes and modes of death were not elucidated. Primary diagnosis might not have matched the cause of death. Further studies are necessary to evaluate cause of death to improve end-of-life care for critically ill children.
In conclusion, mortality in critically ill children improved during the study period, and the improving trends were prominent in children with severe disease. Varying mortality trends according to ICU organization highlight that advances in medical knowledge should be supported structurally.
 XML Download
XML Download