

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
End-of-life care is a complex domain stirring intense emotions. Many healthcare professionals experience moral distress while caring for critically and terminally ill patients. Moral distress has several definitions but is mainly understood as “negative feelings that arise when one knows the right things to do, but institutional constraints make it nearly impossible to pursue the right course of action.”123 Healthcare professionals experience moral distress when they provide futile treatment or work in a poor environment with inadequate resources and unethical behaviors.4 Tertiary hospitals in South Korea are focused on life-saving or life-prolonging treatment; hence, physicians and nurses tend to consider end-of-life care as a treatment failure.56 Under these circumstances, healthcare professionals who are engaged in end-of-life care typically face a lack of resources and leadership. This negligent atmosphere surrounding end-of-life care worsens healthcare professionals’ moral distress.
Previous studies in South Korea have examined the moral distress of nurses in end-of-life care; however, only a few studies have dealt with moral distress among medical students and physicians.789 For instance, Moon et al.9 showed that job stress affected doctors who provided end-of-life care. However, to the best of our knowledge, no study has attempted to compare the moral distress of nurses and physicians. To address the similarities and differences between physicians and nurses, we investigated their experiences of caring for critically and terminally ill patients in tertiary hospitals. Most physicians and nurses work as a team to provide end-of-life care. Unfortunately, differences in attitude, knowledge, and understanding can widen communication gaps, leading to failure in providing high-quality care. Thus, this study focused on how working environments cause disparity among physicians and nurses, hindering mutual understanding between the two disciplines.
METHODS
This study was part of a project to explore the moral distress involved in critical and terminal care in acute settings before the enforcement of the Act on Decisions on Life-Sustaining Treatment for Patients in Hospice and Palliative Care or at the End of Life (the Act on Decisions on Life-Sustaining Treatment) in 2018.10 Since this study was conducted in 2017, it reflects the situation pre-coronavirus disease 2019 (COVID-19) pandemic.
Semi-structured in-depth interviews were conducted. Physicians and nurses who had experienced moral distress when caring for terminally ill patients were recruited from two tertiary hospitals in South Korea. To embrace diverse perspectives and experiences, this study used purposive maximum variation sampling.1112 A total of 22 participants were recruited through advertisements posted on bulletin boards in both hospitals and an online bulletin board in one of the hospitals. Written informed consent was obtained from all participants.
The interviews started with a question regarding a case that the participants occurred when they saw the recruitment announcement, followed by key questions. By starting with their personal experience, the participants were able to freely explore the situations that caused them moral distress. At the start of the interview, the interviewer asked the participants about their primary moral concerns and burdens, such as “Have you experienced any ethical concerns or moral conflicts while caring for a critically and terminally ill patient?” and “Did you feel any physical or psychological burden because of these moral conflicts?”
The raw data collected from the project was analyzed. While the first article10 focused on the values that both physicians and nurses considered in terms of moral distress, this study analyzed the raw data focusing on the differences between physicians and nurses. The recorded interview files and memos were transcribed and transferred to MS Word files and analyzed using grounded theory13 using the qualitative research software MAXQDA. Three research team members repeatedly read the transcribed manuscript and then coded, classified, and structured it. The coded output was reviewed under the supervision of the other research team members and an external expert in nursing-related qualitative research. The first and second reviewers extracted the code from the manuscript with the question, “What is the main theme of moral conflict and how did participants recognize and resolve them?” Subsequently, the third set of reviewers confirmed the structured codes based on the manuscript. The other research team members reviewed the coded results and gave more concrete insights. Through these multiple rounds, all members from diverse positions and backgrounds examined the transcriptions and code structures reflexively; we believe this process reduced the bias of results.
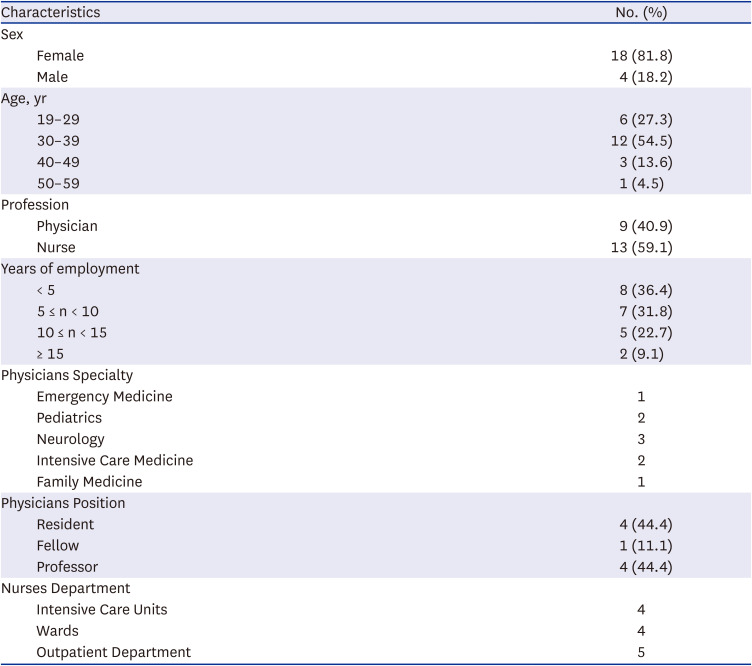
The interviews were conducted between February and May 2017, and each interview lasted 60–90 minutes. A total of 22 people were interviewed, nine (40.9%) of which were physicians and 13 (59.1%) were nurses. The physicians were recruited from various disciplines, including emergency medicine, pediatrics, neurology, intensive care medicine, and family medicine. The staff as well as the residents and fellows joined the study. The nurses who participated also came from different working environments, including intensive care units (ICUs), wards, and outpatient departments. The demographic characteristics of the interviewees are summarized in Table 1.
Table 1
Demographic characteristics of the study participants (n = 22)
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Hospital and Seoul National University Bundang Hospital (No. 1612-071-813). Accordingly, all participants were informed about the purpose and methods of the study, and written consent was obtained prior to their participation.
RESULTS
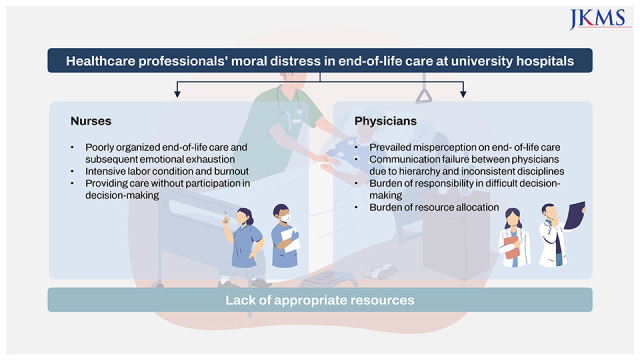
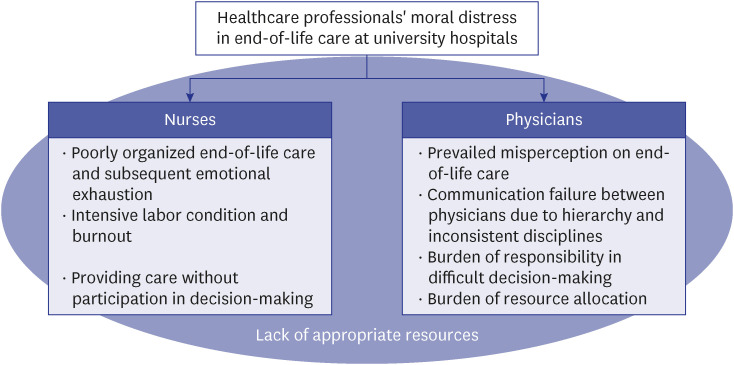
Both physicians and nurses who participated in this study reported that they had frequently encountered ethical conflicts among patients and their families. They struggled owing to a lack of appropriate resources in end-of-life care which caused negative feelings such as anger, powerlessness, emotional burdens, and skepticism. Regardless of the common features of end-of-life care experiences that the physicians and nurses reported, the causal factors and contexts of the cases that gave rise to moral distress differed.
Nurses mainly addressed poorly organized end-of-life care, intensive labor conditions without support for nurses, and providing care without participation in decision-making. Meanwhile, physicians addressed the prevailing misperceptions on end-of-life care, communication failure between physicians owing to hierarchy and fragmented disciplines, the burden of responsibility with making difficult decisions, and the burden of resource allocation.
These aspects of moral distress that the nurses and physicians addressed are hereinafter discussed, and are summarized in Fig. 1.
Nurses
Poorly organized end-of-life care and subsequent emotional exhaustion
Overall, the interviewees considered the life-sustaining treatments meaningless and harmful to patients at the terminal stage in that these interventions provide no benefit to patients and prolong their period of suffering. As healthcare professionals who cared for the patients and closely observed the progression of the disease and their bodily reactions, the participants did not consider life-sustaining treatment as the best option. Rather, they wondered “if this patient is still here with us,” (ID 28. Nurse, Emergency intensive care unit [EICU]) and hoped that “the patient would go home and have the good dinner they wanted” (ID 34. Nurse, Internal medicine ward). Furthermore, they “felt so sorry for the patient who suffered from extreme pain” (ID 20. Nurse, Oncology ward).
The participants addressed that end-of-life care in tertiary hospitals was poorly organized. Since this study was conducted right before the introduction of the Act on Decisions on Life-Sustaining Treatment, all the participants mentioned that the withdrawal of life-sustaining treatment was “illegal.” Thus, they reported that withholding treatment was the main way of stopping such meaningless treatment. One nurse remarked that:
“Doctors say that you cannot remove the machinery respirator once it is already put in because it is illegal. [If the patient’s family agreed to stop life-sustaining treatment] we do not raise the vasopressor [instead of removing the respirator]. We would maintain the current treatment, such as maintaining the amount of vasopressor [but would not increase it or start another treatment].” (ID 28. Nurse, EICU)
As some participants explained, in the circumstance where explicit withdrawal of life-sustaining treatment was believed as an illegal practice, a Do-Not-Resuscitate order (DNR) was believed as the only means to prevent a patient from suffering “meaningless” life-sustaining treatment. Yet, participants addressed the difficulty of initiating end-of-life care conversations with the patients’ family members.
“It is so hard to talk about DNR to patients and their families. You have not died. You still walk around even though you are at the terminal stage. In this situation, if you are asked what you would do in an urgent event, you would be frightened; ‘Am I in such a bad status?’ This is why it is hard to obtain a DNR.” (ID 19. Nurse, Oncology ward)
Moreover, some participants reported several cases wherein cardiopulmonary resuscitation and mechanical ventilators were applied to the patients against their will because one family member insisted on “doing everything” or because none of the family members were present. Participants thought this practice as a mere cover-up. In some cases, the DNR was not delivered to the medical staff during the transfer process. Many participants, however, found that they were not in a position to initiate end-of-life care conversations or mediate with the stakeholders.
For participants, the room for the dying, called the imjongbang, represents the poor integration of end-of-life care into the acute care setting. The room for the dying is reserved for patients who would pass away in the hospital when they could not be transferred to the hospice. However, most nurses viewed this room as a place where only aggressive treatments were withdrawn without proper end-of-life care.
“It is explained that this place is for a good death that all family members spend a last time with the patient… and that medical staff would not do an invasive treatment to a patient in this room. However, often times, some family members complained that we do nothing to the patient… Conversely, in some cases, the patient’s family asked why we did not stop providing oxygen… But the hospital does not allow natural death without any intervention.” (ID 19. Nurse, Oncology ward)
“From the perspective of the family members, they feel abandoned without any care. They would think that we do not check on the patient’s blood pressure or give medication or oxygen although we meant to stop the meaningless life-sustaining treatment.” (ID 20. Nurse, Oncology ward)
Even after being moved to the room for the dying, families may expect physicians and nurses to monitor patients’ vital signs and give them some medications to make them comfortable. Participants thought that this was against the purpose of end-of-life care; nevertheless, they felt guilty for disappointing the patients and family members and felt that they failed to provide the care that patients and their families would need.
While taking care of terminally ill patients and encountering patient deaths, participants frequently experienced intense emotional exhaustion. For example, one participant who worked in the neonatal ICU narrated a neonate’s death, which caused her great emotional distress.
“I could not help but think of the baby. It [the baby’s death] hurt the nurses, too. We all cried when she passed away. Since the event, I try not to become attached to the severely ill baby but it makes me feel guilty.” (Nurse A, ICU)
Similarly, many other participants reported events that made them determined “not become attached to patients” because they were hurt by the patient’s death. Another participant also confessed that she quit working in the wards owing to psychological distress. Participants were trying to find a way to protect themselves from sadness and helplessness; detachment often appeared as a solution, but they felt guilty as well.
Intensive labor conditions without support for nurses and burnout
Most participants raised concerns regarding the working environment, wherein it was hard to “find a chance to go to the toilet” (ID 27. Nurse, Hematology ward) and to “have time to grab something” (ID 34. Nurse, Internal medicine ward). The three-shift system and the number of patients assigned per nurse also exacerbated their labor conditions. One participant said that:
“Because patients flood into the emergency room (ER)… You try to manage to take care of the patients admitted… You only have two hands but you need to do so many things to the patients, and even some of them get worse.” (ID 28. Nurse, EICU)
Owing to overloaded work, it was hard for the participants to care for patients and their families with compassion and to find a meaning for end-of-life care. One participant encapsulated it as “We do not have time for the patients and their families. We do not have time to listen to them” (ID 23. Nurse, EICU). Another participant said, “You should think about ethics, of course, but you don’t have room to think about it” (ID 34. Nurse, Internal medicine ward). Participants reported that taking care of a patient at the terminal stage and a dying patient often meant an additional burden to their already-overloaded work in that this task required more procedures and paperwork. Some participants confessed that they often wished to avoid taking care of a patient in a severe condition.
“Let’s say, a patient passes away at 2AM. Only a few staff work in the ward, and they take care of everything such as writing the documents, changing clothes, and returning the medication. For an extubation, you call an intern because it is their job, but the intern does not get the call while sleeping. You also need to write everything in the EMR (electrical medical records) to hand over to the nurse in duty the next morning. Taking care of a dying patient requires so many work.” (ID 34. Nurse, Internal medicine ward)
“Honestly, it is your work. Doing your best to a patient who gets worse means more medications and more machines. It means an emergency. I can’t tell you that it is not stressful.” (ID 28. Nurse, EICU)
However, participants clearly recognized that the intense workload hampered their realization of a sincere end-of-life care; they felt that it was morally incorrect to consider taking care of a dying patient merely as a burden. Some participants had feelings of guilt, as if they dehumanized their patients; they attempted to strike a balance between preventing themselves from experiencing emotional burn out and providing humane care, which was not easy.
“It is hard… You would be exhausted if you try to embrace all patients and listen to all of them, but you would be too technical if you treat the patient without a heart.” (ID 27. Nurse, Hematology ward)
Some participants highlighted the absence of emotional support for nurses, which exacerbated their working environment. In addition to the emotional labor and psychological distress that originated from taking care of critically and terminally ill patients, nurses reported that it is difficult for seniors and newcomers to help each other in a battlefield-like work environment due to hierarchical relations.
“They say, ‘Be nice to patients. Be nice to newcomer nurses.’ What about us in the middle? Am I supposed to only work without any support and care?” (ID 27. Nurse, Hematology ward)
Participants did not feel that the hospitals support them; one interviewee said: “I don’t see any effective measure to support the nurses. I think we need a system to take care of the nurses practically rather than merely formally.” (ID 5. Nurse, Outpatient department)
Providing care without participation in decision-making: being caught in between the physician and patient
With regard to the physician-nurse-patient relationship, the participants raised that they were caught in the middle of physicians and patients. According to the participants, nurses carry out doctor’s orders and take care of patients at the bedside. However, since nurses did not participate in the decision-making process, participants often had to perform the physician’s orders even if they did not consider it the optimal solution or believed that the family member’s decision is against the patient’s will. Some participants experienced an inner conflict since they were supposed to persuade patients to participate in a treatment and trial that they did not consider efficacious.
“Attending doctors tend to tell the patients only the bright side of the treatment… It is the nurse who explain the rest of it to the patients. Even though the patients would go through the side effects without any positive reaction to the treatment, we are supposed to encourage the patients to take part in the treatment.” (ID 3. Nurse, Outpatient department)
Many nurse participants pointed out that nurses were not in the position to share their own opinions to physicians and patients. For example, one nurse remarked that:
“Sometimes, patients asked us what we thought about the doctor’s suggestion, like, ‘The doctor said that I need to prepare for my ending, and I would like to know what you think.’ I cannot say ‘No, you will be fine’ though. The doctor must have a reason why he or she said that. I feel like being put in an awkward position.” (ID 1. Nurse, Outpatient department)
At times, some participants experienced that they had to explain the details of the treatment process to the patient on behalf of physicians. This is the case in a tertiary hospital in South Korea, where the quality of communication between physicians and patients was low owing to the so-called “three-minute-consultation.”
“When it seems that the talk would be prolonged, doctors would look at us, and we would tell the patient, ‘I will explain it outside the office.’ I would think, ‘Am I a doctor?... Isn’t this a doctor’s job?’” (ID 1. Nurse, Outpatient department)
In particular, when a physician did not conduct a complete end-of-life conversation with the patient and a nurse took over the task, participants felt overwhelmed.
Physicians
Prevailing misperceptions on end-of-life care
Participants agreed on the necessity of end-of-life care. However, the transition from an active treatment to end-of-life care did not go smoothly in their case. In general, the expected primary role of doctors involve curing diseases and saving a patient’s life, and the trainings in medical schools and hospitals focus on these missions. All the participants answered that the professional training in a medical college did not cover how to initiate end-of-life care discussions and how to take care of patients at the terminal stage. Furthermore, some participants mentioned an implicit idea shared by physicians that viewed obtaining a DNR as a sign of treatment failure and negligence of duty. One resident remarked:
“I was told by my senior that an internal medicine professor admonished residents for obtaining a DNR, saying that they did it because they didn’t want to do their job. This means that the professor regarded a DNR as abstaining from further treatment.” (ID 12. Physician, Family medicine)
“If it is concluded that there is nothing to do for the patient but the patient does not die soon… the attending doctors do not come to round often.” (ID 42. Physician, Neurology)
Once a patient was at the terminal stage and was receiving end-of-life care, some participants felt that attending doctors in the teaching hospital setting were no longer interested in the patient. In these cases, obtaining a DNR was regarded as “doing nothing to a patient,” that is, a giving-up on the patient. In the atmosphere in which a transition to end-of-life care was considered as a failure of medicine and an abandonment of a patient, participants reported that the initiation of palliative and hospice care was delayed until “near death” (ID 12. Physician, Family medicine).
Also, some participants experienced psychological distress such as feelings of guilt when they are faced by their patient’s death. One participant remarked: “Doctors think they fail when their patients die even if the death is not their fault.” (ID 40. Physician, Pediatrics) Another participant also shared an anecdote wherein her patient had got worse rapidly after her delivery of bad prognosis, and added: “You feel guilty, thinking ‘I became a doctor to save a life, not to kill someone. Am I making this patient die by not doing any treatment?’” (ID 12. Physician, Family medicine)
Communication failure between physicians due to hierarchy and inconsistent disciplines
The hierarchy within physicians was pointed out by the participants. In the hospital system, residents are supposed to perform their attending doctor and senior resident’s decisions even if they do not agree with them. One participant (ID 42. Physician, Neurology) recalled a past anecdote that he had wanted to try using clotbuster to a stroke patient with cancer at the terminal stage but had to follow the senior resident’s decision not to. Although they thought that residents tended to look after patients more intimately and to have more chances to talk with patients and their families than attending doctors, participants reported that it was hard to actively participate in decision-making conversations and present their opinions either to the attending doctors or the patients and their families. One participant said:
“Even if I think that this treatment would be meaningless, I cannot tell the patient… How can I do that in a situation where you did not reach an agreement with your attending doctor?... It is hard to talk with your attending doctor about the initiation of end-of-life care because they are busy and because they put cure as a top priority.” (ID 12. Physician, Family medicine)
Moreover, many participants highlighted that different treatment goals and roles of medical disciplines often raised conflicts over end-of-life decisions. Each discipline may have heterogenous primary values and attitudes on a proper timing to transition to end-of-life care and life-sustaining treatment. For instance, according to participants, physicians in the ICU would think that physicians in the ER tended to intubate a patient with terminal-stage cancer, which would not be beneficial; Physicians in the ER would complain that oncologists tended to avoid the end-of-life care plan so that the ER staff had to suggest writing a DNR order to the patient, with whom they had no rapport relationship. One participant (ID 21. Physician, ICU) also provided an example that the idea on whether antibiotics should be applied to a patient in the terminal stage might be different between the infectious disease and oncology divisions. Even for the same patient, each specialty expresses different opinions, and they do not communicate with each other to solve the disagreement. This inconsistency leads to physicians being unable to make clear decisions about life-sustaining treatments and patients being exposed to unnecessary decision burdens.
Burden of responsibility in difficult decision-making
Most participants expressed their burden of responsibility in the decision-making process. First, many participants thought that the line of irreversibility, i.e., the criterion of terminal stage and end-of-life, would be often unclear. Participants reported that there were some cases wherein “the patient became better and fully recovered” (ID 21. Physician, ICU) even when a patient seemed hopeless at first sight to the physicians and the family members of the patient.
Second, there was not enough time to consider what the patient would wish and to discuss on care plans with the family members in an emergency. Participants felt stressed when making hard decisions as they could not predict the progress of the disease accurately. One described an urgent situation wherein both withholding treatment and performing the treatment have a high risk:
“It is recommended that a critical decision be made when all the family members of a patient gather, but in neurology there is no time to do that. You have to do the surgery within three hours and cannot wait for the family members to come. That would be unrealistic in the clinical setting participant.” (ID 8. Physician, Neurology)
Third, many participants considered the quality of life that the patient and their family members would go through. In line with the point that irreversibility may not be clear as much as it is presupposed, some participants, particularly in pediatrics and neurology, pointed out cases wherein a treatment could make a patient bed-ridden for a long time. These situations did not fit the definition of terminal stage and end-of-life care, but they imply that a boundary for end-of-life care should be considered in a spectrum of the whole treatment journey. One participant reported that:
“In some cases of children patients, as the medicine has advanced, we can make them live without problems of breathing, heart, and lung. Just they would lie in bed forever… [Unlike in the case of adult patients,] only the mothers took care of every burden… The family would be devastated, but there is no hope for recovery… I doubt if it is right to do tracheostomy and PEG to keep the children and their family in the situation, but it does not make sense not to do the procedures, either, from a doctor’s perspective.” (ID 41. Physician, Pediatrics)
Most of all responsibility of decision making was linked to liability. This was partly because this study was conducted right before the Act was enforced. Most participants feared that a kin of a patient who did not participate in the decision making would result in a lawsuit against physicians. The Boramae Hospital Case was mentioned by several participants as a ground to press on with life-sustaining treatment that a patient would not want to receive or that the physician found no benefit in. In particular, they thought that the hospital system would not protect them from the lawsuit.
Burden of resource allocation
Being assigned limited medical resources for patients was also raised by the participants in line with the physician’s responsibility. In the participants’ recount, the allocation of beds was one of the most critical challenges. As one participant (ID 21. Physician, ICU) remarked, the beds in ICUs, ERs, and wards in tertiary hospitals “did not exist for one individual patient” and the physicians were supposed to consider the fair use of the beds in a way that served the purpose of the place. Yet, they often found that resources were limited for patients in the terminal stage. One participant who worked in the ER reported a case wherein she had to decide which of the two cancer patients in the terminal stage had to be hospitalized or transferred because the oncology ward had only one bed while the ER had no bed. Recalling the case, she confessed that she had thought, “I would go to hell,” after making the decision. The participant remarked:
“Oncologists would want us to hold up their patients in the ER until they find a bed in the ward, but the ER staff cannot do that. If over 3% of ER patients stay here more than 24 hours, the national budget for the ER would be cut back. Oncologists would blame the ER staff for sending the critically ill patients to other hospitals and making their health status worse.” (ID 11. Physician, ER)
In addition to the specific raison d’etre of each department, participants pointed out that the hospital system pressed them to increase the bed turnover rate. Even though participants would like to let their patients stay in the ward for full support, they felt a pressure to discharge the patients “who need a lot of care for a long time” as quickly as possible so that the medical resources could be utilized in an “effective” way. In the case of tertiary hospitals that time was limited, participants were not able to communicate adequately with the patients and their family members to convince them of the reason for the transfer and discharge, particularly when the patients and their families wanted to receive any kind of treatment. Consequently, they were often confronted with the patients and their family members’ complaints.
“They would say, ‘I do not care. Just fix my problem.’ We have only one single room in the ward, and you imagine that three patients insist on taking the single room. At times, they would be very aggressive to the medical staff and we cannot help but embrace the situation.” (ID 40. Physician, Pediatrics)
In sum, participants recognized that personnel, spatial, and temporal resources were limited for critically and terminally ill patients in tertiary hospitals; this made it difficult to provide them with good care while the burden of decision-making is often placed on the individual physicians.
DISCUSSION
During conflicts on end-of-life care, healthcare professionals experience various types of moral distress.1415 The results of this study were largely in line with previous studies. Several studies have demonstrated that nurses in ERs, ICUs, and internal medicine wards showed a high level of moral distress;161718 meanwhile, physicians experienced a sense of failure, frustration, depression, and sadness while taking care of critically and terminally ill patients.9 This study also found that all participants experienced moral distress.
The common features that both physicians and nurses addressed are marginalized end-of-life care and a lack of appropriate resources in acute care settings. Both did not regard life-sustaining treatment as a beneficial option for their critically and terminally ill patients and wished for them to get good quality of end-of-life care. However, tertiary hospitals did not structure the timing of end-of-life care discussion properly or offer the patients personnel, spatial, and temporal resources for end-of-life care. Rather, once a patient was converged to the terminal stage, they were considered resource-consuming and labor-intensive, and were supposed to leave to other institutions as quickly as possible. Also, the end-of-life discussion failed to include those who participated in providing care, especially the nurses and residents. Only when people accept death as a part of life and recognize the need for end-of-life care can conversations regarding end-of-life care begin.192021 However, this study revealed that healthcare professionals often did not agree upon the meaning and timing of end-of-life care; furthermore, systematic education on palliative and hospice care was not conveyed to them. Although lectures and conferences for end-of-life care are occasionally provided for physicians and nurses by a hospital, there are no mandatory structured programs on it. In this institutional setting, the physicians and nurses often experienced feelings of helplessness, frustration, and guilt.
This study reveals the different factors that caused moral distress to nurses and physicians in explicit ways. Nurses are those who take care of patients intimately. Nevertheless, the nurses in this study did not actively participate in the end-of-life care conversation but performed as per the doctor’s order. This position facilitated their emotional exhaustion. In addition, the nurses worked in an environment wherein end-of-life care with compassion22 could hardly be realized owing to institutional barriers23 and overloaded work.24
Conversely, the physicians were more affected by the burden of decision-making and resource allocation, which would impact the quality of life of patients and their families and the overall medical expenses.25 In general, it is regarded that physicians possess authority in treatment and take responsibility for end-of-life care decisions. However, the physician participants also experience emotional distress during end-of-life care due to conflicts in their contradictory roles and insufficient resources.262728 The physicians were often pressed to decide against their intentions and felt that the burden of decision-making fell on the individual physician.
These different aspects of moral distress can be explained by the difference in moral positions. In particular, physicians decide upon the treatment and take the responsibility while nurses live with the decision.29 It can be interpreted that the physicians’ experience of end-of-life care would be a “moral dilemma” and that of nurses would be a “moral distress.”
Regarding hierarchy within the hospital structure, both physicians and nurses recognized that the hierarchical relations caused unfair distribution of workloads. Some studies have shown that hierarchical relations may deepen moral distress toward end-of-life care.229 Along with previous results, hierarchical relations were a major cause of moral distress in this study, which can widen communication gaps. Compared with nurses, who were distressed from the unfair burden between physicians and nurses, most physicians appealed to conflicts between staffs, residents, and specialties. The differences in morality were reflected in the participants’ main narratives, even though physicians and nurses shared the same problems, such as hierarchical relationships and a lack of resources and support.30
Caring for terminal ill patients can give rise to negative emotions and distress among healthcare professionals in university hospital settings. Since tertiary hospitals in South Korea have been recognized as institutions for life-saving treatments for severe illness, end-of-life care has been systemically neglected and remained marginal; thus, it would seem hard to resolve end-of-life care and moral distress. However, it has been recently argued that moral distress can be recognized as a moral investment to reform the clinical environment,3132 Furthermore, moral distress consultations can help improve the staff’s situation and empower them even though it does not resolve moral distress itself.33
Drawing upon the results of this study, we suggest the necessity of a well-integrated end-of-life care in a tertiary hospital. This includes providing guidelines as well as an inclusive atmosphere for an end-of-life care conversation, which offers more personnel, spatial, and time resources for patients in the terminal stage and provides education regarding palliative care. The institutional support for physicians and nurses who are involved in critical and terminal care is also needed. This support should reflect the different roles and positions of physicians and nurses so that moral conflict and communication failure can be reduced.
In conclusion, this study was part of a project that was designed to investigate the moral distress involved in caring for critically and terminally ill patients in South Korea before the introduction of the Act. We demonstrated that healthcare professionals believed in: 1) minimizing meaningless interventions during the terminal stage, 2) letting patients know of their poor prognosis, 3) saving lives, 4) offering palliative care, and 5) providing care with compassion to be right for the patients in the previous article.10 This study revealed the differences between the moral distress experienced by nurses and physicians. Since this research was conducted right before the Act on the Decision on Life-Sustaining Treatment was enforced, these two studies can provide a good reference point to compare the situation before and after the enforcement of the Act and to assess the Act’s consequences. In addition, this project was completed before the COVID-19 pandemic. Future studies that investigate how this pandemic has changed the landscape of end-of-life care in acute settings in South Korea are needed.
We demonstrated severe and complex features of moral distresses among physicians and nurses in tertiary hospitals in South Korea. Moral distress can interrupt communication between healthcare professionals and cause isolation. It also intensifies conflicts in end-of-life care. As a team responding to terminal care situations, physicians and nurses should understand moral distress in a mutual sense and trust each other.
 XML Download
XML Download