

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Immune-mediated inflammatory diseases (IMIDs) are a group of conditions with complex and multifactorial etiology and common inflammatory pathways.12 The IMIDs include several rheumatic and gastroenteologic diseases, comprising rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA), ankylosing spondylitis (AS), psoriatic arthritis (PsA), systemic lupus erythematosus, Crohn’s disease (CD), and ulcerative colitis (UC).2 These diseases, especially RA and inflammatory bowel disease (IBD), are prevalent in reproductive-aged women.3456 Therefore, reproductive health concerns are critical for female patients with IMIDs. Female patients with IMIDs, particularly those with high disease activities, might have higher maternal and perinatal adverse outcomes than healthy populations. Various medications to treat IMIDs could affect these outcomes.47 Self-discontinuing therapies before or during pregnancy due to fear of fetal harm could increase the risk of disease flares and lead to adverse pregnancy outcomes.8910 Biologic agents, including anti-tumor necrosis factor-alpha (TNF-α) agents, non-TNF-α biologics, and Janus kinases inhibitors, are widely used effective therapeutics for various IMIDs such as RA, JIA, AS, PsA, CD, and UC.111213 While several guidelines on the use and safety of biologic agents in women of reproductive age and pregnant women are available for these IMIDs, certainty remains unclear.9141516
As perinatal care is managed by obstetricians, rheumatologists or gastroenterologists (who prescribe biologic agents) may be unable to detect maternal or perinatal complications. Therefore, it would be challenging to conduct a study investigating the effects of biologic agents on pregnancy outcomes in patients with rheumatic diseases and IBD using a hospital-based cohort. Moreover, due to the inadequate sample size in single-center hospital-based approaches, different study methods, such as an approach using a nationwide population database, would be necessary.
Therefore, this study aimed to investigate whether biologic agent exposure was associated with an increase in adverse pregnancy outcomes in patients with rheumatic diseases and IBD using the National Health Insurance Service (NHIS) claims database of South Korea.
METHODS
Data source
This study was a retrospective population-based nationwide study using patient records extracted from the Korean NHIS claims database. The NHIS is the primary social insurance administered by the Korean government, a health insurance system covering 97% of the 50 million Korean population, and a medical aid program covering 3%.17 The NHIS database contains information on patient demographics, diagnosis, medical procedures, operations, and prescriptions.
Study population
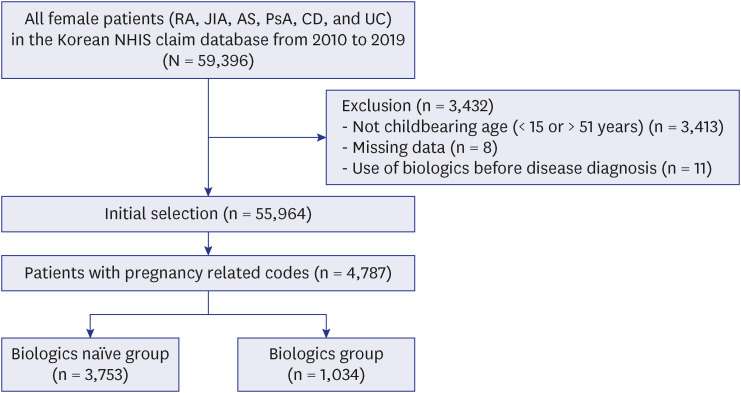
The study population selection process is presented in Fig. 1. The recorded diagnoses were based on the version of the International Classification of Disease 10th revision (ICD-10) modified for the Korean healthcare system and the Korean rare intractable disease (RID) registration code for each disease. In the RID registration program, rare diseases including some rheumatic diseases and IBD, are diagnosed by qualified physicians according to the unified diagnostic criteria distributed by the National Health Insurance. The study cohort included female patients with several rheumatic diseases and IBD between January 2010 and December 2019. The cohort consisted of seropositive RA (ICD-10 code: M05, RID code: V223), JIA (ICD-10 code: M08, RID code: V133), AS (ICD-10 code: M45, RID code: V140), PsA (ICD-10 code: M07, RID code: V237), CD (ICD-10 code: K50, RID code: V130), and UC (ICD-10 code: K51, RID code: V131). We only included patients hospitalized at least once or those who had three or more outpatient visits in 2 years with the corresponding diagnosis. The age of patients was limited to the reproductive age (15–50 years) during the study period.
Fig. 1
Flow diagram of the study population.
AS = ankylosing spondylitis, CD = Crohn’s disease, JIA = juvenile idiopathic arthritis, NHIS = National Health Insurance Service, PsA = psoriatic arthritis, RA = rheumatoid arthritis, UC = ulcerative colitis.
Among the selected patients, we identified pregnant women using the ICD-10 codes associated with pregnancy (codes for labor, abortions or confirmed pregnancies) and procedure codes associated with delivery and abortion (Health Insurance Review and Assessment Service [HIRA] procedure codes for delivery and abortion) (Supplementary Table 1). If a patient had more than one pregnancy during the study period, we only evaluated the first pregnancy to avoid potential bias associated with multiple outcomes from the same patient. The index date was defined as the date of conception, which was defined as the earliest of 38 weeks (266 days) before the delivery date and 14 days before a clinic visit with an ICD-10 code for abortion or confirmed pregnancy.18
The study population was allocated to two groups based on the use of biologic agents before pregnancy-related code records. Biologic agents included etanercept, infliximab, adalimumab, golimumab, tocilizumab, secukinumab, ixekizumab, ustekinumab, vedolizumab, tofacitinib, baricitinib, rituximab, and abatacept.
Additional clinical data were collected from patients, including age, the use of IMIDs-related medications, comorbidities, and the Charlson Comorbidity Index.1920 IMID-related medications include oral non-steroidal anti-inflammatory drugs (NSAIDs), oral glucocorticoids, and immune-modulating agents. The drug exposure of IMID-related medication from rheumatic diseases or IBD diagnosis to the index date was investigated. Long-term glucocorticoid use was defined as using of oral glucocorticoids for 3 months or longer.21 Among these drugs, methotrexate and leflunomide are classified as Federal Drug Administration (FDA) pregnancy category X drugs. Biologic agents and IMIDs-related medications used by the study population were investigated by searching for HIRA formulary codes in the database (Supplementary Table 2).
Study outcomes
The primary endpoint was the impact of prior use of biologic agents on pregnancy outcomes. The secondary endpoints were the effect of the duration of biologic agent exposure and the biologic agent administration during pregnancy on adverse pregnancy outcomes.
Pregnancy outcomes were divided into two categories: 1) live births rate ([total labors minus total abortions or stillbirths]/[total confirmed pregnancies, labors, or abortions]), and 2) adverse pregnancy outcomes. Adverse pregnancy outcomes included six sub-classifications: 2-1) fetal loss (including spontaneous abortion, induced abortion or medical abortion, stillbirth, and ectopic pregnancy), 2-2) preterm delivery, 2-3) preeclampsia/eclampsia, 2-4) gestational diabetes mellitus, excluding those whose condition was diagnosed before pregnancy, 2-5) intrauterine growth retardation, and 2-6) cesarean section. The details of codes for pregnancy outcomes are shown in Supplementary Table 1.
Statistical analysis
Continuous variables were presented as median (interquartile range [IQR]). Categorical variables were presented as frequencies and percentages as assessed using the χ2 and Fisher’s exact tests. We examined the risk of each pregnancy outcome between the biologics and non-biologics groups using multivariate logistic regression models adjusted for recorded diagnosis, age, comorbidities (including Charlson Comorbidity Index, infertility, and previous abortion history), and use of medications (long-term glucocorticoids, NSAIDs, and FDA category X drugs). Adjusted odds ratio (OR) with the 95% confidence interval (CI) were calculated. Statistical significance was determined using two-sided tests, and a P value less than 0.05 was considered significant. All statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
This study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki. The requirement for informed consent was waived by the Institutional Review Board owing to the retrospective nature of the study using a database, and the study was certified by Hanyang University Guri Hospital (No. 2021-04-014-001).
RESULTS
Study population
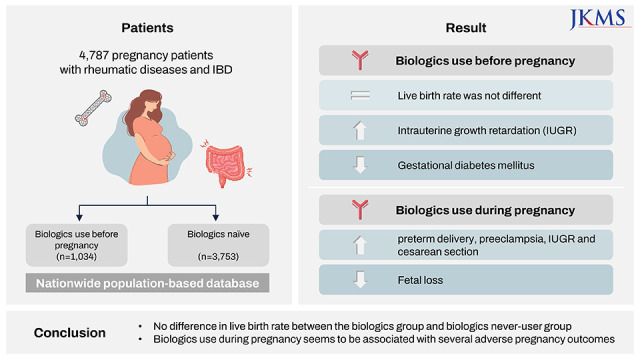
The Korean NHIS database consisted of 59,396 women with RA, JIA, AS, PsA, CD, and UC diagnostic codes between 2010 and 2019 (Fig. 1). Of these women, 55,964 (94.2%) of childbearing age (15–50 years) were identified. Among them, we identified 4,787 (26.8%) women with records of pregnancy-related claims. Finally, we identified 1,034 (21.6%) women who used biologic agents before pregnancy and 3,753 (78.4%) without biologic agent exposure before pregnancy.
Characteristics of the study population
Among the 4,787 participants in the study population, 2,941 (61.4%) were diagnosed with rheumatic diseases (including RA [n = 1,940, 40.5%], JIA [n = 65, 1.4%], AS [n = 900, 18.8%], and PsA [n = 36, 0.8%]) and 1,846 (38.6%) with IBD (CD [n = 582, 12.2%] and UC [n = 1,264, 26.4%]) (Table 1).The individual proportion of use of biologic agents among each disease was 17.9% (348 of 1,940 RA patients), 32.3% (21 of 65 JIA patients), 33.7% (303 of 900 AS patients), 55.6% (20 of 36 PsA patients), 39.9% (232 of 582 CD patients), and 8.7% (110 of 1,264 UC patients). The disease duration was significantly longer in the biologics group than in the biologics naïve group (45.6 vs. 29.1 months, P < 0.001). The median Charlson Comorbidity Index, the proportion of underlying diabetes mellitus and previous history of abortion, was also higher in the biologics group. Long-term glucocorticoid use (≥ 3 months) was more common in the biologics group (57.4% vs. 35.7%, P < 0.001). The rate of exposure to FDA category X drugs (methotrexate and leflunomide) and the rate of other IMID-related drugs use, including NSAIDs and immunosuppressants, was significantly higher in the biologics than in the biologics naïve group (Table 1).
Table 1
Baseline characteristics of the study population
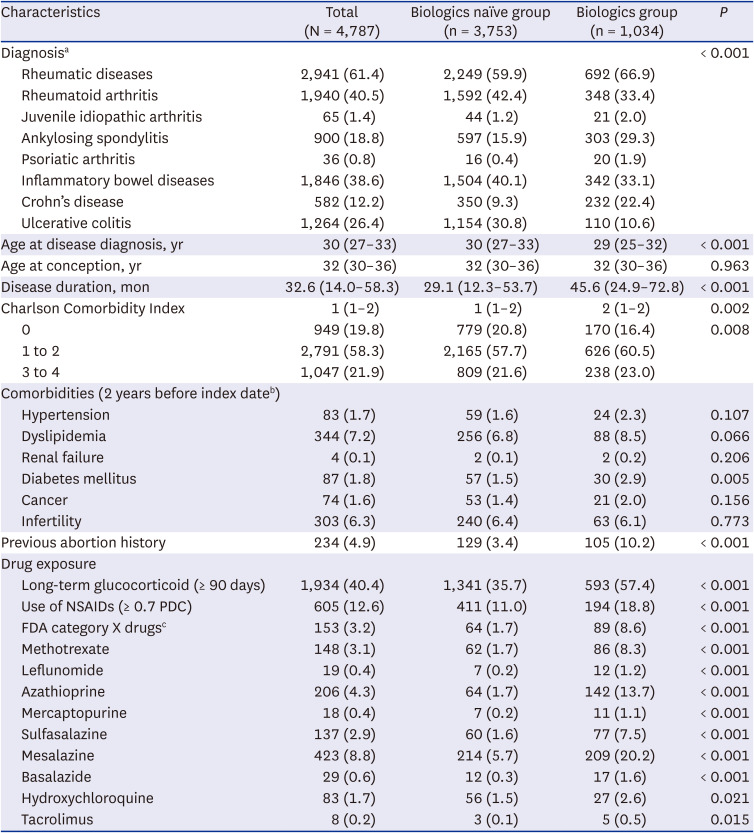
Values are presented as number (%) or median (interquartile range).
FDA = Federal Drug Administration, NSAIDs = non-steroidal anti-inflammatory drugs, PDC = proportion of days covered.
aThe proportion of the use of biologics was 17.9% (348 of 1,940) in rheumatoid arthritis), 32.3% (21 of 65) in juvenile inflammatory arthritis, 33.7% (303 of 900) in ankylosing spondylitis, 55.6% (20 of 36) in psoriatic arthritis, 39.9% (232 of 582) in Crohn’s disease, and 8.7% (110 of 1,264) in ulcerative colitis.
bIndex date was defined as the date of conception.
cFDA category X drugs including methotrexate and/or leflunomide.
Characteristics of the biologics group
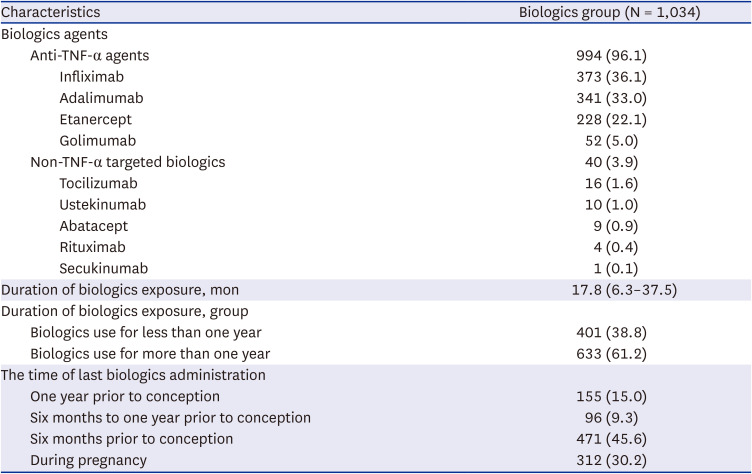
Table 2 shows the details of the biologics group. Anti-TNF-α agents (n = 994, 96.1%) were the most frequently used biologic agents, of which infliximab (n = 373, 36.1%) was the most common, followed by adalimumab (n = 341, 33.0%), etanercept (n = 228, 22.1%), and golimumab (n = 52, 5.0%). No patients received ixekizumab, vedolizumab, tofacitinib, or baricitinib. The median duration of biologic agent exposure was 17.8 months. In addition, 633 patients (61.2%) used biologic agents for more than one year and 312 (30.2%) were administered their last biologic agent during pregnancy. Among the patients who used biologics during pregnancy, 304 (97.4%) were anti-TNF-α agents users and 8 were non-TNF biologics users (tocilizumab [n = 4], ustekinumab [n = 2], abatacept [n = 1], and secukinumab [n = 1]). The median duration of use of biologics during pregnancy and the postpartum period in these patients was 154 days (IQR, 33–238 days).
Table 2
Characteristics of the biologics group
Pregnancy outcomes
The total live birth rates for the biologics and biologics naïve groups were 75.0% and 75.2%, respectively (Table 3). No statistically significant differences were observed in the rates of fetal loss (including spontaneous abortion, induced abortion, stillbirth, and ectopic pregnancy) between the two groups (Table 3). Preterm delivery was observed in 539 patients (11.3%), with no significant difference between the two groups. However, the rate of gestational diabetes mellitus in the biologics naïve group was significantly higher than that in the biologics group (35.3% vs. 29.1%, P < 0.001). Intrauterine growth retardation was observed in 131 patients (2.7%), significantly higher in patients exposed to biologic agents (4.2% vs. 2.3%, P = 0.002). In addition, the rate of cesarean section in patients with delivery codes (vaginal delivery codes plus cesarean delivery codes) was significantly higher in the biologics group than in the biologics naïve group (58.8% vs. 48.3%, P < 0.001). To define the factors associated with adverse pregnancy outcomes, multivariate analyses (adjusted for possible confounding factors [recorded diagnosis, Charlson Comorbidity Index, long-term glucocorticoid use, NSAIDs use, FDA X drugs exposure, age, and history of infertility and abortion]) showed that biologic agents use was associated with a higher risk of intrauterine growth retardation (OR, 1.780; 95% CI, 1.182–2.680) and lower risk of gestational diabetes mellitus (OR, 0.776; 95% CI, 0.658–0.914) compared with the biologics naïve group. However, the risk of fetal loss, preterm delivery, preeclampsia/eclampsia, and cesarean section were not significantly different between the biologics and biologics naïve groups in the multivariate analysis (Table 4). In a subgroup analysis targeting only the anti-TNF-α agent group (n = 994), preterm delivery, intrauterine growth retardation, and cesarean section were significantly higher and gestational diabetes mellitus was lower in the anti-TNF-α agent group than in the biologics naïve group (Supplementary Table 3). Also, anti-TNF-α agent use was associated with a higher risk of intrauterine growth retardation, cesarean section, and lower risk of gestational diabetes mellitus (Supplementary Table 4). Furthermore, a subgroup analysis was conducted to exclude unintended pregnancy from fetal loss, excluding ‘induced abortion’ or ‘medical abortion’ from fetal loss. In this subgroup analysis, the use of biologics also increased the risks of intrauterine growth retardation, and cesarean section, and decreased the risk of gestational diabetes mellitus (Supplementary Table 5).
Table 3
Pregnancy outcomes
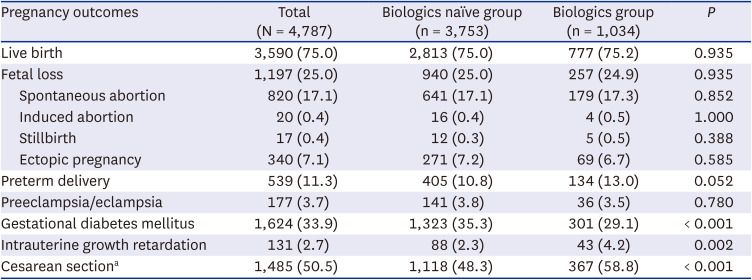
Table 4
Effects of biologics on adverse pregnancy outcomes
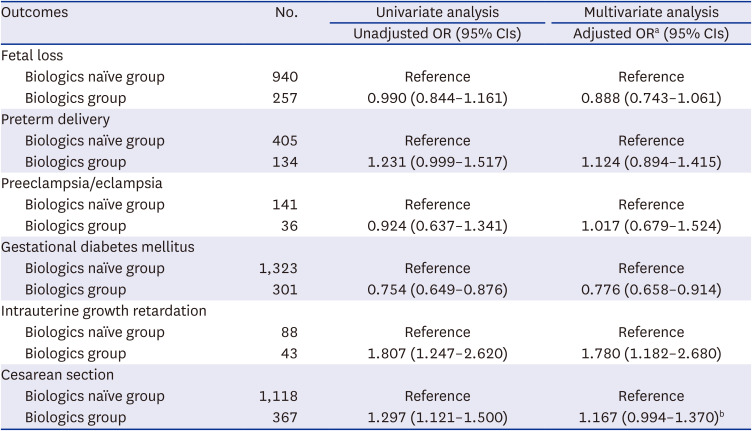
CI = confidence interval, OR = odds ratio, FDA = Federal Drug Administration.
aAdjusted for recorded diagnosis, age, Charlson Comorbidity Index, previous long-term use of glucocorticoids, non-steroid anti-inflammatory drugs, and FDA category X drugs, previous history of infertility, and abortion.
bAdjusted for recorded diagnosis, age, Charlson Comorbidity Index, previous long-term glucocorticoid use, non-steroidal anti-inflammatory drugs, and FDA category X drugs, previous history of infertility, abortion, and cesarean section.
The risk of adverse pregnancy outcomes according to the duration of biologic agent exposure before pregnancy and administration of biologics during pregnancy
We performed the subgroup analysis according to the duration of biologic agent exposure whether it was used for more than one year or less than one year, by logistic regression analysis. In both groups who used biologics for more than 1 year or less than 1 year prior to pregnancy, the risk of cesarean section was increased, the risk of gestational diabetes was decreased, and fetal loss and preeclampsia/eclampsia were not significant compared to the biologics naïve group. Also, compared with the biologics naïve group, the risk of preterm delivery and intrauterine growth retardation was significantly higher only in the group that used the biologic agents for more than one year but not in the group for less than one year (Table 5). In multivariate analysis adjusted for possible confounding factors, only intrauterine growth retardation was significantly increased in the group that used biologic agents for more than one year compared with the biologics naïve group (OR, 2.053; 95% CI, 1.291–3.265), whereas the significance of the increased risk of preterm delivery and cesarean section disappeared. In addition, the risk of gestational diabetes mellitus was still significantly lower in multivariate analysis (biologics use for less than one year: OR, 0.772; 95% CI, 0.610–0.977, biologics use for more than one year: OR, 0.778; 95% CI, 0.638–0.949) (Table 5). Table 6 shows the effect of the biologic agent administration during pregnancy on adverse pregnancy outcomes. The multivariate analysis adjusted for possible confounding factors showed that the patients who received biologic agents during pregnancy were significantly associated with increased risk of preterm delivery (OR, 1.859; 95% CI, 1.535–2.554), preeclampsia/eclampsia (OR, 1.762; 95% CI, 1.003–3.006), intrauterine growth retardation (OR, 3.487; 95% CI, 2.109–5.767), and cesarean section (OR, 1.831; 95% CI, 1.430–2.344), but decreased risk of fetal loss (OR, 0.274; 95% CI, 0.183–0.411). The results of the subgroup analysis excluding unintended pregnancy also showed no significant difference from previous results (Supplementary Tables 6 and 7).
Table 5
Effects of biologics duration on adverse pregnancy outcomes
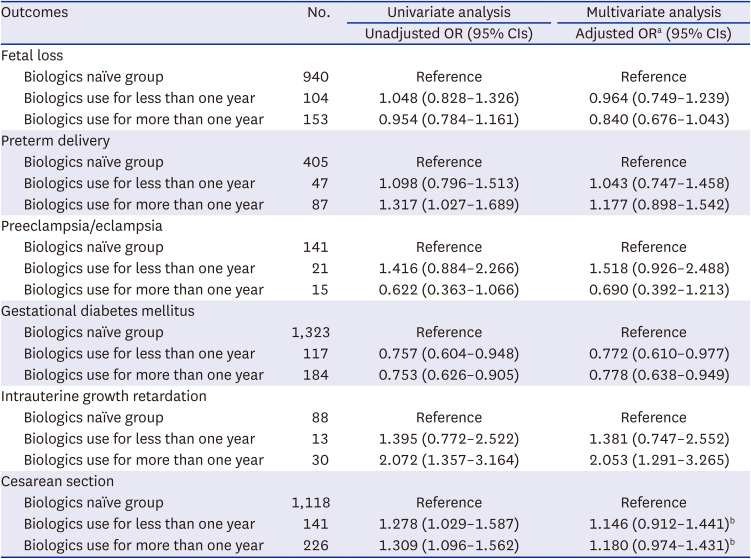
CI = confidence interval, OR = odds ratio, FDA = Federal Drug Administration.
aAdjusted for recorded diagnosis, age, Charlson Comorbidity Index, previous long-term glucocorticoids use, non-steroidal anti-inflammatory drugs, and FDA category X drugs, previous history of infertility, and abortion.
bAdjusted for recorded diagnosis, age, Charlson Comorbidity Index, previous long-term glucocorticoid use, non-steroidal anti-inflammatory drugs, and FDA category X drugs, previous history of infertility, abortion, and cesarean section.
Table 6
Effects of the biologics administration during pregnancy on adverse pregnancy outcomes
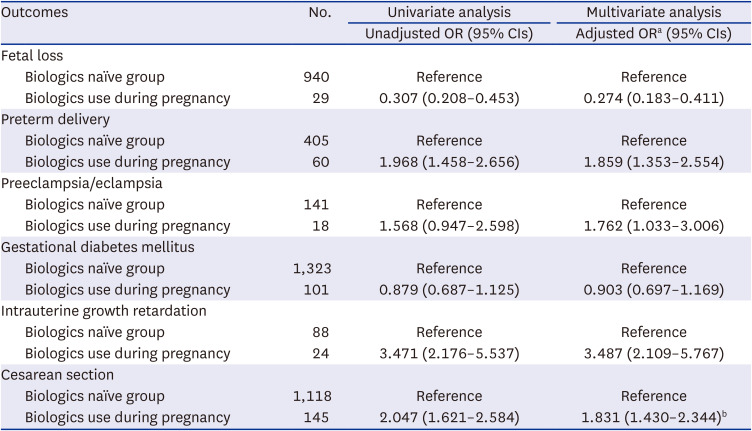
CI = confidence interval, OR = odds ratio, FDA = Federal Drug Administration.
aAdjusted for recorded diagnosis, age, Charlson Comorbidity Index, previous long-term use of glucocorticoids, non-steroid anti-inflammatory drugs, and FDA category X drugs, previous history of infertility, and abortion.
bAdjusted for recorded diagnosis, age, Charlson Comorbidity Index, previous long-term glucocorticoids use, non-steroidal anti-inflammatory drugs, and FDA category X drugs, previous history of infertility, abortion, and cesarean section.
DISCUSSION
This population-based study using the Korean NHIS claims database found that there was no significant difference in live births between the biologics user and biologics naïve groups in patients with several rheumatic diseases and IBD. The risk of intrauterine growth retardation was higher in the biologics group than in the biologics naïve group; however, the risk of gestational diabetes mellitus was lower. In addition, patients treated with biologic agents for longer than one year showed an increased risk of intrauterine growth retardation but not those treated for less than one year. Patients who received biologic agents during pregnancy were significantly associated with increased risk of preterm delivery, preeclampsia/eclampsia, intrauterine growth retardation, and cesarean section but decreased risk of fetal loss.
In the study, the proportion of patients who used biologic agents before and/or during pregnancy was approximately 22% among the female patients of childbearing age with. This proportion was ten times more than that in the previous study using British Columbia population data, which reported that 2.1% of women with autoimmune diseases were exposed to biologic agents during preconception and pregnancy between 2002 and 2012.22 Furthermore, compared with previous studies on female patients with AS and IBD using the Korean nationwide claims database, the proportion of patients using biologics was approximately twice as high in this study.2324 These findings may be due to several reasons: the recent trend of more frequent prescription of biologics, increasing number of biologic agents, expansion of indications for each biologic agent as a result of proven efficacy, and the different operational definitions of the patient groups between studies.111225 Moreover, recently published treatment guidelines for some IMIDs are more favorable for biologic agents use, such as anti-TNF- α agents than the previous guidelines. For example, in 2020, the American College of Rheumatology released guidelines recommending conditional continuation of anti-TNF-α agents before and during pregnancy.16 In addition, recent treatment guidelines for IBD also recommend continued anti-TNF-α agents during pregnancy.1415 Moreover, in a recent small hospital-based study of patients with AS in Korea, 28.6% (6 of 21) of patients had a history of biologic agent use before pregnancy, similar to the findings in our study (1,034 of 4,787 patients, 21.6%).26
Intrauterine growth retardation is a heterogeneous condition that results in small babies for their gestational age due to several causes, including congenital malformations, infections, or placental insufficiency.27 The level of TNF-α was significantly higher in the intrauterine growth retardation group with placental insufficiency than in the healthy control group; however, no difference was observed in the intrauterine growth retardation group with the other causes.27 Previous studies from Denmark, Finland, and Sweden population cohorts reported that the anti-TNF-α agent was significantly associated with a higher OR for small for gestational age (1.36) compared with biologics naïve.28 In a meta-analysis of eight prospective studies, anti-TNF-α agents had a significantly higher risk of small for gestational age (OR, 1.43).29 Corroborating these previous results, our study also showed that intrauterine growth retardation was associated with biologic agent use (OR, 1.780). In particular, the risk of intrauterine growth retardation was significantly higher in the groups that used the biologic agents for more than one year (OR, 2.053) and during pregnancy (OR, 3.487) than in the biologics naïve group. Furthermore, the risk of preterm delivery was significantly higher in the group that used biologic agents during pregnancy (OR, 1.859) than in the biologics naïve group. While immunosuppression due to biologic agents might increase peripartum infection, further studies to explore underlying basic mechanisms for the association of biologics during pregnancy with preterm delivery and intrauterine growth retardation are needed.28
In this study, the proportion of patients who underwent cesarean section was 50.5%, which was significantly higher in the group using biologic agents than in the group without biologic agents (58.8% vs. 48.3%, P < 0.001). The cesarean section rate in Korea is the highest worldwide, maintained at over 35% since the 2000s.30 Previous studies have shown that women with IBD/AS have a higher cesarean section rate than the general population.23313233 In a study using Korean claim data between 2007 and 2017, the cesarean section rate was highest among women with AS (50.8%), followed by RA (44.1%) and the general population (38.0%).33 In another study using the Korean NHIS claim database, cesarean sections were performed more often in women with CD (46.5%) or moderate to severe IBD patients (46.4%) than in the general population (38.8%).23 In a hospital-based study in Korea, the cesarean section rate was twice as high in AS compared with that in women without any autoimmune disease.26 In a study in Norway, women with inflammatory rheumatic diseases (RA, JIA, and AS) had significantly higher rates of cesarean section than those without rheumatic diseases.34 Results from Denmark, Finland, and Sweden population-based studies showed that women with IMIDs treated with anti-TNF-α agents had a higher risk of cesarean section (OR, 1.57) than biologics non-users.28 In particular, in our study, the cesarean section was significantly higher with the use of biologic agents during pregnancy compared with the biologics naïve group. Therefore, consistent with this study and the previous ones, the biologic agents seem to affect the implementation of the cesarean section in IMID patients. However, it should be cautioned that these findings might have been influenced by the severity of the IMID disease requiring biologic agents.
The risk of gestational diabetes mellitus was lower (OR, 0.776) in the biologics group than in the biologics naïve group in this study, suggesting the possibility that anti-TNF-α agents prevent the progression to gestational diabetes mellitus. No previous study has shown that biologic agent use might reduce the risk of gestational diabetes in patients with rheumatic diseases and IBD. Patients with RA and IBD might be at risk of insulin resistance.3536 Several studies have shown that pro-inflammatory cytokines, such as TNF-α and interleukin-6, are associated with insulin resistance; biologic agents that inhibit these cytokines could decrease the risk of diabetes mellitus by increasing insulin sensitivity.373839 Notably, anti-TNF-α agents were associated with a significant reduction in the risk of diabetes mellitus in patients with RA, and showed a favorable effect on insulin sensitivity in IBD patients.3640 Moreover, a study showed that increased TNF-α levels are associated with gestational diabetes mellitus.41 While the previous studies could explain the underlying mechanisms of reduced risk of gestational diabetes mellitus in the biologics group in the present study, the other possibilities such as concomitant glucocorticoid use and disease activity of this association should be addressed, which could not be addressed due to lack of data in the current study. Though the use of biologics during pregnancy showed a tendency to lower the risk of gestational diabetes compared to the non-use of biologics, no statistical significance was obtained (OR, 0.903; 95% CI, 0.697–1.169).
In the study, fetal loss and preeclampsia/eclampsia showed no association with ever-exposure to biologic agents. TNF-α affects hormone synthesis, placental structure, and embryonic development during pregnancy.42 Studies have shown that increased TNF-α levels are associated with fetal loss.43 In addition, some anti-TNF-α agents (adalimumab and etanercept) have effectively treated women with recurrent miscarriages or repeated in vitro fertilization failure.44 In 2004, Katz et al.45 reported no increase in spontaneous abortion rates in a group of 96 pregnant women with RA and CD treated with infliximab compared with the general population. A meta-analysis study showed that fetal loss (including therapeutic abortion and spontaneous abortion) was not significantly different between anti-TNF-α agent users and non-users during pregnancy.29 Another recent meta-analysis study reported no difference in the rates of miscarriage or preeclampsia with the use of biologic agents during pregnancy.46 These previous studies are consistent with the present study regarding biologic agent use not affecting overall fetal loss. Interestingly, we found that the risk of fetal loss in the patients who used biologics during pregnancy was significantly decreased, which needs to be confirmed in further studies with larger sample sizes.
Notably, in our study, biologics use during pregnancy was associated with an increased risk of adverse pregnancy outcomes including preterm delivery, preeclampsia/eclampsia, intrauterine growth retardation, and cesarean section. While, in a small hospital-based study of 18 patients with IBD, there were no pregnancy-related complications such as premature or stillbirths among patients who used biologics during pregnancy.47 Although disease activity decreases during pregnancy in patients with IMIDs, especially RA and IBD, active disease during pregnancy can lead to adverse pregnancy outcomes such as fetal loss, stillbirth, preterm delivery, and cesarean section.48495051 Also, in a meta-analysis, women with IMIDs treated with anti-TNF-α agents showed a significantly increased risk of preterm delivery, spontaneous abortion, and low birth weight than the general population; however, anti-TNF-α non-users also showed similar results, suggesting the contribution of disease itself to the adverse pregnancy outcomes.52 The increase in pregnancy complications in patients who used biologics during pregnancy may be attributed to the patient’s high disease activity rather than biologics.
This study had some limitations. First, the NHIS claims database lacks detailed clinical information on individual patients, such as laboratory findings, disease activities, radiological findings, and lifestyle factors. Since the biologics group is estimated to have higher disease activity than the biologics naïve group, many patients with severe disease activity might be included in the biologics group, which may have resulted in poor pregnancy outcomes such as intrauterine growth retardation. Second, the results of neonatal complications, including congenital anomalies and low birth weight, were unknown because mother-infant pairs were not established. Therefore, further hospital-based studies are needed to confirm the effect of disease activity on pregnancy and fetal outcomes in the biologics group. Third, the precise gestational weeks at the time of delivery and abortion were unknown. Therefore, since the exact exposure time of biologic agents was unclear, we defined the conception date using the operational definition according to the previous literature, which defined it as the earliest of 38 weeks (266 days) before the date of delivery and 14 days before a clinic visit with an ICD-10 code for abortion or confirmed pregnancy.18 However, in cases of extremely preterm birth, the index date may be significantly earlier than the actual conception date. Fourth, most participants used anti-TNF-α agents, and few used non-TNF agents. Therefore, further research should examine the association of pregnancy outcomes with non-TNF biologics. Fifth, the biologics group included patients who used the biologic agent even once in the study. Sixth, it is not possible to obtain drug compliance from the claim data, and prescription itself alone may not accurately reflect the actual individual patient's biologics use. Therefore, further hospital-based studies are needed to verify that the prescribed biologics have actually been administered. To compensate for this limitation, arbitrary criteria for the duration of the biologics use for more than one year or less than one year were set to perform the subgroup analysis for adverse pregnancy outcomes in the present study. However, further studies are needed to analyze more details about the duration of drug exposure and the time points of administration prior to pregnancy, considering the half-life of the biologic agents. Despite these limitations, a major strength of this study was that it used the largest possible population data, a nationwide claims database, to investigate the impact of exposure to biologic agents on pregnancy outcomes in patients with rheumatic diseases and IBD.
In conclusion, the present study using nationwide population data may improve the understanding of the impact of biologics on the pregnancy prognosis of patients with rheumatic diseases and IBD. This study showed that patients treated with biologic agents had live births and fetal loss comparable to the biologics naïve group and lower risk of gestational diabetes mellitus than the biologics naïve group. However, biologics use seems to increase the risk of intrauterine growth retardation and cesarean delivery, especially patients with biologics use during pregnancy. Therefore, clinicians who prescribe biologics during pregnancy need to collaborate with obstetricians for screening and management of pregnancy complications.
 XML Download
XML Download