

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In the midst of the coronavirus disease 2019 (COVID-19), vaccines have been rapidly developed and introduced under emergency use authorization around the world. The messenger RNA (mRNA) vaccine, BNT162b2 (Pfizer/BioNTech), was the first COVID-19 vaccine accepted by the World Health Organization (WHO)1 and used widely together with mRNA-1273 (Moderna), based on their high efficacy (> 94%) in phase-3 trials.23 In South Korea, BNT162b2 and mRNA-1273 have been rolled out since February 27, 2021, and June 18, 2021, respectively. Primarily, adults aged < 60 years were the main targets of these vaccines, which then expanded to all populations aged ≥ 5 years by May 2022, resulting in a vaccine coverage rate of > 80%.4
Given the limited public health experience with this novel vaccine platform and potential movement toward annual COVID vaccination strategy like influenza immunization, it is important to identify and monitor the safety of mRNA vaccines.56 In phase-3 trials, major adverse events (AEs) after vaccination were mild-to-moderate and transient events including injection site pain (66.0–88.2%), fatigue (34.0–65.3%), and headache (25.0–58.6%). The incidence of serious AEs was rare (0.6%) and was similar in the vaccine and placebo groups.23 Following the COVID-19 vaccination, surveillance studies using government-sponsored reporting system database, health record data, or real-time data from mobile applications were conducted to evaluate the real-world safety of mRNA vaccines with an understanding of the clinical trial limitations.789101112 The studies found reassuring results with respect to the acceptable safety profile of the vaccines; however, they mainly focused on AEs reported in the phase-3 trials, which did not reflect the safety concerns recently raised (e.g., menstrual disorder and hair loss), and the results of those studies would likely be limited to under-reporting bias. Furthermore, less safety data exists focusing on young adults, since previous studies largely included participants aged > 50 years. Also, few studies identified the factors associated with AEs after mRNA vaccination. Worldwide proportion of people fully vaccinated is 62.2% as of September 2022,13 and people not vaccinated due to concerns about the AEs of COVID-19 vaccines also exist, thereby information on the risk factors for AEs is required.
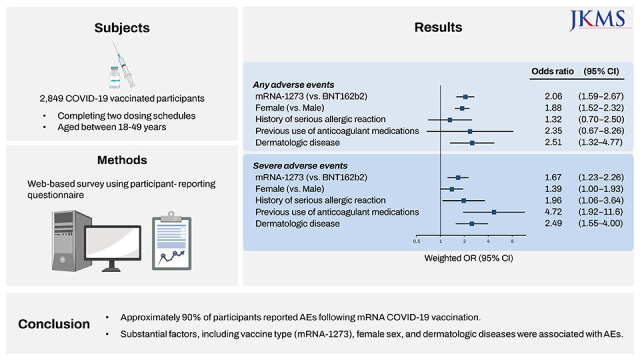
This study aimed to investigate a population-based safety profile of mRNA COVID-19 vaccines and to identify factors associated with participant-reported AEs following mRNA COVID-19 vaccination using nationally representative survey data generated from a population aged between 18–49 years in Korea.
METHODS
Design, setting, and participants
We conducted a cross-sectional, web-based survey between December 2–10, 2021. Gallup Korea, an affiliation of Gallup International, distributed a survey invitation incorporating general concepts, purpose, and informed consent via e-mail to online panels stratified according to age, sex, and region to represent the Korean population. Participants were enrolled if they met the inclusion criteria of the study: 1) individuals who had elapsed at least two weeks after completing both doses of COVID-19 vaccination, and 2) individuals aged 18–49 years. We defined these criteria considering the timing of implementing a nationwide mass vaccination of mRNA COVID-19 vaccine to the general population aged 18–49 years in Korea. We also enrolled participants who received a heterologous vaccine of COVID-19 (adenoviral vector vaccine as the first dose and subsequent mRNA vaccine, or BNT162b2 as the first dose and subsequent mRNA-1273 or vice versa) as the government allowed heterologous vaccination in a similar period of mass vaccination. After enrollment, the participants provided responses regarding their baseline characteristics, COVID-19 vaccination status, and AEs. We then weighted the study participants to adjust for under- or over-coverage from the expected distributions of age, sex, and regional strata derived from the Korean population. A detailed explanation of minimal sample size calculation, participant rewards, the weight calculation methods, etc. is provided in the Supplementary Data 1.
Questionnaires
We developed participant-reporting questionnaires to identify the overall incidence of AEs. The contents of the questionnaire were as follows: 1) demographic and clinical characteristics including age, sex, education level, smoking status, alcohol consumption status, occupation, body mass index (BMI), comorbidities (e.g., diabetes, hypertension, cardiovascular diseases, cancer, autoimmune diseases, dermatologic diseases, respiratory diseases, renal diseases, liver diseases, neurological diseases, and other unsolicited diseases), history of COVID-19, history of serious allergic reactions (e.g., anaphylaxis, and systemic edema), and previous use of anticoagulant medications in the past six months; 2) COVID-19 vaccination status (types and timing of vaccination at the first and second dose); and 3) AEs following COVID-19 vaccination. Participant-reported AEs were measured to determine whether they experienced AEs, including injection site pain, fatigue, arthralgia or myalgia, headache, chills, fever, injection site swelling or redness, nausea or vomiting, menstrual disorders and unexpected vaginal bleeding, stomachache or diarrhea, rash other than at the injection site, dyspnea, mental illness, respiratory symptoms, hair loss, exacerbation of underlying disease, and other unsolicited symptoms (participants could respond by free text). If participants reported any AEs, they were requested to report the duration of each symptom and the time of onset following branching logic. Symptom severity was measured by four exclusive criteria: ‘symptoms were mild enough to not interfere with daily life,’ ‘symptoms interfered with daily life, but did not visit the hospital,’ ‘hospital visit was made, but was not hospitalized,’ ‘hospitalized including intensive care unit or had an emergency department visit.’ Severe AEs were defined as responses to a hospital visit/hospitalization due to AEs. The questionnaire in Korean is provided in Supplementary Data 2.
Outcomes
The primary outcome was the overall incidence of participant-reported AEs following mRNA COVID-19 vaccination and factors associated with AEs. To focus on mRNA vaccines, we restricted only AEs following the mRNA COVID-19 vaccine in our analyses; if a participant received ChAdOx1 nCov-19 (not mRNA vaccine) at the first dose and BNT162b2 at the second dose, AEs of ChAdOx1 nCov-19 at the first dose were excluded, while AEs of BNT162b2 at the second dose were included. We classified AEs into two categories (local and systemic) as the aspects may differ across participants’ characteristics. Local AEs included injection site pain, injection site swelling, redness, swollen lymph nodes, and lymphadenitis, while systemic AEs included other than local AEs specified above. The secondary outcome was the dose- and vaccine-type-specific odds of AEs among the sub-population of study participants. We composed a subset of the study cohort, excluding participants who had received heterologous vaccination, to minimize the potential association between heterologous vaccinations and AEs.
Statistical analysis
The overall incidence of AEs following both doses of COVID-19 vaccination was summarized into weighted proportions by the type of vaccine and sex. For baseline characteristics, we presented the median and interquartile range (IQR) for continuous variables, and frequency and proportion for categorical variables. We conducted multivariable logistic regression to identify factors associated with AEs, using the weighted odds ratio (OR) and 95% confidence interval (CI). The unit of analysis was each dose of the COVID-19 vaccination to consider multiple vaccinations from the same participants. Given that the AE types may differentially occur depending on participants’ characteristics, we constructed the regression model separately according to the types of AEs (any-, severe-, local-, and systemic-AEs vs. no AEs). The model included several demographic and clinical factors: COVID-19 vaccine types (BNT162b2/mRNA-1273), vaccine dose (first dose/second dose), heterologous vaccination, age, sex (male/female), BMI (was categorized into four groups following Asian BMI classification: underweight [< 18.5 kg/m2], normal bodyweight [18.5 to < 23 kg/m2], overweight [23 to < 25 kg/m2], obesity [higher than 25 kg/m2]),14 history of COVID-19, serious allergic reaction, anticoagulant medication use, smoking status, alcohol consumption, and comorbidities. Moreover, dose- and vaccine-type-specific odds of having different types of AEs were assessed in a subset of study participants using multivariable logistic regression. The same variables used in the primary analysis were included in the model. A two-tailed P value ≤ 0.5 was considered statistically significant. All statistical analyses were performed using SAS Enterprise Guide 7.1 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Totally 2,849 adults participated in the survey, with a median (IQR) age of 35 (27–42) years and 1,470 (51.6%) men (Table 1). Our study meets the American Association for Public Opinion Research (AAPOR) reporting guideline,15 and the survey attained a response rate of 13.8% and a cooperation rate of 66.9% under the AAPOR Response Rate Calculation. Most participants received homologous vaccination (BNT162b2 [n = 1,950, 68.4%]; mRNA-1273 [n = 617, 21.7%]) and 282 (9.9%) received heterologous vaccination. Among the cohort, 3.1% had a history of a serious allergic reaction and 1.0% used anticoagulants six-months before vaccination. A total of 50 participants reported having other diseases, including thyroid disorders accounting for the most (15 cases), followed by gout (5 cases) and gastritis/gastric ulcer (3 cases): Although Meniere’s disease, hepatitis B, anemia, ophthalmic disease, and polycystic ovary syndrome were included as well, the frequency of these conditions was uncommon.
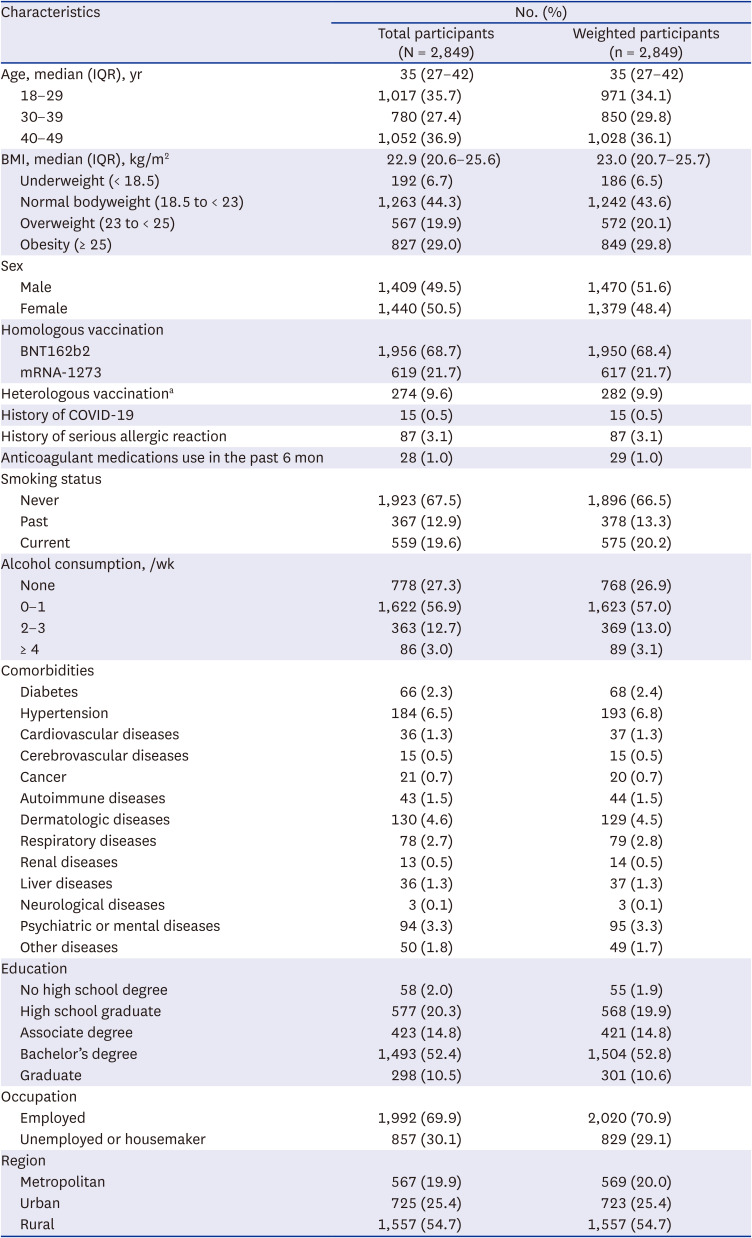
Table 1
Characteristics of COVID-19 vaccinated participants
COVID-19 = coronavirus disease 2019, IQR = interquartile range, BMI = body mass index, mRNA = messenger RNA.
aHeterologous vaccination included participants who received ChAdOx1 nCov-19 at the first dose and BNT162b2 or mRNA-1273 at the second dose, or BNT162b2 at the first dose and mRNA-1273 at the second dose and vice versa.
![]()
Among participants receiving the mRNA COVID-19 vaccine, 90.8% of the first dose and 88.7% of the second dose reported AEs; those with severe AEs were 3.3% and 4.3%, respectively (Fig. 1). The incidence of AEs following mRNA-1273 was higher than that of BNT162b2 at both doses: first dose (93.5% vs. 89.9% for any AEs; 4.8% vs. 2.9% for severe AEs) and second dose (95.0% vs. 87.0%; 5.8% vs. 3.9%) (Supplementary Table 1). The incidence of AEs was higher in women than in men at the first dose (93.9% vs. 87.7% for any AEs; 3.6% vs. 3.1% for severe AEs) and second dose (91.9% vs. 85.5%; 5.6% vs. 3.1%) (Supplementary Table 2). The most common AEs were injection site pain, fatigue, arthralgia/myalgia, headache, chills, fever, injection site swelling/or redness, nausea/vomiting, menstrual disorders and unexpected vaginal bleeding. Whereas most AEs appeared and disappeared within three-days, menstrual disorders and unexpected vaginal bleeding, and hair loss appeared mostly after seven-days of vaccination and persisted for more than three-days (Supplementary Tables 3 and 4). For the severe AEs, there were five cases of thrombosis with thrombocytopenia, four cases of myocarditis/or pericarditis, and one case of anaphylaxis (Supplementary Table 5).
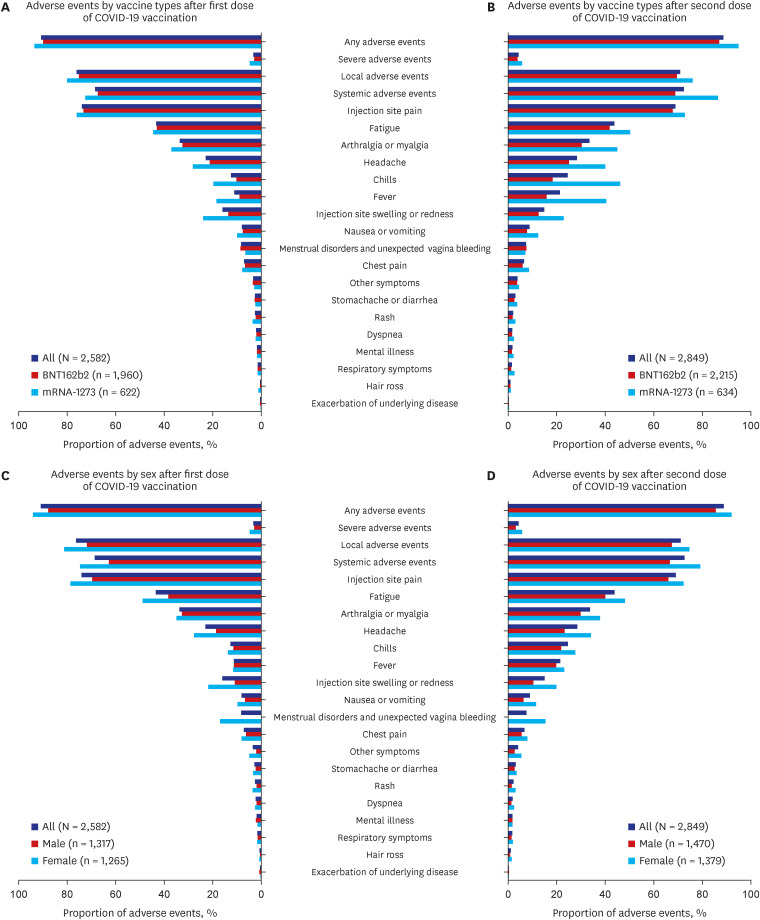
Fig. 1
Adverse events following mRNA COVID-19 vaccination by characteristics of participants. (A) Adverse events by vaccine types after first dose of COVID-19 vaccination. (B) Adverse events by vaccine types after second dose of COVID-19 vaccination. (C) Adverse events by sex after first dose of COVID-19 vaccination. (D) Adverse events by sex after second dose of COVID-19 vaccination.
COVID-19 = coronavirus disease 2019.
![]()
The factors associated with AEs and severe AEs following mRNA COVID-19 vaccination are shown in Table 2. The odds of any AEs were higher in mRNA-1273 (weighted OR, 2.06; 95% CI, 1.59–2.67 vs. BNT162b2), female sex (OR, 1.88; 1.52–2.32), older age group (OR, 1.41; 1.12–1.78 at 40–49 years, and OR, 1.27; 1.01–1.60 at 30–39 years vs. 18−29 years), and those with dermatologic diseases (OR, 2.51; 1.32−4.77); lower in the second dose (OR, 0.82; 0.68−0.98) and those with a history of COVID-19 (OR, 0.35; 0.15−0.83). The odds of severe AEs were higher in mRNA-1273 (OR, 1.67; 1.23−2.26 vs. BNT162b2), those with a history of a serious allergic reaction (OR, 1.96; 1.06−3.64), recent anticoagulant use (OR, 4.72; 1.92−11.6), and those with dermatologic diseases (OR, 2.49; 1.55−4.00).
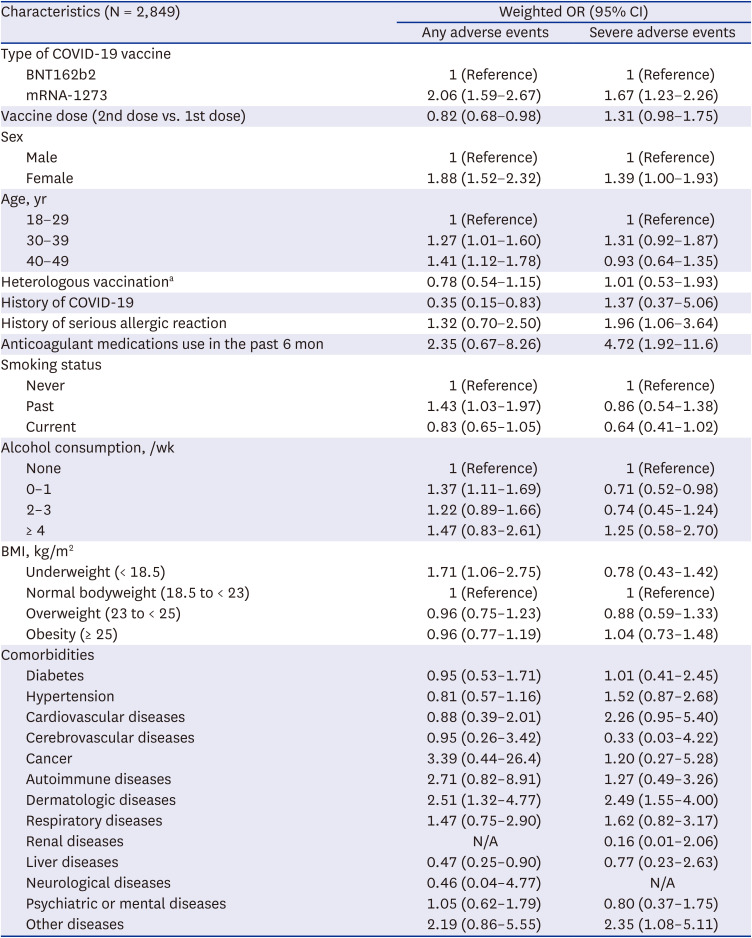
Table 2
Baseline characteristics associated with any adverse events and severe adverse events following mRNA COVID-19 vaccination
COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, BMI = body mass index, N/A = not applicable, mRNA = messenger RNA.
aHeterologous vaccination included participants who received ChAdOx1 nCov-19 at the first dose and BNT162b2 or mRNA-1273 at the second dose, or BNT162b2 at the first dose and mRNA-1273 at the second dose and vice versa.
![]()
The factors associated with local and systemic AEs after the COVID-19 vaccination are shown in Table 3. Local AEs were more prevalent in mRNA-1273 (OR, 1.37; 1.18−1.60 vs. BNT162b2), female (OR, 1.43; 1.24−1.65). The odds of systemic AEs were higher in mRNA-1273 (OR, 1.84; 1.57−2.15 vs. BNT162b2), female sex (OR, 1.71; 1.49−1.97), and patients with dermatologic diseases (OR, 1.77; 1.26−2.49) and lower in those receiving heterologous vaccination (OR, 0.73; 0.56−0.96).
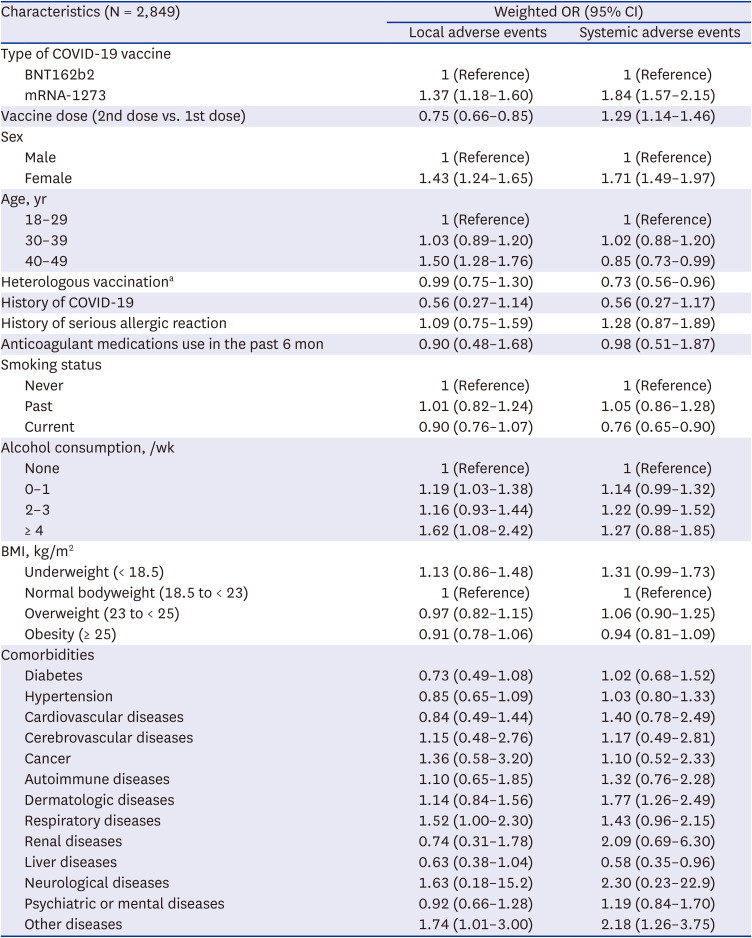
Table 3
Baseline characteristics associated with local and systemic adverse events following mRNA COVID-19 vaccination
COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, BMI = body mass index, mRNA = messenger RNA.
aHeterologous vaccination included participants who received ChAdOx1 nCov-19 at the first dose and BNT162b2 or mRNA-1273 at the second dose, or BNT162b2 at the first dose and mRNA-1273 at the second dose and vice versa.
![]()
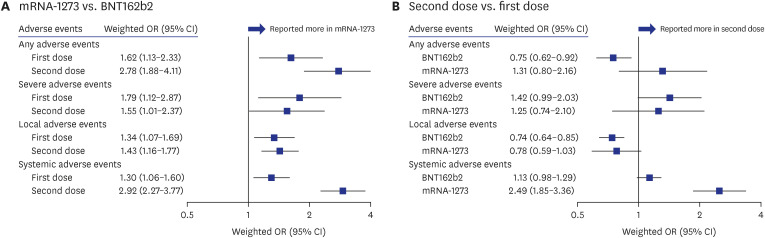
When assessing the association between the odds of AEs stratified by vaccine type (mRNA-1273 vs. BNT162b2) and dose (second vs. first), significant trends of reported AEs were observed across vaccine types and doses (Fig. 2). While all AEs were more predominant in mRNA-1273 than in BNT162b2, the odds were particularly higher for systemic AEs at the second dose (OR, 2.92; 2.27−3.77). For both mRNA COVID-19 vaccines, the incidence of systemic AEs increased at the second dose compared to that at the first dose, whereas the incidence of local AEs decreased.
DISCUSSION
Our survey revealed that 88.7−90.8% of mRNA COVID-19 vacc6ine recipients experienced AEs and 3.3−4.3% reported severe AEs after the first/second dose. The most predominant AEs were injection site pain, fatigue, arthralgia, and myalgia, similar to the results of previous studies.781617 Substantial factors, including vaccination with mRNA-1273, first dose, female sex, and dermatologic diseases were associated with AEs. Additionally, the second dose, history of serious allergic reactions, and anticoagulant medication use in the past six-months were associated with greater odds of severe AEs.
The magnitude of reporting AEs among BNT162b2 recipients was considerably smaller compared to participants in the phase-3 trials of BNT162b2. While 83% and 78% of vaccine recipients aged 16−55 years reported injection site pain after the first and second doses, respectively, in the trial,2 73.4% and 67.8% reported the same AE in this study. The proportion of individuals who reported fatigue after the first dose (43.1%) and the second dose (41.9%) was also lower than that expected from clinical trials (47% and 59%, respectively). In contrast, the proportion of patients experiencing any AEs after both doses of mRNA-1273 in this study (93.5−95.0%) was higher than that reported in the clinical trial (87.8−92.2%).3 However, considerable differences were observed in the trends of AEs compared with results from other participant-reporting studies. The UK app study showed that 13.5% (dose 1) and 22.0% (dose 2) of BNT162b2 recipients reported systemic side-effects and 71.9% (dose 1) and 68.2% (dose 2) reported local side-effects.9 In the US online cohort study, AEs were reported by 64.9% of partially vaccinated and 80.3% of fully vaccinated.10 Although the proportion of AEs was generally higher in our study, we speculated that the difference might be due to potential racial and age differences of the study cohort. As our population mainly comprised Asian heritage and younger individuals (median age of 35 years) compared with the aforementioned studies (54 years; UK study; 59−64 years; US study), contrasting trends of AEs and association of age might be observed, unlike other studies. Given that Beatty and colleagues identified that Asians are more likely to report AEs following the COVID-19 vaccine compared to Caucasians (OR, 1.49; 1.28−1.73),10 this does not preclude the association of genetic differences in AEs following mRNA COVID-19 vaccine.
Among the factors that may have an impact on AEs, the vaccine type was the most significant. Particularly, mRNA-1273 was significantly associated with higher odds of AEs than BNT162b2. These results were consistent with the findings of clinical trials,23 survey-based studies,101819 and a government-sponsored surveillance study.20 However, heterologous vaccination was not associated with AEs in this study. Clinical trials of heterologous prime-boost schedules with ChAdOx1 nCov-19 and BNT162b2 and a prospective cohort study identified no difference in reactogenicity between heterologous and homologous immunization regimens.212223 Although an inverse association between heterologous vaccination and systemic AEs was observed, this should be interpreted with caution, and further evidence on the safety of heterologous vaccination would be required.
In secondary analyses with homologous mRNA vaccine recipients for both doses, mRNA-1273 recipients had higher odds of reporting all types of AEs, regardless of the vaccine dose, compared to BNT162b2 recipients. We also found less frequent reporting of local AEs after the second dose than after the first dose in BNT162b2 recipients (OR, 0.74; 0.64−0.85) and more frequent reporting of systemic AEs after the second dose in mRNA-1273 recipients (OR, 2.49; 1.85−3.36). These results were in line with the profile of safety reports in clinical trials and previous observational studies.23924 Although the CI was wide and included the null value, the odds for local AEs after the second dose of mRNA-1273 were low compared with those after the first dose (OR, 0.78; 0.59−1.03). This was considerably different from previous findings that local AEs were also more common after the second dose than the first dose in mRNA-1273 recipients.324 Further research is needed to interpret this result.
Of the baseline characteristics, female sex was one of the evident factors associated with AEs, showing that the overall incidence of AEs in women was generally higher than that in men in this study, which was also proved by recent studies.101825 A notable finding was that over 15% of female participants reported menstrual disorders and unexpected vaginal bleeding after mRNA vaccination. Although a recent cohort study concluded that COVID-19 vaccination was associated with a small change in the menstrual cycle,26 menstrual disorders and unexpected vaginal bleeding should be carefully monitored in future booster shots. A history of COVID-19 was associated with lower odds of AEs in our study, however; in previous studies, this was not the case.102728 Since the number of participants with COVID-19 history in our study was too small (n = 15), the results might have been derived by chance. Dermatologic diseases are a potential factor associated with AEs. Specific responses to dermatologic diseases could not be identified in our questionnaire. Still, considering the representativeness of this study, it would have shown a similar trend to the common skin diseases in Korea,29 including allergic contact dermatitis, atopic dermatitis, and urticaria. A Japanese study also found that atopic dermatitis was associated with immediate hypersensitivity reactions to mRNA vaccine (OR, 5.82; 1.01−33.71).30 A cohort study reported that atopy may not be a significant risk factor for an allergic reaction to the mRNA vaccine, but this interpretation is limited by a small sample size (n = 68).31 It is known that defects in the epidermal barrier function accelerate sensitization to allergens following dermal exposure.32 Thus, individuals with dermatologic diseases are likely to experience hypersensitive reactions to the COVID-19 vaccines.
For severe AEs, a history of serious allergic reactions and recent anticoagulant use were significantly associated factors. According to a study analyzing the Vaccine Adverse Event Reporting System database, allergy history was more common in vaccine recipients with anaphylactic reactions than in those without (64.9% vs. 49.6%, OR, 1.88).8 Another cohort study also found that a history of high-risk allergy was highly associated with an increased risk of allergic reactions after mRNA COVID-19 vaccination (relative risk, 2.46; 1.92−3.16).33 With respect to recent anticoagulant use, as the number of participants who administered anticoagulants was small, experiences of severe AE in those participants could have a significant impact on the result. In light of the fact that the current COVID-19 vaccination guidelines do not specify contraindications in relation to the indication of anticoagulants and that vaccination can be performed if the anticoagulant user’s treatment status remains stable, the possibility of chance finding cannot be ruled out in this study. However, given the negative effect on anticoagulation control following BNT162b2 inoculation was reported recently,34 continuous monitoring should be needed to be tailored to those populations who were prescribed anticoagulant medication.
Our results should be interpreted with caution given the following limitations. First, there might be potential misclassification of outcomes, as AEs reported by the participants were not medically reviewed. However, we attempted to determine the solicited AEs mainly based on the symptoms experienced by the participants, not medical jargon, focusing on patient-reported outcomes. Second, recall bias from participants who experienced AEs and the heterogeneous characteristics between participants and non-participants may have biased the results due to the nature of the survey-based study. Enrolled participants may have responded to the survey because they experienced symptoms, whereas those who did not experience symptoms were likely to not be interested in completing the survey. Third, the possibility of chance finding cannot be ruled out due to the limited number of participants in this study. Fourth, despite our effort to enhance the representativeness of the sample by stratified sampling and weighting, our study participants might not reflect the overall Korean population. Lastly, as we only examined the short-term safety of mRNA vaccines, further studies are required to evaluate the long-term AEs.
In conclusion, this nationally representative survey revealed that approximately 90% of mRNA vaccine recipients aged 18−49 years reported AEs, however, most AEs were mild and transient. We also found that vaccination with mRNA-1273, female sex, and dermatologic diseases were associated with participant-reported AEs. Additionally, a history of serious allergic reactions and anticoagulant use were significantly associated with greater odds of severe AEs. So far, public health authorities provided information on mRNA vaccines-related frequently reported AEs and their magnitudes, but rarely focused on differences in AEs by vaccine type or dose and risk factors to AEs. We believe that this study generated more enhanced evidence that can be used to update the guidance. Moreover, considering that COVID vaccination might become an annual shot, our findings may aid policymakers and physicians in establishing future vaccination strategies tailored to individuals potentially susceptible to AEs.
 XML Download
XML Download